
Abstract
Background
The BioJet system allows the fusion of magnetic resonance imaging (MRI) images with real-time transrectal ultrasonography to accurately direct biopsy needles to the target lesions. To date, the superiority of targeted biopsy using the BioJet system over cognitive registration remains unknown.
Methods
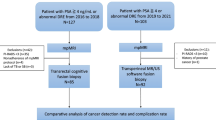
This retrospective study included 171 biopsy-naïve men with elevated prostate-specific antigen (2.5–20 ng/mL) and MRI-positive lesions; 74 and 97 men underwent a four-core targeted biopsy per MRI-positive target lesion and a 14-core systematic biopsy transperineally using the BioJet system and cognitive registration, respectively. Detection rates of significant cancer, defined as grade group ≥ 2 or maximum cancer length ≥ 5 mm, were compared between the BioJet system and cognitive registration using propensity score matching and a multivariate logistic regression model.
Results
After propensity score matching (67 men for each group), the detection rates of significant cancer were significantly higher in the BioJet group than in the cognitive group for both targeted (76% vs. 46%, P = 0.002) and systematic (70% vs. 46%, P = 0.018) biopsy. Multivariate analysis of the entire cohort also showed that the BioJet system was independently associated with significant cancer detection by targeted and systematic biopsy (P < 0.01), along with a higher prostate-specific antigen density and a higher prostate imaging reporting and data system score.
Conclusions
Transperineal prostate biopsy using the BioJet system is superior to cognitive registration in detecting significant cancer for targeted and systematic biopsies.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Previous studies, including a randomized control study, have revealed the efficacy of magnetic resonance imaging (MRI)-guided targeted biopsy (TgB) over systematic biopsy without MRI [1,2,3]. Recently, MRI-transrectal ultrasound (TRUS) fusion TgB has shown superiority over cognitive visual registration transrectal TgB [4, 5] whereas others have shown comparable outcomes in terms of significant cancer (SC) detection [6, 7].
A recent systematic review showed the superiority of the transperineal approach over the transrectal approach in terms of SC detection and infectious complications in fusion TgB [8]. We performed MRI-guided cognitive TgB via a transperineal approach and reported its efficacy in detecting SC [9]. To the best of our knowledge, no study has compared the diagnostic performance of transperineal MRI-guided TgB with fusion and cognitive registration. Furthermore, few studies have compared the diagnostic performance of systematic biopsy (SyB) between these two methods. Visualization of MRI-positive target lesions in fusion image-guided biopsy may potentially improve SC detection by SyB.
Since the start of the fiscal year 2022, the Japanese universal health insurance system has covered MRI-TRUS image-guided fusion biopsy. The BioJet system (D&K Technologies, Germany) is an equipment that allows the fusion of MRI images with real-time TRUS by using a position-encoded stepper to accurately direct biopsy needles. More accurate targeting can be expected using the BioJet system compared to cognitive registration. The superiority of the BioJet system was reported for SC detection in the transitional zone (TZ) in a per-core-based analysis compared to TgB using real-time virtual sonography [10], which reportedly yields superior cancer detection over cognitive registration [11]. Although a pilot study demonstrated superior SC detection by the BioJet TgB compared with SyB in 250 cases [12], another pilot study directly comparing BioJet TgB with cognitive TgB in 50 men did not show the superiority of BioJet TgB in terms of SC detection [13].
In this single-institutional retrospective study, we compared the diagnostic performance of TgB and SyB using the BioJet system with that of transperineal cognitive TgB and SyB. Propensity score matching (PSM) for potential confounders was used to reduce their influence on the associations between biopsy methods and SC detection.
Patients and methods
The Institutional Review Board approved the study protocol (#2464). This retrospective study included 171 biopsy-naïve men with positive MRI findings and elevated prostate-specific antigen levels (PSA, 2.5–20 ng/mL). Between October 2020 and August 2022, 74 men underwent TgB and 14-core SyB using the BioJet system. Between April 2019 and October 2020, 97 men underwent transperineal cognitive TgB and 14-core SyB procedures. The biopsy using the BioJet system was performed as an advanced medical technology approved by the Japanese Ministry of Health, Labor, and Welfare before April 2022. All biopsy procedures were performed transperineally.
The pre-biopsy MRI findings were prospectively evaluated using the Prostate Imaging-Reporting and Data System (PI-RADS, version 2) at a radiology-urology conference attended by a uroradiologist (S.I.) and three urologists (F.K., M.I., and S.K.) with ≥ 10 years of experience. PI-RADS scores ≥ 3 were defined as positive. Sagittal location of target lesions was assigned to apex or base according to their location relative to the prostate sagittal middle line.
Biopsy using the BioJet system is typically performed under saddle block anesthesia by injecting 1 mL of high specific gravity marcaine through the L3/4 or L4/5 intervertebral foramen. Three-dimensional images of the prostate and MRI-positive target lesions were generated from MRI images using the BioJet system and fused with the real-time image of TRUS (Fig. 1a, b). For TgB, four cores per target lesion were biopsied under the guidance of real-time fusion images using a guide-grid template. Similarly, for SyB, 14 cores were biopsied from predefined sites, as previously described (Fig. 1c) [14] using fusion images. SyB using the BioJet system was performed under the guidance of fusion images. When the target lesion overlapped a predefined SyB site, a SyB core was taken without avoiding the target lesion. An experienced urologist (M.I.) conducted the biopsy using the BioJet system.

Magnetic resonance imaging (MRI)-transrectal ultrasound fusion images used during the BioJet biopsy. a A Prostate Imaging-Reporting and Data System score 4 lesion found on pre-biopsy MRI. Arrowheads indicate a target lesion on T2-weighted imaging, diffusion-weighted imaging, apparent diffusion coefficient map, and dynamic contrast enhancement imaging. b Three-dimensional images of the prostate (green color) and a target lesion (red color) generated in the BioJet system. Under the guidance of these images, a biopsy needle was inserted through an appropriate grid. c Schema of 14-core systematic biopsy sites. A, anterior; P, posterior; AL, anterolateral; PL, posterolateral, TZ, transitional zone
Cognitive biopsy was performed freehand, typically under local anesthesia by experienced urologists (M.I., S.K., and M.T.) or trainees under the supervision of an expert, as previously described [14]. The sites and number of SyB and TgB core samples per target lesion were identical to those of the BioJet biopsy.
SC was defined as grade group (GG) ≥ 2 or maximum cancer length (MCL) ≥ 5 mm [9]. We compared biopsy outcomes between BioJet and cognitive registration for both TgB and SyB, including SC detection, number of SC cores, and MCL. In addition, outcomes of SyB were compared in lobes ipsilateral to and contralateral to the target lesions, and MRI-negative regions between BioJet and cognitive registration. MRI-negative regions were defined as predefined SyB sites where the target lesions did not overlap axially. PSM at a 1:1 ratio was carried out with a caliper of 0.25 to adjust for possible baseline confounders, including age, PSA density, family history of prostate cancer, findings of the digital rectal examination, PI-RADS score according to zonal location, diameter of MRI-positive target lesions, and zonal and sagittal location of target lesions. PI-RADS score was distinguished by peripheral zone (PZ) and transitional zone (TZ) in PSM considering the possible difference of SC detection rate by the zonal location [10, 15].
Diagnostic performance in terms of SC detection was compared between BioJet and cognitive biopsy in subgroups stratified by PSA level (< 10 ng/mL and ≥ 10 ng/mL), prostate volume (PV) (< 30 mL and ≥ 30 mL), PI-RADS scores, PSA density (< 0.2 ng/mL2 and ≥ 0.2 ng/mL2), zonal (PZ and TZ), and sagittal location (apex and base) of target lesions.
Statistical analyses were performed with EZR software (version 1.54) [16] and R (version 4.2.1). Differences in continuous variables were evaluated using the Wilcoxon rank-sum test. Differences in categorical variables were evaluated using Fisher’s exact test in the entire cohort and the Mantel–Haenszel test in the PSM cohort. Logistic regression analysis was used to evaluate variables associated with SC detection. A reduced multivariate model was developed using the stepwise backward method. A two-tailed P value < 0.05 was considered statistically significant.
Results
Table 1 lists the demographics of 171 men who underwent BioJet (n = 74) or cognitive biopsy (n = 97) before and after PSM. After PSM, both groups consisted of 67 men. There were no significant between-group differences in clinical variables other than anesthesia methods before and after PSM.
Table 2 shows biopsy outcomes in the BioJet and cognitive groups before and after PSM. After PSM, the SC detection rate by TgB was significantly higher in the BioJet group than in the cognitive group (76% vs. 46%, P = 0.002). No significant differences were observed in the number of SC cores or MCL between BioJet and cognitive TgB. BioJet SyB also showed a significantly higher SC detection rate than cognitive SyB (70% vs. 46%, P = 0.018), along with a significantly greater number of SC cores (median 1 vs. 0, P = 0.045) and longer maximum cancer length (median 6 vs. 2, P = 0.041) in the whole lobe after PSM. BioJet SyB showed a significantly higher SC detection rate than cognitive SyB in the lobes ipsilateral to the target lesions (61% vs. 40%, P = 0.021) but not in the contralateral lobes. To assess the background where BioJet SyB was superior to cognitive SyB in SC detection, we compared SyB outcomes between the two approaches within and outside TgB lesions (Supplementary Table 1). Despite a smaller number of SyB cores within TgB lesions (median: 1 for both groups, P = 0.022), BioJet SyB detected SC within TgB lesions more efficiently than cognitive SyB (42% vs. 22%, P = 0.021) after PSM. The SC detection rate of SyB in MRI-negative regions (i.e., outside TgB lesions) was not statistically different between the two groups in the whole lobe (58% vs. 42%, P = 0.082) and in lobes ipsilateral to (54% vs. 42%, P = 0.23) and contralateral to TgB lesions (21% vs. 28%, P = 0.42).
In the entire cohort, two men (1%) experienced acute urinary retention (one from each group), and none experienced infectious complications (Table 2).
Subgroup analyses in the PSM cohort showed that BioJet TgB was significantly superior to cognitive TgB in terms of SC detection irrespective of PV, PSA density, zonal and apical location of the target lesions, and in subgroups with a PI-RADS score of 4 and lower PSA level (Fig. 2a). BioJet SyB was also significantly superior to cognitive SyB in subgroups with a PI-RADS score of 4, higher PV, lower PSA level, higher PSA density, TZ and basal locations of the target lesions (Fig. 2b).

Forest plot of odds ratios and 95% confidence intervals of BioJet biopsy versus cognitive biopsy in detecting significant cancer in subgroups stratified by PSA level (< 10 ng/mL and ≥ 10 ng/mL), PV (< 30 mL and ≥ 30 mL), PI-RADS scores, and zonal and sagittal location of target lesions; a targeted biopsy, b systematic biopsy. PI-RADS, Prostate Imaging-Reporting and Data System; PV, Prostate volume; PSA, Prostate-specific antigen; PZ, Peripheral zone; TZ, Transitional zone
Multivariate analysis was conducted in the entire cohort for TgB and SyB to confirm the superiority of BioJet biopsy over cognitive registration in detecting SC. As shown in Table 3, BioJet biopsy was significantly and independently associated with SC detection by both TgB and SyB with respective odds ratios (OR) (95% confidence intervals [CI]) of 5.10 [2.21–11.8] (P < 0.001) and 3.20 [1.50– 6.85] (P = 0.003). Higher PSA density and higher PI-RADS scores were also significantly and independently associated with SC detection by both TgB and SyB, whereas the apical location of target lesions was similarly associated with SC detection by SyB (Table 3).
Discussion
In this study, we showed the superiority of MRI-TRUS fusion image-guided biopsy using the BioJet system over transperineal cognitive biopsy for SC detection by TgB and SyB. These findings were obtained from PSM analysis to minimize the influence of potential confounders. Furthermore, our findings were confirmed by performing a multivariate analysis of the entire study cohort. To the best of our knowledge, this is the first study to demonstrate the superiority of transperineal fusion biopsy using the BioJet system over transperineal cognitive biopsy to detect SC.
Regarding TgB, the superior detection of SC by BioJet biopsy over cognitive registration could be attributed to the accurate capture of target lesions under the guidance of MRI-TRUS fusion images. Notably, the superiority of BioJet biopsy was also observed for SyB. In our study, BioJet SyB performed better than cognitive SyB in the detection of SC in the whole lobe and lobes ipsilateral to target lesions but not in the contralateral lobes. In our BioJet SyB practice, a SyB core is taken without avoiding the target lesion when it overlapped a predefined SyB site. The guidance of fusion images is likely to confer efficient SC detection in SyB sites overlapping TgB lesions.
Although a recent randomized study showed the superiority of MRI-guided fusion TgB over cognitive TgB via the transrectal approach [5], the superiority of fusion image guidance over cognitive registration remains controversial, particularly when TgB is performed via the transperineal approach. Two comparative studies using the transperineal approach for TgB using the BioJet system have been published. One study comparing BioJet and cognitive TgB showed comparable SC detection rates (68% and 64%, respectively) [13]. In another study, although BioJet TgB showed superior SC detection for target lesions in the TZ on a per-core basis, SC detection rates were comparable between BioJet TgB and TgB using real-time virtual sonography on a per-patient basis (62% vs. 59%, respectively) [10]. Our study, yielding respective SC detection rates of 76% vs. 51%, is the first to demonstrate the superiority of BioJet TgB over cognitive TgB in detecting SC.
In our study, a single experienced urologist (M.I.) performed biopsies using the BioJet system, whereas cognitive biopsies were performed by various urologists, including trainees under the supervision of experienced urologists, which could have biased biopsy outcomes in favor of the BioJet group. A previous study on BioJet biopsy showed comparable outcomes between experts and residents unless the target lesions were < 8 mm [17]. Our BioJet cohort included only seven men (9%) with index lesions of < 8 mm. We also reported comparable biopsy outcomes between senior urologists and trainees in transperineal cognitive Tg [18]. Therefore, we considered the influence of interoperator variability to be limited in our study.
The present study has some limitations. First, there was a possible bias associated with a retrospective study using a small single-institutional cohort, although the PI-RADS scores were prospectively evaluated and PSM was used to minimize between-group differences in the participants’ backgrounds. External validation with a large multicenter cohort is necessary to confirm our findings. Second, saddle block anesthesia was utilized for BioJet biopsies in most cases while local anesthesia was for cognitive biopsies. We cannot deny the possibility that operators have tried to shorten procedure time to reduce pain when performing cognitive biopsies under local anesthesia. However, the local anesthesia method we utilize can also control pain during biopsy as reported previously [19]. Third, we did not compare biopsy outcomes between the prostatectomy specimens. More studies are warranted to validate biopsy outcomes by referring to the pathology of the prostatectomy specimens.
Conclusion
MRI-TRUS fusion image-guided transperineal biopsy using the BioJet system is superior to transperineal MRI-targeted cognitive biopsy in detecting SC using TgB and SyB.
References
Drost FH, Osses DF, Nieboer D et al (2019) Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst Rev 4:CD012663. https://doi.org/10.1002/14651858.CD012663.pub2
Kasivisvanathan V, Rannikko AS, Borghi M et al (2018) MRI-targeted or standard biopsy for prostate-cancer diagnosis. N Engl J Med 378(19):1767–1777. https://doi.org/10.1056/NEJMoa1801993
Siddiqui MM, Rais-Bahrami S, Turkbey B et al (2015) Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA 313(4):390–397. https://doi.org/10.1001/jama.2014.17942
Wysock JS, Rosenkrantz AB, Huang WC et al (2014) A prospective, blinded comparison of magnetic resonance (MR) imaging-ultrasound fusion and visual estimation in the performance of MR-targeted prostate biopsy: the PROFUS trial. Eur Urol 66(2):343–351. https://doi.org/10.1016/j.eururo.2013.10.048
Izadpanahi MH, Elahian A, Gholipour F et al (2021) Diagnostic yield of fusion magnetic resonance-guided prostate biopsy versus cognitive-guided biopsy in biopsy-naive patients: a head-to-head randomized controlled trial. Prostate Cancer Prostatic Dis 24(4):1103–1109. https://doi.org/10.1038/s41391-021-00366-9
Wegelin O, van Melick HHE, Hooft L et al (2017) Comparing three different techniques for magnetic resonance imaging-targeted prostate biopsies: a systematic review of in-bore versus magnetic resonance imaging-transrectal ultrasound fusion versus cognitive registration. Is there a preferred technique? Eur Urol 71(4):517–531. https://doi.org/10.1016/j.eururo.2016.07.041
Wegelin O, Exterkate L, van der Leest M et al (2019) The FUTURE trial: a multicenter randomised controlled trial on target biopsy techniques based on magnetic resonance imaging in the diagnosis of prostate cancer in patients with prior negative biopsies. Eur Urol 75(4):582–590. https://doi.org/10.1016/j.eururo.2018.11.040
Rai BP, Mayerhofer C, Somani BK et al (2021) Magnetic resonance imaging/ultrasound fusion-guided transperineal versus magnetic resonance imaging/ultrasound fusion-guided transrectal prostate biopsy-a systematic review. Eur Urol Oncol 4(6):904–913. https://doi.org/10.1016/j.euo.2020.12.012
Nakanishi Y, Ito M, Fukushima H et al (2019) Who can avoid systematic biopsy without missing clinically significant prostate cancer in men who undergo magnetic resonance imaging-targeted biopsy? Clin Genitourin Cancer 17(3):e664–e671. https://doi.org/10.1016/j.clgc.2019.03.011
Nagai T, Naiki T, Hamamoto S et al (2020) Comparison of real-time virtual sonography navigation versus BioJet navigation on magnetic resonance imaging-guided prostate needle biopsy: a single institutional analysis. J Endourol 34(7):739–745. https://doi.org/10.1089/end.2020.0042
Miyagawa T, Ishikawa S, Kimura T et al (2010) Real-time virtual sonography for navigation during targeted prostate biopsy using magnetic resonance imaging data. Int J Urol 17(10):855–860. https://doi.org/10.1111/j.1442-2042.2010.02612.x
Shoji S, Hiraiwa S, Ogawa T et al (2017) Accuracy of real-time magnetic resonance imaging-transrectal ultrasound fusion image-guided transperineal target biopsy with needle tracking with a mechanical position-encoded stepper in detecting significant prostate cancer in biopsy-naive men. Int J Urol 24(4):288–294. https://doi.org/10.1111/iju.13306
Valerio M, McCartan N, Freeman A et al (2015) Visually directed vs. software-based targeted biopsy compared to transperineal template mapping biopsy in the detection of clinically significant prostate cancer. Urol Oncol Semin Orig Investig. https://doi.org/10.1016/j.urolonc.2015.06.012
Takeshita H, Numao N, Kijima T et al (2013) Diagnostic performance of initial transperineal 14-core prostate biopsy to detect significant cancer. Int Urol Nephrol 45(3):645–652. https://doi.org/10.1007/s11255-013-0416-0
Shoji S, Hiraiwa S, Endo J et al (2015) Manually controlled targeted prostate biopsy with real-time fusion imaging of multiparametric magnetic resonance imaging and transrectal ultrasound: an early experience. Int J Urol 22(2):173–178. https://doi.org/10.1111/iju.12643
Kanda Y (2013) Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant 48(3):452–458. https://doi.org/10.1038/bmt.2012.244
Checcucci E, Piramide F, Amparore D et al (2021) Beyond the learning curve of prostate MRI/TRUS target fusion biopsy after more than 1000 procedures. Urology 155:39–45. https://doi.org/10.1016/j.urology.2021.06.021
Ito M, Kataoka M, Takemura K et al (2019) Learning curves, cancer detection rates, and complications of transperineal prostate biopsy under local anesthesia by trainee urologists. J Urol 201(4):E181–E181
Kubo Y, Kawakami S, Numao N et al (2009) Simple and effective local anesthesia for transperineal extended prostate biopsy: application to three-dimensional 26-core biopsy. Int J Urol 16(4):420–423. https://doi.org/10.1111/j.1442-2042.2009.02269.x
Acknowledgements
Figure 1c was cited with permission from the publisher of reference 14 (License number 5551200917702).
Author information
Authors and Affiliations
Contributions
Masaya Ito: Conceptualization, data curation, formal analysis, investigation, supervision, and writing–original draft preparation; Ichiro Yonese: Data curation, formal analysis, investigation, visualization, and writing–review & editing; Masahiro Toide: Investigation, writing–review & editing; Shuozo Ikuta: Investigation, writing–review & editing; Shuichiro Kobayashi: Investigation, writing–review & editing; Fumitaka Koga: Conceptualization, investigation, supervision, and writing–review & editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest. The study protocol was approved by the Institutional Review Board (approval #2464).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
About this article

Cite this article
Ito, M., Yonese, I., Toide, M. et al. Superior detection of significant prostate cancer by transperineal prostate biopsy using MRI-transrectal ultrasound fusion image guidance over cognitive registration. Int J Clin Oncol 28, 1545–1553 (2023). https://doi.org/10.1007/s10147-023-02404-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-023-02404-z