
Abstract
Background
To assess the clinical variables that effect progression in patients with viable tumor after post-chemotherapy lymph node dissection due to disseminated non-seminomatous germ-cell tumors.
Methods
We performed a retrospective analysis of 32 patients with viable tumor after PC-RPLND, operated between 1990 and 2016. Patients were categorized into 2 groups as favorable and non-favorable (intermedia and poor) according to International Germ Cell Consensus Classification (IGCCC). Tumor size was determined as the largest dimension of retroperitoneal mass. Clinical factors and adjuvant chemotherapy were evaluated to impact on recurrence free survival (RFS) and overall survival (OS).
Results
The median age of the patients and follow-up duration were 28.5 (17–51) years and 51.5 (4–253) months, respectively. 5-year RFS and OS were 57.8–66.8%, respectively. On univariate analysis, percentage of viable tumor, IGCCC risk group, primary site, second-line chemotherapy and surgical margin status were significant for RFS (p = 0.034, p = 0.002, p < 0.001, p = 0.011 and p < 0.001, respectively), while IGCCC risk group, second-line chemotherapy and surgical margin status were significant for OS (p = 0.004, p = 0.010 and p < 0.001, respectively). On multivariate analysis, second-line chemotherapy and surgical margin were independent risk factors for RFS (p = 0.016, HR 4.927 95% CI 1.34–18.02 and p < 0.001, OR 9.147 95% CI 2.61–31.98, respectively) and surgical margin status was the only predictor of OS (p = 0.038, HR 3.874 95% CI 1.07–13.69).
Conclusion
Retroperitoneal lymph node dissection with negative surgical margin is essential for patients with viable residual tumor after chemotherapy. Need for second-line chemotherapy shows risk of progression.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Post-chemotherapy retroperitoneal lymph node dissection (PC-RPLND) is considered an important therapeutic and staging modality in advanced germ-cell tumors (GCTs). One of the corner-stones in treatment of advanced testicular cancer was the discovery of cisplatin-based chemotherapy; survival rates have reached 70% even for poor prognostic patients [1, 2]. Disease progression after PC-RPLND is a major problem both for patients and clinicians. Live tumor in residual mass is an independent poor prognostic factor for recurrence [3]. The current literature reveals a rate of viable malignancy (± teratoma) in 9–31% of PC-RPLND pathology [4,5,6,7,8]. On the other hand, management of patients with viable tumor is ill-defined in the literature due to a lack of well-designed studies and a slim patient population.
Defining clinical features that predict progression allows clinicians to select appropriate management, such as adjuvant chemotherapy regimens or surveillance. The aim of this study was to present our patients’ outcomes with residual viable tumor after PC-RPLND and determine the risk factors for progression in this population.
Patients and methods
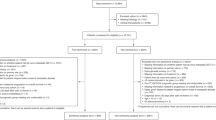
Our Institutional Review Board approved this study with number GO19/675. We identified 237 patients who underwent PC-RPLND between January 1990 and January 2017. Patients with fibrosis or teratoma in the PC-RPLND specimen, seminoma in the orchiectomy specimen, patients with high tumor markers after chemotherapy and those with missing data were excluded. In sum, 32 patients with viable tumor in the PC-RPLND specimen were analyzed.
All patients were evaluated with thoracoabdominal computed tomography and tumor markers after orchiectomy. After all patients received first-line platinum-based chemotherapy, these tools were repeated. Patients with elevated tumor markers received second-line chemotherapy and PC-RPLND (open transabdominal approach) was performed after normalization of tumor markers. Full bilateral template or modified template RPLND was performed at the discretion of the attending surgeon [9].
Patients were categorized into 2 groups as favorable and non-favorable (intermediate and poor) according to International Germ Cell Consensus Classification (IGCCC) [10]. Tumor size was determined as the largest dimension of retroperitoneal mass. Patients with non-GCT tumors, such as sarcoma, in the PC-RPLND specimen, designated as teratoma with malignant transformation, were included in the study [11, 12].
The effect of clinical factors on recurrence free survival and overall survival was evaluated. These factors included age, IGCCC risk group, primary tumor site, tumor size, time interval, second-line chemotherapy, percentage of viable tumor in residual masses, surgical margin status and adjuvant chemotherapy.
SPSS (23.0 Chicago, IL) program was used for statistical analysis. The Kaplan–Meier method was used for estimating PFS and OS. The log-rank test and the Cox proportional hazard regression mode were used for univariate and multivariate analyses, respectively.
Results
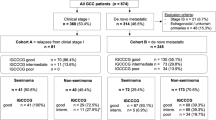
The median age of patients and follow-up duration were 28.5 (17–51) years and 51.5 (4–253) months, respectively. Six (18.8%) patients had a primary retroperitoneal tumor. There were 17 (53%) patients in favorable group, 8 (25%) patients in intermediate group and 7 (22%) patients in poor-risk group according to IGCCC. Among all of them, 3 patients received POMP-ACE (Cisplatin, Vincristine, Methotrexate, Bleomycin, Actinomycin D, Cyclophosphamide, Etoposide) regimen and the others received BEP (Bleomycin, Etoposide, Cisplatin) regimen as first-line chemotherapy. Eleven patients received second-line chemotherapy. VIP (Etoposide, Ifosfamide, Cisplatin), TIP (Paclitaxel, Ifosfamide, Cisplatin), BEP and EP (Etoposide, Cisplatin) were given to 6, 3, 1 and 1 patients, respectively. One patient had teratoma and rhabdomyosarcoma, one patient teratoma and adenocarcinoma (teratoma with malignant transformation) and the others had at least one GCT with or without teratoma. Positive surgical margin rate was 28% (9 patients) and 7 (77.8%) of them were given adjuvant chemotherapy. Totally 20 (62.5%) patients were administered adjuvant chemotherapy; TIP was given to 5 patients, EP 4 patients, BEP 3 patients, VIP 2 patients, paclitexal gemsitabin cisplatin regimen 2 patients and VAC (Vincristine, Actinomycin, Cyclophosphamide), AİVP (Ifosfamide, Etoposide, Adriamisin, G-CSF), VBM (Vinblastine, bleomycin, methotrexate) and Taxol were given to one patient each. Demographic and clinical characteristic of these patients can be found in Table 1.
Disease recurrence was seen in 14 (43.7%) patients and among them 11 (34.4%) died due to progression. The median time to recurrence and death were 9 (3–57) and 16 (6–103) months. Three patients, who showed progression and lived, had no evidence of disease at last follow-up. They underwent salvage RPLN, RPLN & hepatic resection and pulmonary resection after they receiving salvage chemotherapy. 5-year RFS and OS were 57.8% and 66.8%, respectively. On univariate analysis, percentage of viable tumor, IGCCC risk group, primary site, second-line chemotherapy and surgical margin status were significant for RFS (p = 0.034, p = 0.002, p < 0.001, p = 0.011 and p < 0.001, respectively). (Table 2) On multivariate analysis, second-line chemotherapy and surgical margin were independent risk factors for RFS (p = 0.016, HR 4.927 95% CI 1.34–18.02 and p < 0.001, OR 9.147 95% CI 2.61–31.98, respectively). (Table 3) For OS, IGCCC risk group, second-line chemotherapy and surgical margin status were significant on univariate analysis (p = 0.004, p = 0.010 and p < 0.001, respectively). (Table 2) Surgical margin status was the only predictor of OS on multivariate analysis (p = 0.038, HR 3.874 95% CI 1.07–13.69). (Table 3) When factors associated with positive surgical margins were investigated, those in IGCCC non-favorable group and primary extragonadal tumors were found to have higher positive surgical margin rates (p = 0.028 and p < 0.001). Age, lymph node size, tumor stage, time interval, second-line chemotherapy, percentage of viable tumor and adjuvant chemotherapy had no impact on positive surgical margins (p = 0.694, p = 0.365, p = 0.083, p = 0.612, p = 0.118, p = 0.185 and p = 0.264, respectively).
13 (41%) patients had a radical bilateral template RPLND, while 19 (59%) patients received a modified template RPLND. There were a total of 16 additional procedures in 12 (37.5%) patients; 3 (9.4%) being en-bloc nephrectomy, 3 (9.4%) ureteroureterostomy with stent placement, 2 (6.3%) renal vein repair, 3 (9.4%) vena cava repair, 2 (6.3%) thrombectomy with vena cava repair, 1 (3.1%) vena cava patch angioplasty, 1 (3.1%) aortic repair and 1 (3.1%) hepatic resection. Only one patient experienced total evisceration and underwent surgery. There was no mortality.
Discussion
Efficacy of chemotherapy is crucial for excellent outcomes in treatment of advanced GCTs. Furthermore, indications for PC-RPLND in NSGCTs are well defined and surgery has significant advantages. One of the most important arguments for PC-RPLND is the presence of about 50% viable tumor [13, 14]. There is no need for additional treatment in case of teratoma in PC-RPLND. Although growing teratoma syndrome is of concern for these cases, complete resection will yield low recurrence rates [15]. However, viable tumor is the main concern for clinicians and is related with poor prognosis. In addition to the low incidence of testis tumor, patients with viable tumor after PC-RPLN due to advanced disease make up a small proportion testis cancer case. Inevitably, management of this group and risk factors for progression are not clearly defined.
Spies et al. published outcomes of 41 patients with viable tumor in surgical specimen after PC-RPLN [16]. Their study included patients who received first-line and second-line chemotherapy and underwent desperation surgery. The 5-year RFS and 5-year disease-specific survival (DSS) were 71% and 50%, respectively. They found that an elevated AFP before PC-RPLND and presence of postoperative disease recurrence were predictors of DSS, while elevated AFP, advanced stage, an increase amount of preoperative chemotherapy (> 5 cycles) and postoperative complications were predictors of OS. Fizazi et al. studied prognostic factors in 238 viable tumor cases and showed that being in IGCCC intermediate or high-risk group, presence of > 10% viable tumor and incomplete resection were independent poor prognostic factors. 5-year progression-free survival (PFS) rates for patients with no risk factors, with 1 risk factor and with 2 or more risk factors were 100%, 83% and 51%, respectively [12]. These results were verified by a contemporary study published in 2008 with a median follow-up of 5.4 years [17]. Their studies included patients who only received first-line chemotherapy and had normal tumor markers. Our study included salvage second-line chemotherapy, and IGCCC risk group and percentage of viable tumor were found to be insignificant for survival. This may have been caused by the smaller number of patient group.
In our study, there was no desperation surgery and nearly one-third of patients received second-line chemotherapy. The 5-year RFS and OS were 57.8–66.8%, respectively. Second-line chemotherapy and surgical margin were independent risk factors for RFS and surgical margin status was the only predictor of OS. Complete resection was performed on all patients, but microscopic positive surgical margin was the most important parameter for recurrence and death. So, complete resection with negative surgical margin must be the primary goal of surgery. Another predictor of recurrence was second-line chemotherapy. Spies et al. emphasized on adequate systemic chemotherapy until the normalization of serum tumor markers [16]. On the other hand, second-line chemotherapy was predictor of recurrence in our study and > 5 cycles chemotherapy was significant for OS in theirs. Although the preoperative normalization of tumor markers has important prognostic significance [18, 19], need for second-line chemotherapy was found to predict recurrence. This might be associated with less chemo-sensitive tumors in patients who had need for second-line chemotherapy.
Adjuvant chemotherapy is the most important matter in patients with viable tumor. Because contribution of chemotherapy to survival of advanced GCTs was known very well, adjuvant chemotherapy was used routinely [20]. Fox et al. reported viable tumor was detected in 43 of 417 PC-RPLND cases [21]. Of 34 patients who had complete resection, 27 had adjuvant chemotherapy and 7 did not. Nineteen of 27 (70%) were continuously disease-free. All seven who received no postoperative chemotherapy have relapsed. Similarly, in a study that was published by Einhorn et al., postoperative chemotherapy recipients were long-term survivors [21]. However, Spies et al. did not indicate the impact of postoperative chemotherapy on survival in their study [16]. Neither was it emphasized in sCR1 (surgical complete response) study published by Fizazi et al. Although PFS was better in the group who received postoperative chemotherapy when compared to the patients who did not, there was no significant difference in 5-year OS rates [12]. In sCR2 study, there was no evidence of a survival benefit associated with postoperative chemotherapy [17]. They suggested that surveillance should be offered to patients with no risk factors (IGCCC favorable group, < 10% viable tumor and complete resection) and complete resection is more important than postoperative chemotherapy. In our study, adjuvant chemotherapy was not beneficial to RFS or OS. However, our study included a small number of patients and there were no indications for adjuvant chemotherapy. So, these results may not be sufficient for arguing the impact of adjuvant chemotherapy on survival.
The median tumor size (8 cm) was relatively high and ≥ II C clinical stage constituted about one-fourth. Half of all patients were in favorable risk group according to IGCCC and so, we defined IGCCC groups as favorable and non-favorable (intermediate and poor). IGCCC risk group, stage and percentage of viable tumor were not predictors of recurrence and survival. It may be explained with larger median tumor size, and a low number of patients.
Baniel et al. defined 144 complications established in 125 cases in their series of 603 PC-RPLND patients (20.7%). Of all, 93% had residual mass ≥ 5 cm and overall mortality rate was 0.8% [22]. Cary et al. reported 22.1% additional procedure and 3.7% complication rate [23]. Additional procedure rate was associated with mass size, high serum markers and RPLND pathology. For our study, there was no mortality and only one postoperative complication (Clavien grade III A). Sixteen additional procedures were performed in 12 (37.5%) patients. This high additional procedure rate might be associated with high median tumor size.
The main limitation of our study was its retrospective nature. This study included patients who were treated over the past 31 years. So, treatment modalities evolved during this period. Pathology results were reported by different genitourinary pathologists who might have had different interpretations. The effect of adjuvant chemotherapy in surgical margin positive patients could not be assessed due to the limited number of patients who did not receive adjuvant chemotherapy. Finally, there was a heterogenic patient population because our institution is a tertiary-referral hospital.
Post-chemotherapy lymph node dissection has an important contribution to survival of patients with viable tumor despite preoperative chemotherapy. Compete resection with negative surgical margin must be the primary goal of surgery for good survival and less recurrence. Patients who needed second-line chemotherapy have a higher risk of recurrence.
References
Einhorn LH (1990) Treatment of testicular cancer: a new and improved model. J Clin Oncol 8:1777–1781
van Dijk MR, Steyerberg EW, Habbema JD (2006) Survival of non-seminomatous germ cell cancer patients according to the IGCC classification: an update based on meta-analysis. Eur J Cancer 42:820–826
Spiess PE, Brown GA, Liu P et al (2006) Predictors of outcome in patients undergoing postchemotherapy retroperitoneal lymph node dissection for testicular cancer. Cancer 107:1483–1490
Hendry WF, Norman AR, Dearnaley DP et al (2002) Metastatic nonseminomatous germ cell tumors of the testis: results of elective and salvage surgery for patients with residual retroperitoneal masses. Cancer 94:1668–1676
de Wit R, Stoter G, Kaye SB et al (1997) Importance of bleomycin in combination chemotherapy for good-prognosis testicular nonseminoma: a randomized study of the European organization for research and treatment of cancer genitourinary tract cancer cooperative group. J Clin Oncol 15:1837–1843
Albers P, Weissbach L, Krege S et al (2004) Prediction of necrosis after chemotherapy of advanced germ cell tumors: results of a prospective multicenter trial of the German testicular cancer study group. J Urol 171:1835–1838
Debono DJ, Heilman DK, Einhorn LH et al (1997) Decision analysis for avoiding postchemotherapy surgery in patients with disseminated nonseminomatous germ cell tumors. J Clin Oncol 15:1455–1464
Hartmann JT, Candelaria M, Kuczyk MA et al (1997) Comparison of histological results from the resection of residual masses at different sites after chemotherapy for metastatic non-seminomatous germ cell tumours. Eur J Cancer 33:843–847
Jacobsen NE, Foster RS, Donohue JP (2007) Retroperitoneal lymph node dissection in testicular cancer. Surg Oncol Clin N Am 16:199–220
International germ cell consensus classification: a prognostic factor-based staging system for metastatic germ cell cancers. International germ cell cancer collaborative group. J Clin Oncol 15:594–603, 1997
Motzer RJ, Amsterdam A, Prieto V et al (1998) Teratoma with malignant transformation: diverse malignant histologies arising in men with germ cell tumors. J Urol 159:133–138
Fizazi K, Tjulandin S, Salvioni R et al (2001) Viable malignant cells after primary chemotherapy for disseminated nonseminomatous germ cell tumors: prognostic factors and role of postsurgery chemotherapy–results from an international study group. J Clin Oncol 19:2647–2657
Carver BS, Serio AM, Bajorin D et al (2007) Improved clinical outcome in recent years for men with metastatic nonseminomatous germ cell tumors. J Clin Oncol 25:5603–5608
Spiess PE, Brown GA, Pisters LL et al (2006) Viable malignant germ cell tumor in the postchemotherapy retroperitoneal lymph node dissection specimen: can it be predicted using clinical parameters? Cancer 107:1503–1510
Carver BS, Sheinfeld J (2009) Management of post-chemotherapy extra-retroperitoneal residual masses. World J Urol 27:489–492
Spiess PE, Tannir NM, Tu SM et al (2007) Viable germ cell tumor at postchemotherapy retroperitoneal lymph node dissection: can we predict patients at risk of disease progression? Cancer 110:2700–2708
Fizazi K, Oldenburg J, Dunant A et al (2008) Assessing prognosis and optimizing treatment in patients with postchemotherapy viable nonseminomatous germ-cell tumors (NSGCT): results of the sCR2 international study. Ann Oncol 19:259–264
Sheinfeld J (2002) The role of adjunctive postchemotherapy surgery for nonseminomatous germ-cell tumors: current concepts and controversies. Semin Urol Oncol 20:262–271
Stephenson AJ, Bosl GJ, Motzer RJ et al (2005) Retroperitoneal lymph node dissection for nonseminomatous germ cell testicular cancer: impact of patient selection factors on outcome. J Clin Oncol 23:2781–2788
Sheinfeld J, Bajorin D (1993) Management of the postchemotherapy residual mass. Urol Clin North Am 20:133–143
Fox EP, Weathers TD, Williams SD et al (1993) Outcome analysis for patients with persistent nonteratomatous germ cell tumor in postchemotherapy retroperitoneal lymph node dissections. J Clin Oncol 11:1294–1299
Baniel J, Foster RS, Rowland RG et al (1995) Complications of post-chemotherapy retroperitoneal lymph node dissection. J Urol 153:976–980
Baniel J, Sella A (1999) Complications of retroperitoneal lymph node dissection in testicular cancer: primary and post-chemotherapy. Semin Surg Oncol 17:263–267
Acknowledgements
No financial support to declare.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that there is no conflict of interest regarding the publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Altan, M., Haberal, H.B., Aşçı, A. et al. Determination of risk factors for progression in patients with viable tumor at post-chemotherapy lymph node dissection due to disseminated non-seminomatous germ-cell tumors. Int J Clin Oncol 26, 186–191 (2021). https://doi.org/10.1007/s10147-020-01786-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-020-01786-8