
Abstract
Objective
This study aimed to evaluate the efficacy and toxicity of 4-day chemotherapy with methotrexate, etoposide, and actinomycin D (MEA) for patients who were diagnosed with choriocarcinoma and high-risk gestational trophoblastic neoplasia (GTN).
Methods
Between January 1999 and December 2015, 29 patients were treated with 4-day MEA after being diagnosed with choriocarcinoma or high-risk GTN. Complete remission to 4-day MEA and adverse effects were retrospectively evaluated.
Results
The complete remission rates were 79.3% (23/29) and 87.5% (21/24) in all patients and in those who received 4-day MEA as first-line therapy, respectively. Of six patients who developed drug resistance to 4-day MEA, three patients showed complete remission by other treatments, while the other three patients died of the disease. The major adverse effects were leukocytopenia, anemia, and nausea. Of 23 patients who were cured with 4-day MEA, treatment was changed to the etoposide and actinomycin D (EA) regimen in 14 patients, because of leukocytopenia, hepatotoxicity, and stomatitis. Among 20 patients who required hormonal therapy, 15 patients showed normal menstrual cycles after therapy. Five patients had nine conceptions (seven term live births and two spontaneous abortions). No babies were premature or had low birth weight nor did they have congenital anomalies.
Conclusion
The results suggest that the efficacy and the adverse effects of 4-day MEA for choriocarcinoma and high-risk GTN may be the same level as EMA/CO. However, further study will be needed for determining the criteria of changing the treatment regimen from 4-day MEA to the EA regimen.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Multi-agent chemotherapy is necessary for treating choriocarcinoma, and etoposide, methotrexate and actinomycin D, alternating with cyclophosphamide and vincristine (EMA/CO) [1,2,3,4,5,6,7], and methotrexate, etoposide and actinomycin D (MEA) [8,9,10] are widely accepted as first-line treatment regimens for choriocarcinoma and high-risk gestational trophoblastic neoplasia (GTN). The remission rates after treatment with these regimens are similar [1,2,3,4,5,6,7,8,9,10,11]. However, adverse effects due to chemotherapy should also be considered as an aspect of the patient’s health. EMA/CO is more commonly used worldwide than MEA, but the individual efficacy of cyclophosphamide or vincristine for GTN is unclear [8, 9]. The advantage of administering MEA is the use of three drugs, any one of which will be effective for GTN. Three protocols of MEA have been reported with different doses of drugs and for different number of days: “5-day MEA” (methotrexate 450 mg/body on day 1, etoposide 100 mg/body on days 1–5, and actinomycin D 0.5 mg/body on days 1–5; every 14–21 days) [8], “2-day MEA” (methotrexate 300 mg/m2 on day 1, etoposide 100 mg/m2 on days 1–2, and actinomycin D 12 μg/kg on days 1–2; every 14–21 days) [9], and “M/EA” (methotrexate 300 mg/m2 on day 1, etoposide 100 mg/m2 on days 9–11, and actinomycin D 0.5 mg/body on days 9–11; every 18 days) [10]. Since 1999, our institution has been treating patients with choriocarcinoma and high-risk GTN with “4-day MEA”, a shortened regimen of 5-day MEA, to reduce severe adverse effects. Therefore, in this study, we evaluated the efficacy and toxicity of 4-day MEA treatment for patients with choriocarcinoma and high-risk GTN.
Materials and methods
Patients
Twenty-nine patients who were treated with 4-day MEA at Nagoya University Hospital between January 1999 and December 2015 after being diagnosed with choriocarcinoma pathologically or high-risk GTN clinically [12] were included in the study. The exclusion criteria were having never been pregnant, diagnosis of non-gestational choriocarcinoma using deoxyribonucleic acid analysis, and transferring to other hospitals before the completion of the treatment. Pathological diagnosis was possible when patients underwent surgery or biopsy and their pathological specimens were analyzed. Patients who did not undergo any surgery were diagnosed clinically as GTN and classified into high risk according to the International Federation of Gynecology and Obstetrics (FIGO) 2000 staging and risk factor scoring system for GTN [12]. Before treatment, all patients underwent physical examinations, serum human chorionic gonadotropin (hCG) level measurement, complete blood count analysis, renal and liver function tests, transvaginal ultrasonography, chest radiography, and computed tomography of the chest and abdomen. Total hCG in serum samples was measured via enzyme immunoassay using an αhCG monoclonal antibody and a βhCG-CTP monoclonal antibody (SRL Inc., Tokyo, Japan). It is critically required to detect all isoforms of hCG to management of GTN [13]. Patients received hormonal therapy using estrogen when pituitary hCG affected the results of hCG measurement or the menstrual cycle did not resume after chemotherapy. Patients were permitted to become pregnant, if they wished to, when the hCG level had been under the normal limit (≤ 0.5 IU/L) for 12 months after the completion of their treatment. The data of patients including the reproductive status, subsequent pregnancies, and the pregnancy outcome were retrospectively collected from patients’ records. This study was approved by the Ethics Committee of Nagoya University Hospital (approval number 2013-0078).
Treatment protocol
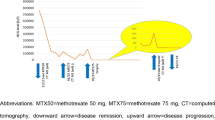
The protocol of the 4-day MEA regimen is detailed in Table 1. Etoposide and actinomycin D are administered from day 1 to day 4 based on the protocol of 5-day MEA [8]. The interval between cycles was set as 14 days. The serum hCG level was measured once or twice a week including just before each cycle. Patients who had constant or increasing serum hCG levels over two cycles of treatment were defined as having drug resistance to the regimen. After the serum hCG level reached the normal limit (≤ 0.5 IU/L), four cycles of consolidation chemotherapy were performed and complete remission was defined as the hCG level ≤ 0.5 IU/L during the consolidation chemotherapy. When adverse effects were too severe to resolve by day 21 or to continue chemotherapy, the regimen of the next cycle was changed to EA (etoposide 100 mg/body on days 1–4, and actinomycin D 0.5 mg/body on days 1–4).
Adverse effects
Adverse effects due to 4-day MEA were registered according to the Common Terminology Criteria for Adverse Events version 4.0. Granulocyte colony-stimulating factor (filgrastim 50 μg/m2, lenograstim 2 μg/kg, or nartograstim 1 μg/kg) was administered when the absolute neutrophil count (ANC) was < 1000/μL, and prophylactically used during days 11–13 when the ANC was < 1500/μL to provide the next cycle as scheduled. After 2014, pegfilgrastim (3.6 mg/body) was injected on day 6 of 4-day MEA when the prior cycle was associated with severe neutropenia (< 500/μL) or neutropenic fever.
Results
Clinical features of patients with choriocarcinoma and high-risk GTN
The mean age of 29 patients was 36.4 years (range 17–70 years; Table 2). Pathological diagnosis of choriocarcinoma was done in 12 patients (41.4%) and clinical diagnosis in 17 (58.6%). Although antecedent pregnancy was hydatidiform mole in 27.6% of patients, 44.8% of patients had a history of hydatidiform moles. According to the 2000 FIGO staging, nine patients (31.0%) had stage I tumors, nine patients (31.0%) had stage III tumors, and 11 patients (38.0%) had stage IV tumors. The average FIGO/WHO prognostic risk score was 11.0. The mean pre-treatment serum hCG level was 24,217.8 IU/L (range 96.4–1,494,610 IU/L) (Table 2). Twenty-four patients had not received any prior chemotherapy for choriocarcinoma or high-risk GTN except for MEA. Five patients had previously received multiple-agent chemotherapy such as EMA/CO; MAC (methotrexate, actinomycin D and cyclophosphamide); and EP (etoposide and cisplatin) regimens [14]. In addition to chemotherapy, 11 patients underwent surgery, including hysterectomy in two patients, wedge resection of choriocarcinoma in the uterus in one, partial pneumonectomy in five, wedge resection of choriocarcinoma in the brain in two, and small intestinal resection in one. Four patients received radiotherapy for brain metastases (whole-brain radiation for one patient and gamma knife therapy for the other three).
Response to 4-day MEA
The average follow-up time was 53.9 months (range 1–152 months). Twenty-three patients (79.3%) achieved complete remission; although three of them experienced relapse, they were cured again using 4-day MEA and surgery. The complete remission rate among 24 patients who received the 4-day MEA regimen as the first-line treatment was 87.5% (Table 3). Although six patients (20.7%) developed drug resistance to 4-day MEA, three of them were cured completely using surgery, radiotherapy, or FA (5-fluorouracil and actinomycin D) [15]. The other three patients, two choriocarcinoma and one high-risk GTN of stage IV, were treated with EP/EMA (etoposide and cisplatin/etoposide, methotrexate, and actinomycin D) [16], FA, EMA/CO, TP/TE (paclitaxel and cisplatin/paclitaxel and etoposide) [17], biweekly TP (paclitaxel and cisplatin), and high-dose ICE (ifosfamide, carboplatin and etoposide) with autologous peripheral blood stem cell transplantation [14], but they died of the disease.
Adverse effects
We evaluated the drug-related adverse effects of 183 courses of 4-day MEA in 29 patients (Table 4). The major adverse effects were leukocytopenia (82.5%) and anemia (77.6%). Grade 4 toxicity was observed only in bone marrow-related adverse effects namely leukocytopenia, anemia, and thrombocytopenia. Although anemia and thrombocytopenia were mostly grade 1 or 2, patients underwent a blood transfusion when they had grade 3–4 anemia or thrombocytopenia. Granulocyte colony-stimulating factor was used for grade 3–4 leukocytopenia, which occurred in 49.2% of treatment cycles. Hepatotoxicity, stomatitis, and nausea were seen in 53.6%, 60.7%, and 63.4% of cycles, respectively, and they were mostly grade 1 or 2.
The mean interval between cycles of 4-day MEA was 17.0 days (range 13–22 days). All 29 patients underwent 207 cycles of MEA and 77 cycles of EA, and the reasons for regimen change were stomatitis (37.5%), hepatotoxicity (31.3%), leukocytopenia (25.0%), and sepsis (6.3%). Twenty-three patients achieved complete remission after 4-day MEA including EA without any therapeutic surgery. Nine patients underwent treatment with only the 4-day MEA regimen, but 14 patients needed the EA regimen with an average of 4.0 cycles. The mean number of total cycles was 10.5, 11.1, and 10.1 in the 23 patients, patients treated with only 4-day MEA, and patients treated with 4-day MEA and EA, respectively (Table 5).
Reproductive status after treatment
We evaluated the reproductive status of patients after chemotherapy including pregnancy and recovery of menstruation (Table 6). Hysterectomy was performed in four patients for treating choriocarcinoma (n = 2) and previous hydatidiform mole (n = 2). Among 26 patients who finally achieved complete remission, 25 patients required hormonal therapy with estrogen, during chemotherapy, for suppressing pituitary hCG. Hormonal therapy was started after an average of 6.2 cycles in patients who received first-line 4-day MEA therapy. After hormone therapy for 6–18 months, the menstrual cycle was normal in 15 patients, while three patients were diagnosed with menopause. Among the three patients, one was 31 years old and she had received whole-brain radiation therapy because of metastases to the cerebellum before she was transferred to our hospital [18]. The second patient was 45 years old and underwent 8 cycles of 4-days MEA, but she had received 14 cycles of chemotherapy for post-molar GTN at 42 years of age. The third patient was 38 years old and underwent a total 35 cycles of multiple regimens such as EMA/CO, EP/EMA, FA, and MEA. Among 11 patients who hoped to bear children, five patients had nine conceptions. The outcomes of the nine pregnancies were seven term live births and two spontaneous abortions. No babies were premature or had low birth weight, nor did they have any congenital anomalies.
Discussion
The results of this study showed that the complete remission rate to 4-day MEA was 79.3% among all patients and 87.5% among patients who received first-line MEA treatment. The complete remission rates to EMA/CO were 69.2–83.6% for all patients and 67.0–90.6% for those who received first-line EMA/CO therapy [1,2,3,4,5,6,7, 11]. However, the more accurate complete remission rates to EMA/CO may be 78–79.7% and 78–80.3% for all patients and for those who received first-line EMA/CO therapy, respectively, because of the inclusion of a higher number of patients (138 and 272 patients, respectively) [3, 7]. Previous studies that evaluated three MEA regimens reported that the complete remission rates for all patients and those that received these treatments as first-line therapy were, respectively, 67.9% and 70.6% [8], 89.7% and 71% [9], and 75% and 75% [10]. These results suggest that 4-day MEA might be as effective as 5-day MEA, although the doses of etoposide and actinomycin were reduced to 80%, but the interval was shorter than 5-day MEA. However, the number of participants in each study on MEA was only 28–38; hence, further studies on MEA including a larger number of patients will be needed for comparing the effectiveness between EMA/CO and MEA, and for deciding the most appropriate regimen for MEA, considering the duration of medication and the dose of each drug.
Regarding adverse effects, the incidence of leukocytopenia and anemia was found in 82.5% and 77.6% of treatment cycles, respectively. In particular, grade 3–4 leukocytopenia was observed in 49.2% of cycles, and the incidence was higher in this study than in previous studies using other regimens. However, no patient died due to leukocytopenia, although one patient had sepsis due to urinary tract infection, because choriocarcinoma in the kidney caused bleeding after day 5 in each cycle. Severe leukocytopenia should be managed to avoid long treatment intervals that can reduce the effectiveness or result in chemotherapy failure. In this study, two methods were effective for managing severe leukocytopenia to achieve remission: prophylactic granulocyte colony-stimulating factor and tentative use of the EA regimen. After we introduced prophylactic granulocyte colony-stimulating factor in 2005, the proportion of patients in whom the regimen was changed from MEA to EA decreased from 85.7% (6/7) to 45.5% (10/22).
The reproductive status after 4-day MEA was favorable, because most patients in the reproductive age had a regular menstrual cycle after hormonal treatment. Hormonal therapy using estrogen (and progesterone) was needed for suppressing luteinizing hormone, which increased due to ovarian dysfunction. High levels of luteinizing hormone induce hCG secretion from the pituitary gland [19, 20], and pituitary hCG should be suppressed for detecting hCG levels from choriocarcinoma. In this study, the fertility rate among patients who desired babies was 45.5% (5/11 patients) and seven babies were born without any congenital abnormality. The average age of women who could not conceive was 37.3 years (range 35–41 years) at the start of treatment, higher than that of women who could (27.6 years; range 21–33 years). The fertility rate may be better after MEA than after EMA/CO, because cyclophosphamide induces ovarian failure [21]. However, it is difficult to compare the fertility rate and the rate of live births between regimens, because the demographic characteristics of patients, such as age, stage, and the number of cycles, were not the same and the number of patients was not high enough to be assessed, especially the number of patients who received MEA regimens. Goto et al. reported that the incidence of congenital anomalies was higher in patients who underwent multi-agent chemotherapy for choriocarcinoma (3/21; 14.3%) than the population-based incidence in Japan and that receiving more methotrexate was significantly associated with having babies with heart abnormalities [22]. Rustin et al. reported that 79% of patients (37/47) who underwent chemotherapy using cyclophosphamide and desired for babies had live births and that no significant difference was found in the mean amount of drugs (methotrexate, actinomycin D, vincristine, and cyclophosphamide) between patients having live births and those who did not have live births [23]. In other studies, multi-agent chemotherapy for choriocarcinoma and high-risk GTN was not associated with the incidence of malformation including heart abnormalities [3, 4, 10, 24]. These results suggest that ovarian failure and fertility may be related to the patient’s age (>35 years) rather than the kind of regimen administered to patients with choriocarcinoma.
This study has some limitations. First, the number of patients was only 29, much smaller than the number of patients in some studies on EMA/CO conducted in the United Kingdom or America. Choriocarcinoma is so rare and there is no system to allocate patients with GTN to designated medical centers for their treatment in Japan. In the Japanese health system, every general hospital or cancer center can provide chemotherapy at the desire of patients. Therefore, only a few studies have been reported on evaluation of treatments for choriocarcinoma or high-risk GTN in Japan [8, 15, 22]. Further studies are needed by including more patients and with longer follow-ups at different hospitals. Second, the criteria for changing 4-day MEA to EA were not clearly set during the study. The results of this study suggest that grade 3–4 stomatitis, grade 3–4 hepatotoxicity, and grade 4 leukocytopenia should be considered the criteria for using EA in the next cycle. Pegfilgrastim, the most effective granulocyte colony-stimulating factor product for leukocytopenia, was approved by the Japanese Ministry of Health in 2014, and it can be administered prophylactically to a patient who is expected to have grade 4 leukocytopenia. We started prophylactic granulocyte colony-stimulating factor in 2005 and it is very effective; however, we found that pegfilgrastim injections on day 6 of 4-day MEA was the most effective regimen and that it never caused leukocytopenia. To reduce hepatotoxicity and stomatitis, administration of the higher dose of folinic acid or EA regimen can be considered, but it would lead to smaller or no efficacy of methotrexate. Phase II trials may be needed in the future for determining the criteria of choriocarcinoma and high-risk GTN to use EA regimen as first-line therapy.
In conclusion, this is the first study to evaluate the efficacy and adverse effects of 4-day MEA in patients with choriocarcinoma and high-risk GTN. The complete remission rate to 4-day MEA was similar to that obtained after other MEA regimens and EMA/CO, but slightly better in patients who received first-line 4-day MEA therapy. The adverse effects after chemotherapy were well tolerated, although prophylactic granulocyte colony-stimulating factor and tentative switching to the EA regimen were needed. These results suggest that 4-day MEA may be recommended as one of the first-line treatments for choriocarcinoma and high-risk GTN, but further studies will be needed for determining the criteria for changing treatment from 4-day MEA to EA.
References
Lybol C, Thomas CM, Blanken EA et al (2013) Comparing cisplatin-based combination chemotherapy with EMA/CO chemotherapy for the treatment of high risk gestational trophoblastic neoplasia. Eur J Cancer 49(4):860–867. https://doi.org/10.1016/j.ejca.2012.09.015
Lu WG, Ye F, Shen YM et al (2008) EMA-CO chemotherapy for high-risk gestational trophoblastic neoplasia: a clinical analysis of 54 patients. Int J Gynecol Cancer 18(2):357–362. https://doi.org/10.1111/j.1525-1438.2007.00999.x
Bower M, Newlands ES, Holden L et al (1997) EMA/CO for high-risk gestational trophoblastic tumors: results from a cohort of 272 patients. J Clin Oncol 15(7):2636–2643. https://doi.org/10.1200/JCO.1997.15.7.2636
Kim SJ, Bae SN, Kim JH et al (1998) Risk factors for the prediction of treatment failure in gestational trophoblastic tumors treated with EMA/CO regimen. Gynecol Oncol 71(2):247–253. https://doi.org/10.1006/gyno.1998.5161
Escobar PF, Lurain JR, Singh DK et al (2003) Treatment of high-risk gestational trophoblastic neoplasia with etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine chemotherapy. Gynecol Oncol 91(3):552–557
Soper JT, Evans AC, Clarke-Pearson DL et al (1994) Alternating weekly chemotherapy with etoposide-methotrexate-dactinomycin/cyclophosphamide-vincristine for high-risk gestational trophoblastic disease. Obstet Gynecol 83(1):113–117
Newlands ES, Bagshawe KD, Begent RH et al (1991) Results with the EMA/CO (etoposide, methotrexate, actinomycin D, cyclophosphamide, vincristine) regimen in high risk gestational trophoblastic tumours, 1979 to 1989. Br J Obstet Gynaecol 98(6):550–557
Matsui H, Suzuka K, Iitsuka Y et al (2000) Combination chemotherapy with methotrexate, etoposide, and actinomycin D for high-risk gestational trophoblastic tumors. Gynecol Oncol 78(1):28–31. https://doi.org/10.1006/gyno.2000.5813
Soto-Wright V, Goldstein DP, Bernstein MR et al (1997) The management of gestational trophoblastic tumors with etoposide, methotrexate, and actinomycin D. Gynecol Oncol 64(1):156–159. https://doi.org/10.1006/gyno.1996.4534
Dobson LS, Lorigan PC, Coleman RE et al (2000) Persistent gestational trophoblastic disease: results of MEA (methotrexate, etoposide and dactinomycin) as first-line chemotherapy in high risk disease and EA (etoposide and dactinomycin) as second-line therapy for low risk disease. Br J Cancer 82(9):1547–1552. https://doi.org/10.1054/bjoc.2000.1176
Turan T, Karacay O, Tulunay G et al (2006) Results with EMA/CO (etoposide, methotrexate, actinomycin D, cyclophosphamide, vincristine) chemotherapy in gestational trophoblastic neoplasia. Int J Gynecol Cancer 16(3):1432–1438. https://doi.org/10.1111/j.1525-1438.2006.00606.x
Committee FO (2002) FIGO staging for gestational trophoblastic neoplasia 2000. FIGO Oncology Committee. Int J Gynaecol Obstet 77(3):285–287
Cole LA, Sutton JM (2004) Selecting an appropriate hCG test for managing gestational trophoblastic disease and cancer. J Reprod Med 49(7):545–553
Yamamoto E, Niimi K, Fujikake K et al (2016) High-dose chemotherapy with autologous peripheral blood stem cell transplantation for choriocarcinoma: a case report and literature review. Mol Clin Oncol 5(5):660–664. https://doi.org/10.3892/mco.2016.1011
Matsui H, Iitsuka Y, Suzuka K et al (2004) Salvage chemotherapy for high-risk gestational trophoblastic tumor. J Reprod Med 49(6):438–442
Newlands ES, Mulholland PJ, Holden L et al (2000) Etoposide and cisplatin/etoposide, methotrexate, and actinomycin D (EMA) chemotherapy for patients with high-risk gestational trophoblastic tumors refractory to EMA/cyclophosphamide and vincristine chemotherapy and patients presenting with metastatic placental site trophoblastic tumors. J Clin Oncol 18(4):854–859. https://doi.org/10.1200/JCO.2000.18.4.854
Wang J, Short D, Sebire NJ et al (2008) Salvage chemotherapy of relapsed or high-risk gestational trophoblastic neoplasia (GTN) with paclitaxel/cisplatin alternating with paclitaxel/etoposide (TP/TE). Ann Oncol 19(9):1578–1583. https://doi.org/10.1093/annonc/mdn181
Yamamoto E, Niimi K, Shinjo K et al (2014) Identification of causative pregnancy of gestational trophoblastic neoplasia diagnosed during pregnancy by short tandem repeat analysis. Gynecol Oncol Case Rep 9:3–6. https://doi.org/10.1016/j.gynor.2014.04.001
Birken S, Maydelman Y, Gawinowicz MA et al (1996) Isolation and characterization of human pituitary chorionic gonadotropin. Endocrinology 137(4):1402–1411. https://doi.org/10.1210/endo.137.4.8625917
Braunstein GD (2002) False-positive serum human chorionic gonadotropin results: causes, characteristics, and recognition. Am J Obstet Gynecol 187(1):217–224
Warne GL, Fairley KF, Hobbs JB et al (1973) Cyclophosphamide-induced ovarian failure. N Engl J Med 289(22):1159–1162. https://doi.org/10.1056/NEJM197311292892202
Goto S, Ino K, Mitsui T et al (2004) Survival rates of patients with choriocarcinoma treated with chemotherapy without hysterectomy: effects of anticancer agents on subsequent births. Gynecol Oncol 93(2):529–535. https://doi.org/10.1016/j.ygyno.2004.02.018
Rustin GJ, Booth M, Dent J et al (1984) Pregnancy after cytotoxic chemotherapy for gestational trophoblastic tumours. Br Med J (Clin Res Ed) 288(6411):103–106
Lok CA, van der Houwen C, ten Kate-Booij MJ et al (2003) Pregnancy after EMA/CO for gestational trophoblastic disease: a report from The Netherlands. BJOG 110(6):560–566
Acknowledgements
This work was supported by JSPS KAKENHI Grant number JP17K16845.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Sato, S., Yamamoto, E., Niimi, K. et al. The efficacy and toxicity of 4-day chemotherapy with methotrexate, etoposide and actinomycin D in patients with choriocarcinoma and high-risk gestational trophoblastic neoplasia. Int J Clin Oncol 25, 203–209 (2020). https://doi.org/10.1007/s10147-019-01540-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-019-01540-9