
Abstract
This paper explores the connection between alcohol-related mortality, drinking behavior, and macroeconomic conditions in Finland using both aggregate and microlevel data from recent decades. The aggregate data reveal that an improvement in economic conditions produces a decrease in alcohol-related mortality. Microlevel data show that alcohol consumption increases during economic expansion while the probability of being a drinker remains unchanged. This demonstrates that alcohol-related mortality and self-reported alcohol consumption may be delinked in the short-run business cycle context. One explanation for this paradox is that most harmful forms of drinking are not captured in survey-based data used to study the effect of macroeconomic conditions on alcohol consumption. Our evidence does not overwhelmingly support the conclusions reported for the United States that temporary economic downturns are good for health.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Macroeconomic conditions matter for health. This issue has led to a body of literature that has produced mixed findings (for a summary see [24]). Initial empirical studies based on time-series analyses revealed a positive relationship between measures of health and economic conditions [1, 2, 3]. Several authors, however, noted that these studies suffer from serious technical problems [8, 26, 28]. Analyses that try to control for the shortcomings have usually failed to find a consistent relationship between health and economic conditions [7, 10, 15]. Recent studies from developed countries have, surprisingly, found a negative relationship between economic conditions and health [20, 21, 22, 23, 24]. These studies report out that mortality declines in periods of economic slump.
The observed correlation between macroeconomic conditions and health arises from changes in individuals’ health behavior [23]. Some of the recent studies have therefore analyzed individual microdata [23, 25]. In particular, drinking seems to decrease during temporary economic downturns. Ruhm and Black [25] argue that this pattern arises owing to the decline in alcohol use among existing drinkers rather than from the movement into and out of drinking. In particular, they point out that heavy drinkers drink less during economic downturns. However, it is difficult to capture abusive drinking directly linked to mortality by using survey-based information on alcohol consumption. Interestingly, Dee [6] reports that binge drinking, i.e., the consumption of large amounts of alcohol on the same occasion, is strongly countercyclical. Such a finding supports the hypothesis that drinking, at least binge drinking, is used as a form of self-medication in time of psychological stress during economic downturns.
There has been extensive research on socioeconomic differences in mortality in Finland. Perhaps the most well-known paper in this literature is that of Martikainen and Valkonen [13]. In addition, there has been research concerning alcohol-related mortality (e.g., [14, 17]). These studies, however, generally focus on differences in mortality between socioeconomic groups and do not examine the effect of macroeconomic conditions on alcohol-related mortality. Closest to our investigation is a study by Mäkelä [18] who analysed the relationship between alcohol-related mortality and aggregate economy in 1987–1995 using register-based data from Statistics Finland. Mäkelä [18] reported that alcohol-related mortality increased during the economic boom in the late 1980s and decreased slightly during the recession of the early 1990s. In addition, Jäntti et al. [11] discovered by exploiting Finnish municipal data from 1987–1994 that regional unemployment was not associated with an increase in overall mortality during a period of rapidly increasing unemployment. One possible way to interpret this finding is to say that during the early 1990s the welfare state managed to insulate the population against rising unemployment having a negative effect on health.
This contribution focuses on the relationship between alcohol-related mortality, drinking and macroeconomic fluctuations in Finland. We use both aggregate data on alcohol-related mortality and microlevel data on alcohol consumption during recent decades. Importantly, alcohol-related mortality is an unambiguous indicator of abusive drinking that captures the social costs of macroeconomic conditions. In particular, it has been shown that changes in drinking produce a rather immediate effect on mortality. This was first demonstrated during the Second World War in France, where there was an almost immediate drop in the number of alcohol-related deaths as consumption of alcohol decreased drastically (e.g., [5]). As we use both aggregate data on alcohol-related mortality and microlevel data on drinking, we are able to examine the connection between these.
The relationship between drinking and macroeconomic conditions is complex because many factors at work at the same time. For instance, drinking may decrease during slumps because persons have less money to spend on alcohol along with other items of consumption (e.g., [25]). In addition, there may be less work-related stress during economic downturns, which induces less drinking among those who work. On the other hand, unemployment, which typically soars during slumps, may stimulate consumption of alcohol among unemployed persons. The present analysis does not attempt to distinguish the different effects that may have an effect on drinking. The goal of this contribution is more modest: we aim to provide an overall picture about the underlying connection between alcohol-related mortality, drinking, and macroeconomic conditions based on the data sets that are well suited to give an answer to this question.
By investigating the effects of macroeconomic conditions on alcohol-related mortality and drinking in Finland, we seek to increase the understanding of these matters in several ways. First, these matters have not been investigated in Finland before, and it is not clear whether the findings from the United States on alcohol-related mortality and drinking are valid globally. In particular, there was an extreme economic downturn in Finland during the early 1990s. The national unemployment rate rose very rapidly from 3% to 17%. This makes it possible to investigate the effect of an unusual economic crisis. In addition, the high alcohol tax in Finland makes alcohol relatively expensive. Then, given a decline in the income level caused by recession, drinking may be expected to decline more in Finland than in a country with lower alcohol taxes. Second, this study examines the relatively large regional differences in economic outcomes and health in Finland. In this respect the analysis complements and expands on earlier studies of regional health differences in Finland (e.g., [27]). Uniquely for Finland, we incorporate the effects of macroeconomic conditions in the analysis. In particular, the prevalence of wide regional disparities is helpful in identifying the effects of macroeconomic conditions. Third, we provide evidence on the issue based on both aggregate data on alcohol-related mortality and microlevel data on drinking. Until now it has been common to use either aggregate data or microlevel data.
After describing the data sets used in this analysis we introduce the empirical strategy for identifying the effect of macroeconomic conditions on alcohol-related mortality and drinking.
The data
Alcohol-related deaths are an important contributor to overall mortality in Finland. For instance, Mäkelä [18] reports that alcohol-related deaths accounted for 6% of all deaths in Finland over the period 1987–1995. Our aggregate data on the number of alcohol-related deaths per 100,000 inhabitants originates from Statistics Finland; reporting errors and misclassifications of causes of death should therefore be minimal. The data set spans the period 1975–2001 and is comprehensive, covering all persons in all regions of the country. The major advantage of the data is that they are reliable because they derive from the death certificates given by physicians based on the classification of causes of death adopted by the World Health Organization. Alcohol-related mortality is defined as deaths from alcohol-related diseases and alcohol poisoning. Using the ICD10 (1998) classification by the World Health Organization, this refers to the following classes: F10 (mental and behavioral disorders due to use of alcohol), G312 (degeneration of nervous system due to alcohol), G4051 (special epileptic syndromes related to alcohol), G621 (alcoholic polyneuropathy), G721 (alcoholic myopathy), I426 (alcoholic cardiomyopathy), K292 (alcoholic gastritis), K70 (alcoholic liver disease), K860 (alcohol-induced chronic pancreatitis), O354 (maternal care for (suspected) damage to fetus from alcohol), P043 (maternal care for (suspected) damage to fetus from alcohol), X45 (accidental poisoning by and exposure to alcohol). A disadvantage of these data is that they include information solely on mortality, but on individuals’ health behavior. In addition, the data are not rich in terms of covariates.
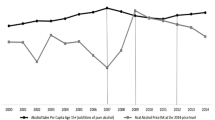
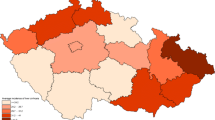
There are wide disparities in alcohol-related mortality across the Finnish regions (Fig. 1), as described by Mäkelä et al. [19] for the period 1991–1996. Permanent regional differences must be considered in estimating models on the effect of macroeconomic conditions on alcohol-related mortality. Figure 2 illustrates the overall relationship between the employment rate and alcohol-related mortality during 1975–2001 in Finland. Both series are detrended. Interestingly, this figure reveals that alcohol-related mortality seemed to decline during the great depression of the early 1990s. Mäkelä [18] has documented a similar pattern in alcohol-related mortality using data from 1987–1995.

Average alcohol-related mortality 1975–2001 per region (deaths per 100,000 inhabitants)

Employment rate and alcohol-related mortality in Finland 1975–2001. Note: Both series are detrended and normalized to having an average of 0 and a standard deviation of 1
The microlevel data on drinking originates from surveys conducted at the National Public Health Institute. The surveys on health behavior started in 1978. They have been repeated annually using samples of 5,000 randomly selected 15- to 64-year-old, permanently resident citizens. The sample frame excludes noncitizens, about 4% of the population. The survey is carried out as a postal questionnaire. On average 73% of those targeted responded. The major advantage of the data is that they include information on individuals’ health behavior, including consumption of alcohol. Hence the data set contains detailed questions on drinking since 1982. In addition, the questions have remained the same over the period. Socioeconomic background variables are recorded such as age, education, and marital status which the literature show to be important for drinking. We include these variables as covariates in the models, but it is important to keep in mind that this paper focuses on the effect of macroeconomic conditions on drinking. The most important drawback is that the data are self-reported, which means that they can contain reporting errors. In addition, binge drinking is not captured. It is typical that alcohol use is seriously underestimated in self-reported data sources. However, as Ruhm and Black [25] argue, this biases the estimates only if the underreporting varies systematically with the macroeconomic conditions.
To examine the effect of macroeconomic conditions we link these data sets using information on individuals’ places of residence to data from regional national accounts produced by Statistics Finland. Individuals’ places of residence are aggregated to 20 provinces that correspond to the so-called NUTS3 regions stipulated by the European Union. Recently constructed regional national accounts by Statistics Finland are available from 1975. This means that we are in a good position to investigate the relationship between alcohol-related mortality, drinking, and macroeconomic conditions because the time span of the data includes a number of business cycle fluctuations.
Macroeconomic conditions are measured by the regional employment rate in some models and by the change in regional real GDP in some. The unemployment rate has been favored as a measure of economic conditions in most of the previous literature. Unfortunately, the regional unemployment rates are not available for the entire period of investigation in our case. More importantly, some authors, including Clark and Summers [4], have argued that the employment rate is a better measure of labor market conditions for groups that frequently enter and exit the labor market. Entries and exits to the labor market do not change the size of the population, but they do change the size of the labor force. This means that the employment rate is more a stable measure than the unemployment rate. The latter point is particularly relevant in the Finnish case, because Ilmakunnas and Maliranta [9] have reported that the turnover of jobs and workers was intensive during the turbulent 1990s, which cover part of our observation period.
Empirical strategy
Econometrically we estimate models of the following type for the microdata on drinking: Y ijt =α j +βX ijt +E jt +λ t +ε ijt , where Y is the outcome (measures of alcohol drinking) for individual i living in region j in year t. X is a vector of individual characteristics (such as age and education), E measures economic conditions (the employment rate or the growth rate of regional real GDP), ε is an error term, and α and λ represent unobserved determinants of life-style behaviors associated with the region and survey year. It is important to include the fixed effects (FE) for regions because there are large, permanent differences in alcohol-related mortality and drinking across the Finnish regions. Some of these differences may arise, for instance, from the varying strictness of prevailing religious attitudes and other preferences towards alcohol drinking. In this FE set-up the effects of macroeconomic conditions on alcohol-related mortality and drinking are identified by intraregion variations, relative to the corresponding changes in other regions. We take into account the fact that observations are clustered by regions in the calculation of standard errors of estimates. Moulton [16] has stressed that otherwise standard errors are seriously biased downwards in a data set that combines aggregate variables such regional unemployment on microunits because there is a correlation of error terms within regions.
The recent research on the effects of macroeconomic conditions on health has used the FE set-up outlined above (e.g., [20, 21, 22, 23]). The most important motivation for the use of the FE set-up is that it allows us to exploit within-region changes in macroeconomic conditions that automatically control for time-invariant factors that may be spuriously correlated with economic conditions across regions. This spurious correlation has been a serious problem in the earlier studies in this strand of the literature. Therefore through the use of FE models we are able to obtain more precise and unbiased estimates for the effects of macroeconomic conditions.
For aggregate data on alcohol-related mortality we estimate FE models that are otherwise similar to those estimated for drinking to explain (the log of) alcohol-related mortality, but naturally we are unable to include individual-level covariates. Controls for the gender structure of the regions are included in these models, instead. It is important to take into account the gender structure of the regions because Mäkelä [18] documents (for the period 1987–1995) that alcohol-related deaths account in Finland for around 11% of all deaths for men, but for only 2% of all deaths for women.
Results
Alcohol-related mortality exhibits a countercyclical pattern. The results reported in Tables 1 and 2 reveal that an improvement in regional macroeconomic conditions measured by the employment rate produces a decrease in alcohol-related mortality, other things being equal. The regional GDP growth rate and alcohol-related mortality are not related. The magnitude of the estimated effect of the employment rate on alcohol-related mortality is quite substantial because, according to the magnitude of the coefficients reported in Table 2, a one percentage point increase in the employment rate leads to around a 2–5% decline in alcohol-related mortality. Interestingly, the great depression of the early 1990s is a clear exception to this general pattern (Table 1, row 3). During this period alcohol-related mortality declined, as there was an unprecedented meltdown in macroeconomic activity in Finland. This result is in line with Figure 2, which illustrated the aggregate evolution of alcohol-related mortality during the past few decades. It is important to note that our estimation results for the period 1975–2001 are not entirely driven by the great depression of the early 1990s because the results for the period 1975–1987 (Table 1, column 2) do not indicate that alcohol-related mortality declines during economic downturns.
The evidence from the microdata on drinking shows that there is no overall connection between macroeconomic conditions and the probability of being a drinker in the data after controlling for the respondent’s gender, age, education, and marital status (Table 3). The unreported control variables show that men, older persons, those with low education, and singles drink more. The only statistically significant results emerge for alcohol consumption. An expansion in regional GDP produces a substantial increase in alcohol consumption. Hence drinking is definitely procyclical in Finland. Based on the results reported in Table 3 (row 5 and 7) a one percentage point increase in the growth rate of regional GDP rate leads to an approx. 0.3–0.4% increase in alcohol consumption. This effect is most likely driven by the income effect because alcohol is a normal good. (Unfortunately, our data contain no information on the income level of individuals. Ruhm and Black [25] provide evidence that a part of the decrease in drinking in bad times results from declining incomes. Mangeloja and Pehkonen [12] report that the income elasticity for total alcohol consumption varies between 0.7–1.1 in Finland.) The results are stronger for regional GDP growth, but there is also some evidence that an increase in the employment rate produces an increase in the consumption of alcoholic items. In particular, the results in Table 3 (row 8) reveal that each one percentage point increase in the employment rate leads to an approx. 1.2% increase in the consumption of alcohol over the period 1990–1996. Overall the findings that derive from microlevel data on drinking suggest that slumps entail healthier times.
Discussion
This paper explored the relationship between alcohol-related mortality, drinking behavior, and macroeconomic conditions in Finland using both aggregate and microlevel data. The results from the aggregate data based on register-based information on mortality reveal that an improvement in regional macroeconomic conditions measured by the employment rate produced a decrease in alcohol-related mortality over the period of 1975–2001, other things being equal. This particular pattern is inconsistent with the recent evidence from the United States (e.g., Ruhm [21, 22]) according to which mortality declines during slumps. However, during the great depression of the early 1990s, alcohol-related mortality did decline in Finland, as there was an unprecedented collapse in macroeconomic activity. This is a rather remarkable finding as it is possible that it shows drinking of the kind that leads to death to be sensitive to changes in the income level even in a Nordic welfare state.
The results from the microdata that are based on a representative survey of the Finnish population over the period of 1982–2001 reveal that expansion in regional GDP and an increase in the employment rate produce an increase in alcohol consumption while having no effect on the probability of being a drinker. This piece of evidence confirms the fact that drinking is procyclical. Ruhm and Black [25] report similar results for the United States according to which the macroeconomic variation in drinking is dominated by changes at the intensive margin (how much existing drinkers consume) rather than at the extensive margin (whether they drink at all). An explanation for this pattern is that abstinence from alcohol consumption is most likely driven by individuals’ underlying preferences towards alcohol drinking that are immune to temporary macroeconomic conditions. In other words, the course of preferences takes more time than the duration of a typical business cycle. In contrast, the consumption of alcoholic items responds positively to the income level that increases during good economic times.
Our findings are most directly comparable to research that analyzes the effect of macroeconomic conditions on health behavior based on FE models that exploit regional variation (e.g., [20, 21, 22, 23, 25]). The Finnish evidence presented does not overwhelmingly support the conclusions reported for the United States according to which temporary economic downturns are good for health. In contrast, at least alcohol-related mortality seems to increase in those bad times that are not exceptional economic crises such as that experienced in Finland in the early 1990s, but there is still evidence that alcohol drinking is procyclical. This suggests that alcohol-related mortality and self-reported alcohol consumption may be delinked in the short-run business cycle context. One possible explanation for this paradox is that binge drinking, which is most closely associated with alcohol-related mortality, is not captured in a survey-based data that we use when studying the effect of macroeconomic conditions on alcohol consumption through the use of microlevel data. In addition to binge drinking, it is possible that drinking strong alcohol is countercyclical because strong alcohol can be used as a form of self-medication during economic distress. This calls for more detailed empirical studies on the prevalence of these most harmful forms of alcohol drinking during economic downturns and induces challenges for the design of surveys.
References
Brenner H (1973) Mental illness and the economy. Cambridge: Harvard University Press
Brenner H (1975) Trends in alcohol consumption and associated illnesses: some effects of economic changes. Am J Public Health 65: 1279–1292
Brenner H (1979) Mortality and the national economy. Lancet 26: 568–573
Clark K, Summers L (1982) The dynamics of youth unemployment. The youth labor market: its nature, causes, and consequences. Chicago: University of Chicago Press
Cook P, Moore M (1987) Alcohol. Handbook of health economics, vol 1. Amsterdam: Elsevier
Dee T (2001) Alcohol abuse and economic conditions: evidence from repeated cross-sections of individual-level data. J Health Econ 10: 257–270
Forbes J, McGregor A (1984) Unemployment and mortality in post-war Scotland. J Health Econ 3: 219–257
Gravelle H, Hutchinson G, Stern J (1981) Mortality and unemployment: a critique of Brenner’s time series analysis. Lancet II: 675–679
Ilmakunnas P, Maliranta M (2003) The turnover of jobs and workers in a deep recession: evidence from the Finnish business sector. Int J Manpower 24: 216–246
Joyce T, Mocan N (1993) Unemployment and infant health: time-series evidence from the state of Tennessee. J Hum Resour 28: 185–203
Jäntti M, Martikainen P, Valkonen T (2000) When the welfare state works: unemployment and mortality in Finland. The mortality crisis in transitional economies. UNU/Wider studies in development economics. Oxford: Oxford University Press
Mangeloja E, Pehkonen J (2006) Prices, income and availability: consumption of spirits, wine and beer in Finland, 1960–2004. Working paper no 309. Jyväskylä: University of Jyväskylä
Martikainen P, Valkonen T (1996) Excess mortality of unemployed men and women during a period of rapidly increasing unemployment. Lancet 348: 909–912
Martikainen P, Valkonen T, Martelin T (2001) Change in male and female life expectancy by social class: decomposition by age and cause of death in Finland 1971–95. J Epidemiol Community Health 55: 494–499
McAvinchey IA (1994) Comparison of unemployment, income, and mortality interaction for five European countries. Appl Econ 20: 453–471
Moulton BR (1990) An illustration of a pitfall in estimating the effects of aggregate variables on micro units. Rev Econ Stat 72: 334–338
Mäkelä P (1998) Alcohol-related mortality by age and sex and its impact on life expectancy. Eur J Public Health 8: 43–51
Mäkelä P (1999) Alcohol-related mortality during an economic boom and recession. Contemp Drug Problems 26: 369–390
Mäkelä P, Ripatti S, Valkonen T (2001) Alue-erot miesten alkoholikuolleisuudessa. Suomen Lääkärilehti 56: 2513–2519
Neumayer E (2004) Recessions lower (some) mortality rates: evidence from Germany. Soc Sci Med 58: 1037–1047
Ruhm C (2000) Are recessions good for your health? Q J Econ 115: 617–650
Ruhm C (2003) Good times make you sick. J Health Econ 22: 637–658
Ruhm C (2005a) Healthy living in hard times. J Health Econ 24: 341–363
Ruhm C (2005b) Macroeconomic conditions, health and mortality. Elgar companion to health economics. Cheltenham: Edward Elgar
Ruhm C, Black W (2002) Does drinking really decrease in bad times? J Health Econ 21: 659–678
Stern J (1983) The relationship between unemployment, morbidity, and mortality in Britain. Popul Stud 37: 61–74
Vartiainen E, Puska P, Jousilahti P et al. (1995) Twenty year trends in coronary risk factors in North Karelia and other areas of Finland. The North Karelia project. 20 year results and experiences. Helsinki: National Public Health Institute
Wagstaff A (1985) Time series analysis of the relationship between unemployment and mortality: a survey of econometric critiques and replications of Brenner’s studies. Soc Sci Med 21: 985–996
Conflict of interest
The corresponding author affirms that no connection exists between the author(s) and (a) the supplier of any product mentioned in this article or (b) any supplier of a competing product.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Johansson, E., Böckerman, P., Prättälä, R. et al. Alcohol-related mortality, drinking behavior, and business cycles. Eur J Health Econ 7, 212–217 (2006). https://doi.org/10.1007/s10198-006-0358-x
Issue Date:
DOI: https://doi.org/10.1007/s10198-006-0358-x