
Abstract
Background
High body mass index (BMI) is associated not only with a higher incidence of breast cancers but also with poorer prognosis. It is speculated that both enhanced production of estrogens and other factors associated with obesity are involved in these associations, but the biological characteristics associated with high BMI have yet to be thoroughly identified.
Methods
We studied 525 breast cancers, focusing on biological differences between tumors associated with high and low BMI and by immunohistochemically defined intrinsic subtype. Ki67 expression levels were used to differentiate luminal A from luminal B estrogen receptor (ER)+/human epidermal growth factor receptor 2 (HER2)-breast cancers.
Results
Premenopausal patients with high BMI showed a significantly higher frequency of lymph node metastasis (46.4 % vs. 22.9 %, P = 0.005) and tended to have a larger tumor size (P = 0.05) and higher nuclear grade (P = 0.07) than those with low BMI. These differences were not observed among postmenopausal patients. BMI was not associated with distribution of breast cancer subtypes, and ER, progesterone receptor (PR), and Ki67 expression levels of each subtype showed no differences between high and low BMI among premenopausal patients.
Conclusion
Higher BMI might influence aggressive tumor characteristics among premenopausal patients, but its influence on ER, PR, and Ki67 expression levels seems to be limited.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Body mass index (BMI) has been firmly established as being related to not only the incidence but also the prognosis of breast cancer. Because an increase in BMI is positively associated with breast cancer risk for postmenopausal patients but not premenopausal patients [1, 2], such an increase seems to be involved in breast cancer incidence, possibly through enhanced production of circulating estrogens [3]. This hypothesis seems to be supported by a reportedly positive association between BMI and ER-positive breast cancer risk for postmenopausal women [4]. It has further been reported that elevated BMI is significantly associated with worse prognosis, especially for pre-/perimenopausal patients [5]. Consistent with this finding, Kawai et al. [6] found that higher BMI was associated with an increase in mortality for premenopausal patients. Their analysis of subsets showed a positive association between higher BMI and worse prognosis for patients with hormonal receptor (HR)-positive tumors. In addition, enhanced BMI in their study correlated with worse prognosis only for HR-positive and for human epidermal growth factor receptor 2 (HER2)-negative but not HER2-positive or triple-negative tumors, irrespective of menopausal status [7, 8].
Thus, the effect of BMI on breast cancer incidence and prognosis seems to be restricted to ER-positive breast cancers. However, it is not yet clear why prognosis correlates with BMI of premenopausal patients. In a study by Berclaz et al. [5], a positive association between BMI and prognosis was recognized for patients treated with chemotherapy but not with endocrine therapy. Similar findings were obtained in a study reported by Sparano et al. [7] in which adjuvant chemotherapy was administered to all patients. Furthermore, according to data from the ATAC (anastrozole, tamoxifen, alone, or in combination) trial, postmenopausal women with high BMI treated with anastrozole showed significantly more distant recurrences than those with a low BMI, possibly caused by ineffective suppression of estrogen production resulting from an increase in aromatase activity in patients with high BMI [9]. Nevertheless, in spite of these findings, it is currently still unknown how adjuvant treatments including chemotherapy and endocrine therapy affect the relationship between BMI and prognosis.
If the occurrence of tumors in patients with high BMI is the result of an increase in estrogen status, these tumors are likely to be highly estrogen dependent, thus resulting in a favorable prognosis. On the other hand, a poorer prognosis for patients with high BMI may indicate that BMI plays a significant part in breast cancer etiology and prognosis by mediation through various mechanisms. To determine the crucial role of BMI, the relationship between tumor biological characteristics and BMI of patients thus needs to be thoroughly analyzed, but this issue has not yet been specifically discussed in the literature. The purpose of the study presented here was to disclose the relationship between BMI at the time of diagnosis and biological characteristics, focusing specifically on ER, PR, and Ki67 expression levels in terms of different subtypes.
Materials and methods
Patients
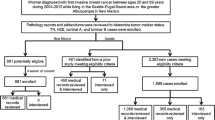
The 525 cases of invasive breast cancers treated with mastectomy or breast-conserving surgery at Hyogo College of Medicine or Tokushima Breast Clinic between 2005 and 2012 were recruited consecutively. Histological diagnosis of breast cancer was confirmed in each case (493 invasive ductal carcinomas, 15 invasive lobular carcinomas, and 19 other types), and patients with noninvasive carcinoma were excluded. This study was approved by the Ethics Committee of Hyogo College of Medicine.
Immunohistochemical staining and classification of subtypes
For classification of subtypes, immunohistochemical staining of ER, PR, HER2, and Ki67 was performed. Formalin-fixed, paraffin-embedded tissues were cut and used for immunohistochemical analyses. Staining was followed by automated immunostaining with BOND-MAX (Leica Microsystems, Tokyo, Japan) for ER and PR, and with Autostainer (Dako, Tokyo, Japan) for HER2 and Ki67. The primary antibodies used for this study were ER (1D5), PR (PgR636), HER2 (Hercep Test), and Ki67 (MIB1), all from Dako (Glostrup, Denmark). Expression levels of these proteins were determined immunohistochemically as the percentage of positive cancer cells in the nuclei for ER, PR, and Ki67, and by membrane staining for HER2. When nuclear stained cells accounted for 1 % or more, they were deemed positive for ER and PR, and HER2 positivity was defined as HER2 (3+), or HER2 (2+) and fluorescence in situ hybridization (FISH) positive. Different areas of densely stained lesions were selected microscopically, and more than 500 cancer cells were counted to determine Ki67 expression levels.
The criteria reported by Cheang et al. [10] were used to separate ER-positive and HER2-negative breast cancers into luminal A and luminal B subtypes by using a cutoff point of 14 % Ki67. The subtypes were defined as follows: luminal A, ER+/HER2−, Ki67 < 14 %; luminal B, ER+/HER2−, Ki67 ≥ 14 %; luminal/HER2, ER+/HER2+; HER2, ER−/HER2+; and triple negative (TN), ER−/HER2−.
Statistical analysis
The relationship between BMI, calculated as weight (kg) divided by height (m2), and breast cancer characteristics was determined with the chi squared test. ER, PR, and Ki67 expression levels for each subtype were calculated with the Mann–Whitney test. Differences were considered statistically significant if the P value was less than 0.05. JMP10 (SAS Institute Japan, Tokyo, Japan) was used for all analyses.
Results
Correlation between BMI and clinicopathological characteristics of breast cancers
The BMI of the postmenopausal patients (mean, 23.3 kg/m2; standard deviation, 3.8 kg/m2) was significantly higher than that of premenopausal patients (22.0, 4.1) (P < 0.0001; Table 1). We used the categorization by Kawai et al. [6] of BMI of Japanese breast cancer patients into quartiles (<21.2, ≥21.2 to <23.3, ≥23.3 to <25.8, and ≥25.8 kg/m2) to set 23.3 kg/m2 as the median cutoff and divide the patients into high- and low-BMI level groups (low, <23.3 kg/m2; high, ≥23.3 kg/m2). As shown in Table 1, there were significantly more postmenopausal (n = 153, 73.9 %) than premenopausal patients with high BMI (n = 56, 26.1 %) (P = 0.0002; Table 1).
Table 2 shows that a significantly higher percentage of premenopausal than postmenopausal patients with high BMI had lymph node metastases (46.4 % vs. 22.9 %, P = 0.005), whereas the correlation between large tumor size (37.0 % vs. 23.7 %) and high nuclear grade (grade 3, 39.0 vs. grade 1, 27.8 %) was marginally significant (P = 0.05 and P = 0.07, respectively). However, the two groups of postmenopausal patients showed no significant differences in tumor size, nuclear grade, or histological type (Table 3). More postmenopausal patients with high BMI tended to have PR-positive than PR-negative tumors (48.9 % vs. 37.8 %, P = 0.05), but there was no significant difference in HER2 positivity between the two BMI groups.
Correlation between BMI and breast cancer subtypes
We also divided breast cancers into five groups: luminal A (ER+/HER2− and Ki67 < 14 %, n = 237), luminal B (ER+/HER2− and Ki67 ≥ 14 %, n = 150), luminal/HER2 (ER+/HER2+, n = 40), HER2-positive (ER−/HER2+, n = 37), and TN (ER−/HER2−, n = 61). There were no statistically significant differences between BMI and breast cancer subtypes (Table 4) even when menopausal status was factored in.
ER, PR, and Ki67 expression levels in tumors of patients with high BMI
Findings of the analysis of ER expression levels by subtype of ER-positive breast cancers of patients in the two BMI groups are shown in Table 5. There were no significant differences between high and low BMI patients with luminal A and luminal B cancers, but ER expression of luminal/HER2 tumors of patients with high BMI [mean ± standard deviation (%), 90.4 ± 21.1] was significantly higher (P = 0.001) than that of patients with low BMI (40.5 ± 33.2). There were no differences in PR expression levels between the two BMI groups for any of the subtypes (Table 6). Because luminal A and luminal B breast cancers were initially classified according to the Ki67 expression level, we also classified luminal subtype (luminal A and luminal B), and their Ki67 expression levels were analyzed in relationship to high or low BMI (Table 7). However, there were no significant differences of Ki67 expression levels between the two BMI groups for any of the subtypes.
Discussion
The results of our study confirmed that higher BMI of premenopausal patients was significantly associated with lymph node metastasis and marginally associated with large tumor size as well as high nuclear grade. However, no such differences were detected in postmenopausal patients. In addition, we could not find any associations between BMI and breast cancer subtypes. Biglia et al. [11] found that postmenopausal patients with higher BMI (>25) showed a higher frequency of ER/PR-positive cancers than did those with lower BMI (87 % vs. 75 %), but no such difference was seen in premenopausal patients. Consistent with this observation, we found that the frequency of PR-positive tumors was marginally higher for postmenopausal patients but not for premenopausal patients with high BMI, which strongly suggests that a higher BMI influences tumor biology mediated through an increase in the production of estrogens.
Although high BMI was significantly more prevalent among postmenopausal (55.4 %) than premenopausal patients (30.3 %), the distribution of the subtypes was not significantly different for patients with either high or low BMI even when menopausal status was taken into consideration. Because ER, PR, and Ki67 expression levels of the subtypes did not differ between high and low BMI, except for ER expression levels in postmenopausal luminal/HER2 breast cancers, we hypothesize that the influence of high BMI on the biological characteristics of these tumor is limited. Alternatively, we confirmed that higher BMI was significantly associated with lymph node metastasis in premenopausal patients.
It has been reported that BMI of postmenopausal and/or premenopausal women is significantly associated with characteristics of the aggressive tumor phenotype, i.e., large tumor size, lymph node metastasis, and higher proliferation index [11, 12]. Thus, the characteristics of tumors with high BMI seem to be different from those of tumors of patients with low BMI, which are caused not only by estrogens but also by other factors. Fatty tissues secrete several cytokines including leptin, tumor necrosis factor-α, insulin-like growth factor (IGF), and interleukin-6 [13], which are likely to be involved in tumor biology-mediating crosstalk between estrogen and growth factor signaling. On the basis of the findings of these studies and of others that demonstrated that higher insulin levels and elevated C-peptide levels are associated with increased recurrence of or death from breast cancers [14, 15], the factors associated with obesity may explain, at least in part, the poorer prognosis for patients with high BMI.
The reason why there is an association between high BMI and aggressive characteristics in premenopausal but not in postmenopausal patients is currently not known. Because PR positivity of breast cancers of postmenopausal patients with high BMI was marginally higher, these cancers are likely to feature higher estrogen dependency and less aggressive phenotype. On the other hand, ER expression levels of luminal/HER2 cancers with low BMI were comparatively lower, which may indicate there is a difference in estrogen dependency between breast cancers of patients with high and low BMI.
Since the study by Berclaz et al. [5] established that an association between overall survival (OS) and obesity was restricted to patients treated by chemotherapy, it has been speculated that there is a difference in sensitivity to chemotherapy between tumors of patients with high and with low BMI. Sparano et al. [7] reported that disease-free survival (DFS) and OS were significantly poorer for HR-positive/HER2-negative/unknown cancer subsets of obese patients. High estrogen dependency and less sensitivity to chemotherapy may be one explanation of this difference [16]. However, as we found no differences in ER and PR expression levels between breast cancers with high and low BMI among premenopausal patients, we think differences in chemosensitivity between them are unlikely. Alternatively, the worse prognosis for breast cancers of premenopausal patients with high BMI could be at least partly explained by their aggressive phenotype (higher frequency of lymph node metastasis, large tumor size, and high nuclear grade).
In conclusion, we established that a difference exists between the clinicopathological characteristics of breast cancers of patients with high and low BMI. Because distribution by subtypes did not show significant differences, and ER, PR, and Ki67 expression levels were similar for tumors in premenopausal patients with high and low BMI, the influence of BMI on these biological characteristics seems to be limited. However, the fact that lymph node metastasis was significantly higher for premenopausal patients with high BMI leads us to think that differences in aggressive characteristics may in fact be influenced by BMI, mediated not through estrogens but through other factors. The main limitation of this study is that the conclusion was reached based on a study with a limited number of subjects, so that there is a clear need for verification studies comprising a large number of breast cancers as well as focusing on prognosis and drug sensitivity.
References
Renehan AG, Tyson M, Egger M et al (2008) Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371(9612):569–578
Harvie M, Hooper L, Howell AH (2003) Central obesity and breast cancer risk: a systematic review. Obes Rev 4(3):157–173
McTiernan A, Rajan KB, Tworoger SS et al (2003) Adiposity and sex hormones in postmenopausal breast cancer survivors. J Clin Oncol 21(10):1961–1966
Phipps AI, Malone KE, Porter PL et al (2008) Body size and risk of luminal, HER2-overexpressing, and triple-negative breast cancer in postmenopausal women. Cancer Epidemiol Biomarkers Prev 17(8):2078–2086
Berclaz G, Li S, Price KN et al (2004) Body mass index as a prognostic feature in operable breast cancer: the International Breast Cancer Study Group experience. Ann Oncol 15(6):875–884
Kawai M, Minami Y, Nishino Y et al (2012) Body mass index and survival after breast cancer diagnosis in Japanese women. BMC Cancer 12:149
Sparano JA, Wang M, Zhao F et al (2012) Obesity at diagnosis is associated with inferior outcomes in hormone receptor-positive operable breast cancer. Cancer (Phila) 118(23):5937–5946
Dawood S, Lei X, Litton JK et al (2012) Impact of body mass index on survival outcome among women with early stage triple-negative breast cancer. Clin Breast Cancer 12(5):364–372
Sestak I, Distler W, Forbes JF et al (2010) Effect of body mass index on recurrences in tamoxifen and anastrozole treated women: an exploratory analysis from the ATAC trial. J Clin Oncol 28(21):3411–3415
Cheang MC, Chia SK, Voduc D et al (2009) Ki67 index, HER2 status, and prognosis of patients with luminal B breast cancer. J Natl Cancer Inst 101(10):736–750
Biglia N, Peano E, Sgandurra P et al. (2013) Body mass index (BMI) and breast cancer: impact on tumor histopathologic features, cancer subtypes and recurrence rate in pre and postmenopausal women. Gynecol Endocrinol 29(3):263–267
Daling JR, Malone KE, Doody DR et al (2001) Relation of body mass index to tumor markers and survival among young women with invasive ductal breast carcinoma. Cancer (Phila) 92(4):720–729
Goodwin PJ, Ennis M, Pritchard KI et al (2002) Fasting insulin and outcome in early-stage breast cancer: results of a prospective cohort study. J Clin Oncol 20(1):42–51
Goodwin PJ, Ennis M, Bahl M et al (2009) High insulin levels in newly diagnosed breast cancer patients reflect underlying insulin resistance and are associated with components of the insulin resistance syndrome. Breast Cancer Res Treat 114(3):517–525
Irwin ML, Duggan C, Wang CY et al (2011) Fasting C-peptide levels and death resulting from all causes and breast cancer: the health, eating, activity, and lifestyle study. J Clin Oncol 29(1):47–53
Viale G, Regan MM, Maiorano E et al (2008) Chemoendocrine compared with endocrine adjuvant therapies for node-negative breast cancer: predictive value of centrally reviewed expression of estrogen and progesterone receptors. International Breast Cancer Study Group. J Clin Oncol 26(9):1404–1410
Conflict of interest
Y. Miyoshi has received honoraria from Sanofi, AstraZeneca K.K., and GlaxoSmithKline K.K. T. Katagiri is a board member of Oncotherapy Science Co. Ltd. The other authors declare that they have no conflicts of interest in this article.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Yanai, A., Miyagawa, Y., Murase, K. et al. Influence of body mass index on clinicopathological factors including estrogen receptor, progesterone receptor, and Ki67 expression levels in breast cancers. Int J Clin Oncol 19, 467–472 (2014). https://doi.org/10.1007/s10147-013-0585-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-013-0585-y