
Abstract
Background
Radium-223 (Ra-223) is a targeted alpha therapy that has been shown to prolong overall survival (OS) in patients with metastatic castration-resistant prostate cancer (mCRPC) with bone metastases. However, prognosis after Ra-223 administration varies among patients. The aim of the present study was to assess risk factors associated with the poor prognosis of patients treated with Ra-223.
Methods
We retrospectively reviewed patients’ records of treatment with Ra-223 between October 2016 and December 2019. All patients had mCRPC, bone metastasis, and no known visceral metastases, and received up to six cycles of Ra-223 (55 kBq/kg). Prognostic factors for OS were analyzed by Cox proportional hazards model and log-rank test.
Results
We identified 42 patients who received at least one cycle of Ra-223 (median six cycles, range 1–6). Approximately two-thirds of patients had received at least two lines of therapy for mCRPC. The median age was 74 years, and the median follow-up duration was 13.6 months. The median OS time was 16.6 months. On multivariate analysis, PSA doubling time (PSADT) (0–3 months) at baseline, number of bone metastases (≥ 20), and treatment line of Ra-223 (4th–5th line) remained significantly correlated with the poor OS (HR 4.354, P = 0.003; HR 2.855, P = 0.020; and HR 4.871, P = 0.001, respectively).
Conclusions
Our study demonstrated that a shorter PSADT, a heavier volume of bone metastases, and a later treatment line before Ra-223 are poor prognostic factors for mCRPC patients. These newly discovered risk factors may help select patients who potentially have long-term OS after Ra-223 treatment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Metastatic prostate cancer has a poor prognosis of 42 months for overall survival (OS) [1] owing to the development of metastatic castration-resistant prostate cancer (mCRPC). Since 2010, the number of life-prolonging treatments for mCRPC has increased from one (docetaxel) to six, dramatically expanding treatment options and creating the potential to combine therapies for mCRPC. These options are docetaxel [2], sipuleucel-T [3], cabazitaxel [4], abiraterone acetate (abiraterone) [5], enzalutamide [6], and radium-223 dichloride (Ra-223), a targeted alpha therapy [7]; each improved OS versus placebo or standard care in randomized controlled trials. In the phase III ALSYMPCA trial, Ra-223 versus placebo significantly prolonged OS [7] and delayed time to first symptomatic skeletal event [8], resulting in a meaningful improvement in the quality of life [9]. It was also well tolerated, with a low myelosuppression incidence [10]. However, the ideal patient populations and timing for Ra-223 administration remain unclear. In mCRPC patients with Ra-223 treatment, various clinical factors associated with poor prognosis have been reported, including poor performance status (PS), high PSA, high alkaline phosphatase (ALP), high lactate dehydrogenase (LDH), anemia, lower number of Ra-223 injections (< 5), total ALP or LDH increase at 12 weeks, and bone scan index [11,12,13,14], but a conclusion still has not been reached. Furthermore, in real-world medical care, we sometimes encounter mCRPC patients with rapid progression of disease after Ra-223 administration, yet there have been few reports regarding this. In the present study, we investigated risk factors correlated with the poor prognosis of mCRPC patients with Ra-223. We demonstrated that mCRPC patients with a shorter PSA doubling time (PSADT), a heavier volume of bone metastases, and a later treatment line of Ra-223 injection had a poor prognosis. Collectively, this clinical information may help us to develop a proper strategy for Ra-223 treatment in mCRPC patients.
Materials and methods
Study design
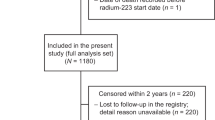
Between October 2016 and December 2019, a total of 42 mCRPC patients with Ra-223 administration were retrospectively enrolled in this study at our institution. All patients underwent Ra-223 treatment for mCRPC at our hospital. This study was approved by the institutional review board of the Osaka International Cancer Institute (No. 18044).
Forty patients were pathologically diagnosed by needle biopsy and two patients were clinically diagnosed with prostate cancer before the initial treatment. Histological diagnosis was determined based on standard hematoxylin- and eosin-stained sections. Pathological classification for Gleason scores was evaluated with the grading system proposed by the 2014 International Society of Urological Pathology (ISUP) [15]. Castration-resistant disease was defined as disease progression at a serum testosterone level of less than 50 ng per deciliter during maintenance treatment consisting of androgen-ablation therapy with a luteinizing hormone-releasing hormone agonist or antagonist. All patients were required to continue androgen-ablation therapy throughout the study. In all patients, two or more bone metastases were detected on skeletal scintigraphy or magnetic resonance imaging, and there were no known visceral metastases other than to lymph nodes before Ra-223 administration. In all patients, blood collection was performed before each administration of Ra-223 and after the final administration. Laboratory data, presence of pain, and other clinical information were collected from medical records. PS before Ra-223 treatment was evaluated by Eastern Cooperative Oncology Group performance status. PSADT was calculated by log (2) divided by the slope of the linear regression of log (PSA) over time in months [16]. When the value of PSADT was negative, it was defined as stable. All patients received Ra-223 as treatment between the first and fifth lines for mCRPC. All patients received up to six injections of Ra-223 (55 kBq/kg), which were administered at a rate of one every 4 weeks. OS was evaluated from the first administration of Ra-223 to the last follow-up point or to the day of death. Adverse events (AEs) that occurred less than 4 weeks after the final Ra-223 injection were reported only if they were determined to be related to Ra-223. AEs were graded according to the Common Terminology Criteria for Adverse Events, version 4.0.
Statistical analysis
Statistical analysis was performed using JMP Pro 15.0.0 (SAS Institute Inc., Cary, NC, USA). Results on patients were presented as median + range. Hazard ratios (HRs) for OS were estimated using the Cox proportional hazards model to investigate the association between survival and predictive variables. OS rate was calculated using the Kaplan–Meier method. Differences among different groups were assessed by the log-rank test and were considered statistically significant when the P value was less than 0.05.
Results
Patient characteristics and outcomes of Ra-223 treatment
The characteristics of 42 patients are summarized in Table 1. The median age of all patients was 74 years (range 56–90 years). Most patients had received at least two lines of therapy including new anti-androgens (abiraterone, enzalutamide) and taxanes (docetaxel, cabazitaxel). In line with the number of Ra-223 treatments for mCRPC, the number of lines under three was 28 (66.7%), and that over four was 14 (33.3%). In PSADT, six patients had stable values and one patient had missing data. Regarding cycle numbers of Ra-223, 12 (28.6%) patients had under four cycles, and one (2.4%) patient had five, while 29 (69.0%) patients completed six cycles. The reasons for the lower cycle numbers of Ra-223 (under four) were mCRPC progression (n = 10) and the onset of comorbidities (n = 2). Four patients developed the progressive disease at bone metastatic lesions after receiving one to four cycles of Ra-223 and died within 6 months after initial injection of Ra-223. Subsequent therapy after Ra-223 included 11 (26.2%) cases that received abiraterone, 14 (33.3%) of enzalutamide, 9 (21.4%) of docetaxel, and 12 (28.6%) of cabazitaxel.
Survival and prognostic factors in mCRPC patients with Ra-223 administration
At the time of analysis, 16 (38.1%) patients were alive, while 25 (59.5%) patients had died of cancer progression and one patient of comorbidity. Median follow-up time from the first Ra-223 administration was 13.6 months (range 0.6–38.0 months). Median OS time was 16.6 months (Fig. 1).

Overall survival curve of 42 mCRPC patients with Ra-223 administration by Kaplan–Meier analysis. mCRPC metastatic castration-resistant prostate cancer, Ra-223 radium-223
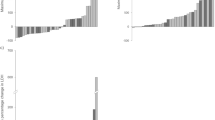
First, we evaluated the prognostic factors for mCRPC patients with Ra-223 injection. Multivariate analysis consisting of factors before Ra-223 injection showed that a short value of PSADT, the number of bone metastases (≥ 20), and the treatment line of Ra-223 (4th–5th line) were significantly associated with poor OS (HR 4.354, P = 0.003; HR 2.855, P = 0.020; and HR 4.871, P = 0.001, respectively; Table 2). Patients with a PSADT of 3 months or less had a significantly shorter OS than those with a PSADT of more than 3 months or who were stable, with an estimated median survival of 12.5 months versus 21.0 months (P = 0.022; Fig. 2a). Similarly, the number of bone metastases and the treatment line of Ra-223 were significantly associated with OS (≥ 20 vs. < 20, median survival 14.2 vs 21.0 months, P = 0.007; 4th–5th line vs. 1st–3rd, median survival 9.6 vs 21.0 months, P < 0.001, respectively; Fig. 2b, c). Next, we evaluated whether the model using these three risk factors classified the prognosis of mCRPC patients. We set short PSADT before Ra-223 administration (< 3.0 months), number of bone metastases (≥ 20), and treatment line of Ra-223 (4th–5th line) as each risk factor. Using the Kaplan–Meier method and log-rank test, we found that the number of these risk factors was significantly associated with OS (0–1 factors (n = 26) vs 2 (n = 11) vs 3 (n = 4), P < 0.001; Fig. 2d).

Short PSADT before Ra-223 administration (< 3.0 months), number of bone metastases (≥ 20), and treatment line of Ra-223 (4th–5th line) were associated with poor OS. OS was analyzed in 42 mCRPC patients by Kaplan–Meier analysis and log-rank test. PSADT was not available in one patient. Association of PSADT (a), number of bone metastases (b), and treatment line (c) for OS. d A model using three risk factors of short PSADT before Ra-223 administration (< 3.0 months), number of bone metastases (≥ 20), and treatment line of Ra-223 (4th–5th line) classified the prognosis of mCRPC patients. mCRPC metastatic castration-resistant prostate cancer, OS overall survival, PSADT PSA doubling time, Ra-223 radium-223
Adverse events caused by Ra-223 treatment
Finally, we evaluated AEs caused by Ra-223 administration. More than one AE (of any grade) occurred in 22 of 42 (52.4%) patients, and 10 (23.8%) patients had grade 3–4 AEs during the period of observation. The most common AE (any grade) was lymphocytopenia (n = 12, 28.6%), followed by anemia (n = 11, 26.2%), neutropenia (n = 3, 7.1%), thrombocytopenia (n = 3, 7.1%), and osteonecrosis of the jaw (n = 1, 2.4%). In AEs of grades 3–4, the most common event was anemia (n = 5, 11.9%), followed by lymphocytopenia (n = 2, 4.8%), thrombocytopenia (n = 2, 4.8%), neutropenia (n = 1, 2.4%), and osteonecrosis of the jaw (n = 1, 2.4%).
Discussion
Currently, there are many choices of treatment that include Ra-223 for mCRPC in clinical guidelines [17, 18]. However, there are no reliable indicators that enable clinicians to administer Ra-223 to mCRPC patients at the most ideal timepoint. Various factors, such as PS, PSA, ALP, LDH, hemoglobin, number of Ra-223 injections, and bone scan index, have been reported as prognostic factors of Ra-223 treatment [11,12,13,14], yet they remain inconclusive. According to a large international early access program, patients with less advanced mCRPC are more likely to complete Ra-223 treatment and to achieve better OS [19]. Because the prescription dose is six injections over 20 weeks, patients with a poor prognosis may not benefit enough from Ra-223 treatment. Therefore, we examined the clinical indicators for the poor prognosis of Ra-223 administration in mCRPC patients.
Through the prognostic analysis of Ra-223 treatment in our cohort, we demonstrated novel findings that may have utility in clinical settings. Multivariate analysis showed that shorter PSADT before Ra-223, number of bone metastases (≥ 20), and later treatment line of Ra-223 were significantly associated with poor OS. Previous studies have reported various risk factors of pre-, simultaneous-, and post-Ra-223 treatment for OS, yet there were no reports of the association between PSADT and poor OS, to the best of our knowledge. PSADT is well reported as a prognostic marker for patients with both hormone-sensitive prostate cancer and castration-resistant prostate cancer [20,21,22]. We found that mCRPC patients with a shorter PSADT at baseline had a poor prognosis after Ra-223 treatment, therefore, Ra-223 treatment may have a limited survival benefit for these patients. Regarding the number of bone metastases, previous reports also showed that mCRPC patients with a higher volume of bone metastases had a poorer prognosis after Ra-223 administration [23]. As well as this study, another study reported that early treatment line for Ra-223 was associated with good prognosis in mCRPC patients [24]. When we assessed the OS model using these three factors, patients with zero or one factor had a clearly longer survival than those with two or more factors. Although Ra-223 was reported to be well tolerated in mCRPC patients [10, 25], physicians should bear in mind the importance of careful monitoring of patients, especially those with these risk factors, after Ra-223 administration. In fact, four patients in this study showed rapid progression of bone diseases after one to four cycles of Ra-223 administration.
There are some apparent limitations to this study. Our study was retrospective and recruited a relatively small number of patients. Backgrounds of patients such as their history of treatments for mCRPC and number of lines of Ra-223 in their treatment course of mCRPC were not aligned. Therefore, there is the possibility that treatments before or after Ra-223 might have had some impacts on OS. In addition, risk factors identified in the current study are poor prognostic factors after Ra-223 administration, but do not necessarily indicate poor efficacy of Ra-223. Some patients with one of these factors may have clinical benefit from Ra-223 treatment. Further investigations are needed to validate our results in larger numbers of patients through multi-institutional studies.
In conclusion, our results imply that shorter PSADT, the heavier volume of bone metastases, and later treatment line of Ra-223 are poor prognostic indicators for mCRPC patients treated with Ra-223. These newly discovered risk factors may be utilized to select patients who potentially have long-term OS after Ra-223 treatment. Nevertheless, further investigations into the optimization of patients to receive Ra-223 treatment are needed to maximize the clinical benefits of this therapy.
Abbreviations
- AE:
-
Adverse event
- ALP:
-
Alkaline phosphatase
- HR:
-
Hazard ratio
- mCRPC:
-
Metastatic castration-resistant prostate cancer
- LDH:
-
Lactate dehydrogenase
- OS:
-
Overall survival
- OR:
-
Odds ratio
- PS:
-
Performance status
- PSADT:
-
PSA doubling time
- Ra-223:
-
Radium-223
References
James ND, Spears MR, Clarke NW et al (2015) Survival with newly diagnosed metastatic prostate cancer in the “Docetaxel Era”: data from 917 patients in the control arm of the STAMPEDE Trial (MRC PR08, CRUK/06/019). Eur Urol 67:1028–1038
Tannock IF, de Wit R, Berry WR et al (2004) Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 351:1502–1512
Kantoff PW, Higano CS, Shore ND et al (2010) Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med 363:411–422
de Bono JS, Oudard S, Ozguroglu M et al (2010) Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 376:1147–1154
de Bono JS, Logothetis CJ, Molina A et al (2011) Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med 364:1995–2005
Scher HI, Fizazi K, Saad F et al (2012) Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med 367:1187–1197
Parker C, Nilsson S, Heinrich D et al (2013) Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 369:213–223
Sartor O, Coleman R, Nilsson S et al (2014) Effect of radium-223 dichloride on symptomatic skeletal events in patients with castration-resistant prostate cancer and bone metastases: results from a phase 3, double-blind, randomised trial. Lancet Oncol 15:738–746
Nilsson S, Cislo P, Sartor O et al (2016) Patient-reported quality-of-life analysis of radium-223 dichloride from the phase III ALSYMPCA study. Ann Oncol 27:868–874
Vogelzang NJ, Coleman RE, Michalski JM et al (2017) Hematologic safety of radium-223 dichloride: baseline prognostic factors associated with myelosuppression in the ALSYMPCA trial. Clin Genitourin Cancer 15:42–52.e8
Saad F, Carles J, Gillessen S et al (2016) Radium-223 and concomitant therapies in patients with metastatic castration-resistant prostate cancer: an international, early access, open-label, single-arm phase 3b trial. Lancet Oncol 17:1306–1316
Sartor O, Coleman RE, Nilsson S et al (2017) An exploratory analysis of alkaline phosphatase, lactate dehydrogenase, and prostate-specific antigen dynamics in the phase 3 ALSYMPCA trial with radium-223. Ann Oncol 28:1090–1097
McKay RR, Jacobus S, Fiorillo M et al (2017) Radium-223 use in clinical practice and variables associated with completion of therapy. Clin Genitourin Cancer 15:e289–e298
Naito M, Ukai R, Hashimoto K (2019) Bone scan index can be a useful biomarker of survival outcomes in patients with metastatic castration-resistant prostate cancer treated with radium-223. Cancer Rep 2:e1203
Epstein JI, Egevad L, Amin MB et al (2016) The 2014 International Society of Urological Pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma: definition of grading patterns and proposal for a new grading system. Am J Surg Pathol 40:244–252
Memorial Sloan-Kettering Cancer Center cancer information: prostate cancer nomogram. https://www.mskcc.org/nomograms/prostate/psa_doubling_time. Accessed 1 May 2020
The Prostate Cancer Guidelines; European Association of Urology in 2020. https://uroweb.org/guideline/prostate-cancer/. Accessed 1 May 2020
NCCN Guidelines Version 1. 2020 Prostate Cancer. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf. Accessed 1 May 2020
Saad F, Gillessen S, Heinrich D et al (2019) Disease characteristics and completion of treatment in patients with metastatic castration-resistant prostate cancer treated with radium-223 in an international early access program. Clin Genitourin Cancer 17:348–355.e5
Antonarakis ES, Chen Y, Elsamanoudi SI et al (2011) Long-term overall survival and metastasis-free survival for men with prostate-specific antigen-recurrent prostate cancer after prostatectomy: analysis of the Center for Prostate Disease Research National Database. BJU Int 108:378–385
Oudard S, Banu E, Scotte F et al (2007) Prostate-specific antigen doubling time before onset of chemotherapy as a predictor of survival for hormone-refractory prostate cancer patients. Ann Oncol 18:1828–1833
Stewart AJ, Scher HI, Chen MH et al (2005) Prostate-specific antigen nadir and cancer-specific mortality following hormonal therapy for prostate-specific antigen failure. J Clin Oncol 23:6556–6560
Fosbøl MØ, Petersen PM, Kjaer A et al (2018) 223 Ra therapy of advanced metastatic castration-resistant prostate cancer: quantitative assessment of skeletal tumor burden for prognostication of clinical outcome and hematologic toxicity. J Nucl Med 59:596–602
Vidal M, Delgado A, Martinez C et al (2020) Overall survival prediction in metastatic castration-resistant prostate cancer treated with radium-223. Int Braz J Urol 46:599–611
Parker CC, Coleman RE, Sartor O et al (2018) Three-year safety of radium-223 dichloride in patients with castration-resistant prostate cancer and symptomatic bone metastases from phase 3 randomized alpharadin in symptomatic prostate cancer trial. Eur Urol 73:427–435
Acknowledgements
The authors wish to thank the patients and their families for participating in this study, as well as the staff for supporting the study. We also thank H. Nikki March, PhD, from Edanz Group (https://www.edanzediting.com/ac) for editing a draft of this manuscript.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
KN received speaker honoraria from Astellas, Novartis and Bayer; research funding from Bayer outside the submitted work. Remaining authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Yamamoto, Y., Okuda, Y., Kanaki, T. et al. Clinical indicators for predicting prognosis after radium-223 administration in castration-resistant prostate cancer with bone metastases. Int J Clin Oncol 26, 192–198 (2021). https://doi.org/10.1007/s10147-020-01776-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-020-01776-w