
Abstract
Antibiotics are essential agents that have greatly reduced human mortality due to infectious diseases. Their use, and sometimes overuse, have increased over the past several decades in humans, veterinary medicine and agriculture. However, the emergence of resistant pathogens is becoming an increasing problem that could result in the re-emergence of infectious diseases. Antibiotic prescription in human medicine plays a key role in this phenomenon. Under selection pressure, resistance can emerge in the commensal flora of treated individuals and disseminate to others. However, even if the effects of antimicrobial use on resistance is intuitively accepted, scientific rationales are required to convince physicians, legislators and public opinion to adopt appropriate behaviours and policies. With this review, we aim to provide an overview of different epidemiological study designs that are used to study the relationship between antibiotic use and the emergence and spread of resistance, as well as highlight their main strengths and weaknesses.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction: setting the scene
Antibiotics are essential agents in human medicine. Along with hygiene and vaccination, their discovery in the 1940s changed the patterns of major human diseases, ending the era of ‘infectious diseases’ and beginning the era of chronic and degenerative diseases [1–3]. This epidemiological transition [1] led to a decrease in infantile mortality and increase in life expectancies. However, we are now facing a new transition involving the re-emergence of infectious diseases and specific concerns regarding resistant pathogens [3]. The use, and sometimes overuse, of antibiotics in humans, veterinary medicine and agriculture have provided selective pressure favouring the emergence and spread of resistant microorganisms [4].
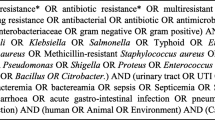
Antibiotic use in human medicine might have serious implications at both individual and population levels (Fig. 1). It might initially increase a patient’s risk of colonisation or infection with resistant organisms. Under selection pressure, commensal or pathogenic microorganisms might acquire new resistance mechanisms and pre-existing resistant microorganisms might increase. In addition, the colonisation resistance of commensal flora will be impaired, leading to increased susceptibility to colonisation with new and resistant microorganisms. Antibiotic use may also increase the risk of colonisation or infection with resistant organisms in people who have not received antibiotics. Indeed, the increased reservoir of resistant organisms among antibiotic users will disseminate into the community, increasing the probability that others will acquire resistant microorganisms [5].

Role of antibiotic pressure on the emergence and spread of resistant microorganisms in commensal microflora at the individual and population levels. A Acquisition of new resistant mechanisms among commensal flora under antibiotic pressure. B Rising density of colonisation by resistant microorganisms already present at low levels in commensal flora under antibiotic pressure. C Impairment of the normal flora and colonisation resistance associated with antibiotic pressure, leading to increased susceptibility to colonisation by new resistant microorganisms. D At the population level, the combined consequences of individual antibiotic treatments might lead to an increased reservoir of individuals who are colonised by resistant microorganisms that are likely to disseminate into the community. E Possible cross-transmission of resistant microorganisms emerged among the commensal flora of antibiotic users to unexposed people
However, if the impact of antimicrobial use on resistance is intuitively accepted, the general public, physicians and legislators require scientific rationales in order to understand the consequences of overprescription, change their practices and adopt suitable policies. This review provides an overview of the different study designs used to establish the relationships between antibiotic use and the emergence and spread of resistance; further, it highlights their main strengths and weaknesses.
Establishing causal inference in epidemiology
Establishing causal inferences [6] is part of the general process of scientific reasoning. In epidemiology, different models of causation are used to investigate risk factors associated with medical events [6–9]. Different sets of criteria have been proposed to assess causality, although none are infallible [10–13]. However, most epidemiologists define three main criteria of contributory causes: (i) the existence of an association between a cause and an effect at an individual level; (ii) the respect of temporal sequence (i.e. the cause precedes the effect); and (iii) the reversibility of the effect (i.e. altering the cause alters the probability of occurrence of the effect) [8]. Other criteria such as the strength and consistency of the association or dose–response relationship may also contribute to defining contributory causes (Table 1) [8, 11, 14].
The findings of epidemiological studies are of particular interest because they can lead to better understanding of diseases and create new strategies for prevention. In our field, many studies have been conducted in order to highlight the risk factors associated with the emergence of resistant microorganisms; their findings have prompted calls to reduce unnecessary antibiotic use, enhance surveillance systems, facilitate antimicrobial development and alert public opinion [15–22]. However, the 18th-century empiricist, David Hume [10], stated that certainty is impossible to obtain in empirical sciences; even the most carefully designed epidemiological study may be controversial or irreproducible [14]. Indeed, all studies potentially face problems demonstrating their internal or external validity (Table 2). Internal validity can be defined as the ability to avoid systematic errors (i.e. biases) and truly measure what was intended. All observational and some experimental studies present built-in biases such as selection, information and confounding biases that undermine the internal validity and quality of their results [23, 24]. In contrast, external validity is the extent to which the results of a study can provide a correct basis for a further generalisation (i.e. generalisability) [23, 24]. It is critical that clinical researchers, microbiologists and epidemiologists, studying the association between antibiotic exposure and the risk of the emergence of resistance, design robust studies that minimise internal biases and potential threats to the extrapolation of their findings.
Observational studies
Observational (i.e. non-experimental) studies describe the size and direction of a relationship among variables, including individual characteristics such as demographics or medical data, without implying any intervention from the investigator [25, 26]. They are frequently used because they are generally easier to implement than experimental studies [26–29]. However, unlike interventional studies, they are unable to demonstrate the reversibility of an effect and assess all criteria of a contributory cause (Table 1).
Cohort studies
Cohort studies follow up and compare different groups of subjects undergoing various exposures (e.g. antibiotic treatment vs. no treatment). However, unlike experimental studies, investigators select subjects to be observed and classify them according to the exposure status, rather than by assigning them to exposure groups [26]. In most cases, cohort studies prospectively follow volunteers until endpoints or the end of the study is reached. In our field, follow-up periods are not very long (a few weeks to a few months) because of the short duration of antibiotic courses, rapid emergence of resistance under antibiotic and limited length of stay of hospitalised patients [30–35]. Two other kinds of cohort also exist: retrospective cohorts, in which investigators identify subjects reaching the endpoint and where medical records are used to collect data about exposure [36–38], and ambidirectional cohorts, in which data collection goes in both directions [39, 40].
Due to their special design, cohort studies have appealing advantages. Since they collect information from exposition to outcome, they offer the possibility of analysing a clear temporal sequence between the putative cause and outcome, which is ideal for demonstrating causality (Table 1) and allowing the calculation of the incidence rate. In our field, prospective designs also allow the planning of serial surveillance sampling screening for colonisation with resistant microorganisms (as opposed to clinical sampling screening for infection) before, during and after antibiotic therapy. This is very useful for determining the acquisition of resistant microorganism in commensal flora [5] and has been used in several studies [30, 32, 33, 35, 41]. D’Agata et al. followed a cohort of patients undergoing haemodialysis through serial rectal swabbing from hospital admission until discharge and found that the acquisition of vancomycin-resistant enterococci is associated with vancomycin exposure [30]. Cohort studies can also help evaluate the risk of clinical infection once colonisation with resistant microorganisms has occurred [5]. Razazi et al. carried out a prospective study focusing on extended-spectrum beta-lactamase-producing Enterobacteriaceae acquisition and further infections associated with such bacteria among intensive care unit patients [42]. More generally, cohort studies are useful because they allow the calculation of true relative risks in contrast to case–control and cross-sectional studies, which only enable relative risk approximation. Finally, cohorts might also be useful for investigating multiple outcomes associated with a single exposure [8, 26, 43], such as the emergence of different resistant microorganisms under a unique antibiotic pressure [36].
However, like all observational studies, cohorts have limitations that threaten their internal validity (Table 2). First, selection bias can be an issue. Indeed, cohorts should theoretically compare groups of subjects similar in all respects except for the exposure and, therefore, the choice of the control group is critical. Internal comparison (e.g. controls chosen among patients from the same ward not receiving antibiotics) is always preferable for minimising the baseline differences between groups. However, the exposition criteria themselves might lead to substantial differences between groups. For example, patients receiving broad-spectrum antibiotics might not be comparable to patients receiving narrower-spectrum antibiotics or no antibiotics. They might have a more severe condition perhaps associated with an increased number of past hospitalisations that is potentially responsible for an increased load of multi-resistant organisms. Second, cohorts may also suffer from information bias, i.e. errors associated with the collection of the information used to measure the outcome (Table 2) [8, 23, 26, 44]. To limit such biases, outcomes should be defined clearly and information questionnaires standardised [23].
Another problem is confounding factors [8, 23, 26, 44]. Confounding factors are variables distributed differently between exposed and unexposed subjects that will affect the outcome but are not intermediate links in the chain of causation (Table 2) [8, 23, 26]. They can be random or due to selection bias and obscure the causal relationship examined by the study [8, 23, 26]. However, there are strategies to limit confounding factors. Individuals with known confounding factors can be excluded at inclusion, although this can potentially hinder the recruitment process and further generalisability of the study (Table 2). It is also possible to apply a correction for confounding factors during multi-variate analyses [8, 23, 26].
In contrast, loss to follow-up is a specific issue in cohort studies. It has two main consequences: (i) it can diminish the power of the study and (ii) it can introduce a bias, distorting results due to different bail-out rates in the exposed and unexposed groups [43]. The best way to avoid loss to follow-up is to pay attention during enrolment and include only participants who will probably complete the study. Conversely, such a strict attitude also has downsides; it can generate selection bias, hinder recruitment and impair the further generalisability of the results. However, in our field, loss to follow-up is not a substantial problem, as follow-up periods are usually short. Another major limitation associated with follow-ups in cohorts are the costs and difficulties of implementation, which often discourage researchers and explains why these observational designs are used less frequently than others (Table 3).
Case–control studies
Case–control studies are popular because of their appealing advantages. First, they require relatively less time, because the event of interest has already occurred when the study starts [26, 44]. Second, they are useful when studying rare conditions such as resistant microorganism infection [45]. Third, they allow the simultaneous investigation of multiple exposures associated with the outcome (e.g. multiple antibiotic exposures) [26, 44]. Their main features are to identify individuals who present with a medical event of interest (e.g. colonisation or infection with a resistant microorganism) from a well-defined source population and select controls representative of the source population who do not present with the event [8, 26, 44]. The control group will allow the evaluation of the exposure distribution within the source population and, subsequently, compare it to that observed in cases [26]. This will allow the calculation of odds ratios, which are a good estimate of relative risks when the incidence rate of the outcome is low in the population [46]. There are several papers in the literature that address the methodological issues of case–control studies on antibiotic risk factors associated with antibiotic-resistant organisms [45, 47–51].
The first issue is the choice of question to be addressed (i.e. the impact of antibiotic exposure on the acquisition of resistant microorganisms or on the risk of infection) and of the definition of the outcome [48]; most investigators use the results of clinical cultures to define their cases, whether they address the former [52–55] or the latter [56–59] question. If this makes sense when studying the post-antibiotic risk of infection, when studying acquisition, it may lead to the identification of distorted risk factors such as risk factors associated with the current infection, regardless of the presence or absence of resistant microorganisms [48]. Moreover, when using clinical samples to study community patients, there is a risk of using samples collected only because the first-line antibiotics failed [60], which might result in an overestimation of the association between resistance and prior exposure [60]. Hence, surveillance cultures assessing the colonisation status of patients are preferable for addressing the acquisition question [48].
Another challenge lies in the selection of the control group. Indeed, if the level of exposure in the controls is not representative of the actual baseline in the source population, selection bias will occur, threatening internal validity (Table 2) [23, 46]. To limit this phenomenon, investigators generally match cases and controls on the basis of criteria such as age, gender, hospital ward and, in our field, the time at risk for acquisition (i.e. the length of hospital stay) [49]. However, the matching process has drawbacks; it can hinder recruitment and, by definition, it is impossible to examine the effects of matched variables [23]. Investigators studying the acquisition question must face another challenge associated with the choice of controls [47–49, 51]. If the study aims to determine the risk factors for acquiring a specific resistant microorganism, controls should be chosen from among patients with negative cultures for the causative microorganisms [49]. However, in their review of 37 case–control studies, Harris et al. state that investigators most frequently select controls from among patients with positive cultures for susceptible microorganisms [47]. Consequently, they might improperly identify antibiotics as risk factors for acquiring resistant microorganisms. Indeed, antibiotics have intrinsic activities against susceptible organisms, and controls defined as carriers of susceptible organisms are less likely to have been exposed to antibiotics than the source population or cases [47]. In contrast, if the study aims to establish risk factors for developing resistant strains in individuals already carrying susceptible strains, controls should be chosen from among subjects with positive cultures for the susceptible microorganism [49].
More generally, case–control studies might present other issues related to internal validity (Table 2) [8, 23, 26]. First, information biases can occur; they involve recall and reporting biases, which arise when subjects from one group are more likely to recall or report events than others, as well as classification or measurement biases, which result from dissymmetric information collection according to a subject’s status as a case or control [8, 23, 26]. All of these biases may impair the quality of risk factor measurement and distort associations between exposure and outcome. To reduce these biases, information about expositions should be gathered by interviewers blinded of the subjects’ case or control status using standardised questionnaires [8, 23, 26]. Second, investigators must deal with the recurrent issue of confounding factors [8, 23, 26]. As described above, different strategies exist to minimise confounding factors, including excluding individuals with known confounding factors, matching processes and mathematical correction [8, 23, 26] (Table 3).
Cross-sectional studies
Cross-sectional or prevalence studies include all people or a representative sample from a population, regardless of exposure or outcome [26]. They are performed to examine the presence or absence of a medical event such as carriage or infection with a resistant microorganism and exposure to an antibiotic at a particular time [26, 27]. Similar to case–control studies, they are frequently used because they require relatively little time and are easy to implement [8, 26, 60–63].
However, cross-sectional studies have critical limitations. Since both exposure and outcome are ascertained simultaneously, the temporal sequence cannot be clearly established (Table 1) [27]. For example, if colonisation with resistant microorganisms is more frequent among subjects exposed to antibiotics, does it mean that prior antibiotic exposure leads to extra colonisation or that subjects with higher colonisation consume more antibiotics because they are more prone to infections? Another problem, called length-biased sampling, is the over-representation of cases with chronic conditions [27]. For example, subjects with a transitory excess of resistant microorganisms following antibiotic exposure are less likely to be identified as cases than subjects carrying long-term resistant microorganisms due to an underlying medical condition. Finally, cross-sectional studies are susceptible to other internal validity threats such as information biases due to their retrospective nature and confounding factors (Table 2) [8, 23, 26]. Therefore, they might not be the optimal study design for achieving aetiologic objectives (Table 3).
Interventional studies
A common attribute of interventional studies is the control of one or more variables, manipulated by the investigator, to observe their effect on dependant variables [25, 64]. Interventional studies offer the possibility to test the reversibility of an effect (Table 1). Moreover, the assignment of exposure by the investigator is a way to limit confounding factors and enhance internal validity (Table 2) [26].
Randomised controlled trials
Randomised experiments are considered to be the gold standard of causal research in medical sciences and are at the top of the hierarchy of study types in the evidence-based literature [25, 65–67]. They are prospective studies in which volunteers are randomly assigned healthcare interventions. If designed well, these studies are able to demonstrate all three criteria of a contributory cause (Table 1). This is why they gained increasing recognition during the 20th century and became the best approach for assessing healthcare interventions. However, few randomised trials have been designed to investigate the association between antibiotic exposure and the emergence or spread of resistant microorganisms [68–74]. In contrast, several trials have been designed to evaluate the efficacy of antibiotics, while some analyse resistance as a secondary outcome [75, 76].
Randomisation is the key principle in randomised controlled trials. The random assignment of treatments to the participants, which is controlled by the investigators, allows the creation of probabilistically similar groups. Hence, any differences observed between groups are probably due to differences in the treatments [25]. In other words, proper randomisation reduces the selection and confounding biases (Table 2) that hinder all other epidemiological studies [23, 77]. However, it is important to stress that randomisation is associated with critical implementation issues [77, 78]. There are many methods for generating unpredictable randomised allocation sequences—some as simple as tossing a coin or using a random number table. However, their benefits might be undermined if the allocation sequence is not kept concealed [24, 77, 78]. Knowledge of the next assignment could cause selection biases to seep back into trials; investigators could exclude patients perceived to be part of an inappropriate group [24, 78]. Schulz et al. demonstrates that trials using inadequate allocation concealment strategies yield larger estimates of treatment effects and produce more heterogeneous results [79]. The generation and concealment of unpredictable randomised allocation sequences are the keys to ensuring the unbiased nature of randomised trials.
However, randomised trials are sometimes susceptible to other systematic errors. First, detection biases can occur when the investigators assessing the outcome know the treatment that has been allocated to the participants. Blinding strategies, in which the nature of the treatment is masked to the participants and/or investigators, can be used to prevent this [80, 81]. In our field, microbiologists analysing samples for resistance should be blinded to the treatment of the participants [71]. Another possible difficulty, similar to cohort studies, is the loss to follow-up [43, 81]. However, in our field, this problem is generally minor, because follow-ups do not last very long (1–2 months in the above-mentioned studies) [68–74]. Finally, although randomised trials may be the best option for ensuring high internal validity, they can suffer from a lack of external validity (Table 2). Indeed, inclusion and exclusion criteria are sometimes unduly rigorous, leading to the exclusion of particular at-risk groups [27]. In addition, patients willing to participate tend to differ from those who choose not to participate [27]. Both factors might limit the generalisability of the findings of such studies [27] (Table 3).
Quasi-experimental studies
Quasi-experimental studies aim to demonstrate causality between an intervention and outcome without using randomisation [25, 82, 83]. Even if their credibility for assessing causality is lower than that of randomised trials, they are frequently used when it is not logistically feasible or ethical to conduct randomised trials [25, 82, 83]. In our field, they are invaluable for evaluating the impact of antibiotic prescription control policies with respect to resistant microorganisms and assessing the performance of interventions implemented to limit outbreaks of resistant microorganisms. There are various papers in the literature that address their methodological issues in the fields of infection control and antibiotic resistance [82–86]. As described by Harris et al. in 2004 and 2005 [82, 83], there are many existing designs for quasi-experimental studies that can be clustered into three groups: (i) designs that do not use control groups, the most frequent being the one-group pre-test–post-test (before-and-after) design, in which investigators make measurements in a unit/hospital before the intervention and another afterwards [87–94]; (ii) designs that use control groups but no pre-test, in which investigators apply an intervention in a unit/hospital and compare the outcome to an intervention-free unit/hospital [95]; and (iii) designs that use control groups and pre-test, most often using one group with an intervention and another intervention-free group, with measurements before and after the intervention [96]. Harris et al. propose a hierarchy of these designs with respect to their internal validity quality: group (iii) is better than group (ii), which is better than group (i) [82]. However, they report that higher-quality designs are not used most frequently probably because they are more difficult to implement [83]. This is corroborated by de Bruin and Riley, who analysed 12 quasi-experimental studies on the effect of vancomycin-prescribing interventions on vancomycin-resistant enterococci and found all of them to be simple pre-test–post-test designs [84].
Even though quasi-experimental studies meet the three major criteria of contributory causes (Table 1), they present limitations arising from non-randomisation, leading to difficulties in controlling for confounding factors [82, 83]. The best way to minimise threats to their internal validity is to use higher-quality designs that include control groups, which may help identify confounding factors, and pre-test measurements, which allow the assessment of the initial comparability of groups and highlight potential selection bias [82, 83, 85].
Another limitation of quasi-experimental studies is ‘maturation effects’ [82]. Indeed, measurements before and after an intervention may be separated by several months, and observed variations might simply be the result of seasonal cycles. To limit this problem, investigators can choose a higher-quality study design, in which the intervention is first administered to the intervention group and then to the control group. This helps demonstrate the reproducibility of the results in the two groups at two different times (Table 3).
Population-level and multi-level studies
Previous designs gathered individual-level data and studied the direct effects of antibiotics on resistance. In contrast, population-level studies are a common way to describe the indirect effects of antibiotics on resistance (Fig. 1) [5]. These designs are very useful for establishing links between changes in the levels of antibiotic prescription (e.g. reduced antibiotic use following local or national recommendations) and antibiotic resistance [97]. Among population-level studies, investigators can choose between observational or cluster-randomised interventional studies.
In population-level observational studies, aggregated data regarding antibiotics are obtained either out of reimbursement data or through sales or distribution data [97–100]. Unfortunately, both strategies present limitations: using reimbursement data is associated with a risk of under-detection bias due to unaccounted over-the-counter sales, parallel trade or non-reimbursed antibiotics, while using sales/distribution data is associated with risks of under- or over-detection bias due to parallel import or export [100]. Therefore, population-level studies sometimes lack sufficient data regarding antibiotic exposure to avoid confounding factors [101], and studies that estimate both individual- and population-level antimicrobial use (i.e. multi-level studies) are preferable [5, 99, 102, 103]. For instance, Harbarth et al. demonstrate this in a study reporting a significant association between antibiotic exposure and resistance at the individual level but not at the group level [102]. Similarly, Donnan et al. studied the association between trimethoprim resistance in urinary bacteria and antibiotic exposure and found no association at the practice level, whereas individual exposure to antibiotics was significantly associated with trimethoprim resistance in the multi-level model [99].
The main feature of cluster-randomised trials is the same as that of a randomised trial, except that investigators control the intervention by assigning it randomly to groups of patients rather than individuals [104–106]. Cluster-randomised trials are a key tool for evaluating interventions at the group level, especially in health services [104–106]. They can be implemented when it is impractical or unethical to randomise individuals. However, they also present noteworthy drawbacks. First, many more subjects are required to obtain the same level of precision [44]. Second, it is considerably more complex to analyse the data produced because they are no longer independent and basic statistical procedures generally assume such a characteristic [44]. Therefore, cluster-randomised trials remain rare in our field. We identified less than ten studies using the search terms ‘cluster randomised trial’, ‘anti-bacterial agents’ and ‘resistance’ in the MEDLINE database [107–110]. The work of Skalet et al. focusing on trachoma control in Ethiopia and re-analysed to discuss Streptococcus pneumoniae resistance [109] is an interesting example; 24 communities were randomised to receive either azithromycin mass treatment during the first year of life or no antibiotics. This work demonstrates that frequent azithromycin use selected for macrolide resistance among nasopharyngeal S. pneumoniae at the community level. The work of de Smet et al. also provides an example [107, 108]. Patients with mechanical ventilation in 13 intensive care units in the Netherlands were randomised and received standard care, oropharyngeal decontamination with topical antibiotics or digestive decontamination with topical antibiotics plus intravenous cefotaxime. The results show that the acquisition of respiratory tract colonisation with highly resistant pathogens is lowest with the digestive decontamination procedure [108] (Table 3).
Systematic reviews and meta-analysis
Until the mid-1990s, the system for ranking the levels of evidence in clinical research attributed the highest grade to ‘at least one properly randomised controlled trial’ [111, 112]. However, this paradigm has been challenged by different studies showing that well-conducted observational studies can produce results similar to those of randomised trials [67, 113, 114]. Meanwhile, the results of randomised trials can exhibit significant discrepancies possibly because they are less likely to include a broad representation of the population [67, 115]. These findings led to the conclusion that a single randomised trial cannot provide gold-standard results on a topic of interest and that evidence from different studies should be analysed together [65, 67].
Thus, researchers perform systematic reviews associated with a meta-analysis (a combined analysis of the data reviewed). This approach aims to identify, synthesise and, if possible, quantitatively combine the results of relevant studies. Meta-analyses increase statistical power and allow the calculation of more precise estimations of the effects of risk factors. It is of great interest to generalise the results of single studies, reconcile inconsistent results, assess weak risk factors with large impacts on public health (as in our field) and investigate the risks associated with rare diseases [116]. Systematic reviews and meta-analyses have been increasingly used over the past decade, primarily for randomised controlled trials and observational studies to a lesser extent [67, 117–120]. However, few focus on the relationship between antibiotic exposure and resistance. We found less than ten studies in the MEDLINE database using the search terms ‘meta-analysis’, ‘anti-bacterial agents’ and ‘resistance’ [60, 84, 121–124].
However, the strength of meta-analyses may also be their weakness, and two major difficulties arise from combining and generalising the results of different studies. The first problem is publication bias: studies with negative results are less likely to be published than others. This limitation could lead the meta-analysis to overestimate the relationship between an exposure and outcome [116, 117, 125]. Second, not all included studies might have the same degree of quality and they might possess various biases. Hence, combining their results could lead to the combination of non-comparable results [117]. This limitation is particularly important when combining the data of observational studies, which are more likely to be biased. The best way to minimise this issue is to thoroughly develop and conduct the research protocol. First, the most accurate research question should be defined using common sense, clinical insight and biological plausibility. This will aid the selection of precise inclusion and exclusion criteria to select relevant studies [125, 126]. After the selection process using pre-determined search strategies in electronic databases such as MEDLINE, the validity and comparability of included studies must be evaluated through statistical tests assessing the magnitude of inter-study heterogeneity [116, 127–129]. This point is crucial because it will determine whether a pooled estimate can be calculated or not. If the heterogeneity is high, no overall estimate should be reported. However, this problem can be partly avoided if the reviewers have access to the individual data from each study instead of the overall data. In this case, all data will be re-analysed using the new statistical model, thus, presenting the results in a unified way. Unfortunately, this type of meta-analysis is very rare because it is more expensive and very time consuming (Table 3).
Mathematical modelling
Mathematical modelling is another tool for analysing the associations between antibiotic exposure and the emergence and spread of resistance at the individual or population level [5]. Modelling implies the use of a theoretical framework and aims to explore scenarios under varying conditions [130, 131]. Two kinds of models are found in the literature. The oldest ones are deterministic models using ordinary differential equations [130, 131]. They are applied when the dynamics of the study population can be described according to the average behaviour of individuals [130, 131]. Individuals are aggregated into homogeneous compartments (e.g. colonised/non-colonised or infected/non-infected), the parameters of the model are fixed and chance events are not taken into account. Unfortunately, these models are not well suited for small populations such as hospital wards, in which fluctuations of colonisation or infection with resistant organisms might happen by chance [130, 131]. To take into account the random variability of the outcome, modellers use stochastic models. In stochastic models, events do not occur at a fixed rate but with a probability inferred by the parameter value [130, 131]. These models, also called ‘individual-based models’, are able to take individual heterogeneity into consideration [132]. To evaluate the average behaviour in these models, modellers run many simulations and determine the mean and variance of the results [130–132].
In our field, models have demonstrated their value on several occasions. They can help generate or test hypotheses about the relationships between antibiotic use and resistance patterns [5]. For example, they can describe the impact of different treatment protocols on resistance patterns [133]. D’Agata et al. found that, among several factors possibly contributing to the emergence of resistant bacteria, delayed initiation of the antibiotic is probably the most important [134]. Models can also generate hypotheses about the most important factors to control or help test the efficacy of intervention programmes. Bonhoeffer et al. and Bergstrom et al. demonstrate that mixing strategies (i.e. the simultaneous use of different antibiotics at the population level) perform as good as or better than cycling policies to prevent the spread of resistance, while the best option to combat overall resistance is treating individuals with a combination of drugs [135, 136]. Kouyos et al. proposed and tested another strategy based on the regular switching of antibiotics in hospital wards according to the cumulative results of susceptibility testing performed on bacteria isolated from the same ward [137].
However, the strength of modelling, which allows the simulation of different situations to explore relationships between inter-dependent variables, is also its weakness. All models involve the simplification of reality and, therefore, cannot truly address the level of complexity that influences the acquisition of an antibiotic-resistant microorganism. The findings of mathematical models should always be subsequently tested in empirical studies (Table 3).
Conclusion
Choosing an appropriate study design to investigate the relationship between antibiotic exposure and its effects on resistance is critical for researchers. Up to now, many case–control and cross-sectional studies have been published. Although they provide a general understanding of the subject, they present limitations that might impair their ability to provide further insight. Prospective cohort studies and randomised trials would help us gain a more precise understanding of the individual effects of antibiotic exposure. Moreover, multi-level studies and cluster-randomised trials might be useful for investigating the indirect effects of exposure at the community level.
References
Omran AR (2001) The epidemiologic transition. A theory of the Epidemiology of population change. 1971. Bull World Health Organ 79:161–170
Armelagos GJ, Brown PJ, Turner B (2005) Evolutionary, historical and political economic perspectives on health and disease. Soc Sci Med 61:755–765. doi:10.1016/j.socscimed.2004.08.066
Harper K, Armelagos G (2010) The changing disease-scape in the third epidemiological transition. Int J Environ Res Public Health 7:675–697. doi:10.3390/ijerph7020675
Bax R, Mullan N, Verhoef J (2000) The millennium bugs—the need for and development of new antibacterials. Int J Antimicrob Agents 16:51–59. doi:10.1016/S0924-8579(00)00189-8
Lipsitch M, Samore MH (2002) Antimicrobial use and antimicrobial resistance: a population perspective. Emerg Infect Dis 8:347–354
Susser M (2001) Glossary: causality in public health science. J Epidemiol Community Health 55(6):376–378. doi:10.1136/jech.55.6.376
Rothman KJ, Greenland S, Poole C, Lash TL (2008) Causation and causal inference. In: Rothman KJ, Greenland S, Lash TL (eds) Modern epidemiology. Lippincott Williams & Wilkins, Philadelphia, p 5–31
Riegelman RK (2005) Studying a study and testing a test: how to read the medical evidence, 5th edn. Lippincott Williams & Wilkins, Philadelphia
Olsen J (2003) What characterises a useful concept of causation in epidemiology? J Epidemiol Community Health 57(2):86–88. doi:10.1136/jech.57.2.86
Hume D (1739) Part III. Of Knowledge and Probability. In: A Treatise of Human Nature. Book 1. Of the Understanding
Hill AB (1965) The environment and disease: association or causation? Proc R Soc Med 58:295–300
Susser M (1991) What is a cause and how do we know one? A grammar for pragmatic epidemiology. Am J Epidemiol 133(7):635–648
(1964) Smoking and Health: Report of the Advisory Committee to the Surgeon General of the Public Health Service. Washington, DC: US Department of Health, Education, and Welfare: Public Health Service Publication
Rothman KJ, Greenland S (2005) Causation and causal inference in epidemiology. Am J Public Health 95:S144–S150. doi:10.2105/AJPH.2004.059204
Infectious Diseases Society of America (IDSA), Spellberg B, Blaser M, Guidos RJ, Boucher HW, Bradley JS et al (2011) Combating antimicrobial resistance: policy recommendations to save lives. Clin Infect Dis 52(Suppl 5):S397–S428. doi:10.1093/cid/cir153
Carlet J, Collignon P, Goldmann D, Goossens H, Gyssens IC, Harbarth S et al (2011) Society’s failure to protect a precious resource: antibiotics. Lancet 378(23):369–371. doi:10.1016/S0140-6736(11)60401-7
Carlet J, Jarlier V, Harbarth S, Voss A, Goossens H, Pittet D et al (2012) Ready for a world without antibiotics? The Pensières Antibiotic Resistance Call to Action. Antimicrob Resist Infect Control 1(1):11. doi:10.1186/2047-2994-1-11
Centers for Disease Control and Prevention (CDC). Get Smart: Know When Antibiotics Work. Home page at: http://www.cdc.gov/getsmart/
Alvan G, Edlund C, Heddini A (2011) The global need for effective antibiotics—a summary of plenary presentations. Drug Resist Updat 14:70–76. doi:10.1016/j.drup.2011.01.007
European Medicines Agency (EMA). The bacterial challenge—time to react a call to narrow the gap between multidrug-resistant bacteria in the EU and development of new antibacterial agents. Available online at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2009/11/news_detail_000044.sjsp&jsenabled=true
European Antimicrobial Resistance Surveillance Network (EARS-Net). Home page at: http://www.ecdc.europa.eu/en/activities/surveillance/EARS-Net/Pages/index.aspx
European Surveillance of Antimicrobial Consumption (ESAC). Home page at: http://app.esac.ua.ac.be/public/
Grimes DA, Schulz KF (2002) Bias and causal associations in observational research. Lancet 359(19):248–252. doi:10.1016/S0140-6736(02)07451-2
Jüni P, Altman DG, Egger M (2001) Systematic reviews in health care: assessing the quality of controlled clinical trials. BMJ 323(7303):42–46. doi:10.1136/bmj.323.7303.42
Shadish WR, Cook TD, Campbell DT (2002) Experimental and quasi-experimental designs for generalized causal inference. Houghton Mifflin, Boston
Rothman KJ, Greenland S, Lash TL (2008) Modern epidemiology, 3rd edn. Lippincott Williams & Wilkins, Philadelphia
Grimes DA, Schulz KF (2002) An overview of clinical research: the lay of the land. Lancet 359(9300):57–61. doi:10.1016/S0140-6736(02)07283-5
Funai EF, Rosenbush EJ, Lee MJ, Del Priore G (2001) Distribution of study designs in four major US journals of obstetrics and gynecology. Gynecol Obstet Invest 51:8–11
Scales CD Jr, Norris RD, Peterson BL, Preminger GM, Dahm P (2005) Clinical research and statistical methods in the urology literature. J Urol 174:1374–1379
D’Agata EMC, Green WK, Schulman G, Li H, Tang Y-W, Schaffner W (2001) Vancomycin-resistant enterococci among chronic hemodialysis patients: a prospective study of acquisition. Clin Infect Dis 32(1):23–29. doi:10.1086/317549
Feikin DR, Dowell SF, Nwanyanwu OC, Klugman KP, Kazembe PN, Barat LM et al (2000) Increased carriage of trimethoprim/sulfamethoxazole-resistant Streptococcus pneumoniae in Malawian children after treatment for malaria with sulfadoxine/pyrimethamine. J Infect Dis 181(4):1501–1505. doi:10.1086/315382
Woerther P-L, Angebault C, Jacquier H, Hugede H-C, Janssens A-C, Sayadi S et al (2011) Massive increase, spread, and exchange of extended spectrum β-lactamase-encoding genes among intestinal Enterobacteriaceae in hospitalized children with severe acute malnutrition in Niger. Clin Infect Dis 53:677–685. doi:10.1093/cid/cir522
Ong DSY, Jongerden IP, Buiting AG, Leverstein-van Hall MA, Speelberg B, Kesecioglu J et al (2011) Antibiotic exposure and resistance development in Pseudomonas aeruginosa and Enterobacter species in intensive care units. Crit Care Med 39:2458–2463. doi:10.1097/CCM.0b013e318225756d
Donskey CJ, Chowdhry TK, Hecker MT, Hoyen CK, Hanrahan JA, Hujer AM et al (2000) Effect of antibiotic therapy on the density of vancomycin-resistant enterococci in the stool of colonized patients. N Engl J Med 343(26):1925–1932. doi:10.1056/NEJM200012283432604
Lepelletier D, Cady A, Caroff N, Marraillac J, Reynaud A, Lucet J-C et al (2010) Imipenem-resistant Pseudomonas aeruginosa gastrointestinal carriage among hospitalized patients: risk factors and resistance mechanisms. Diagn Microbiol Infect Dis 66:1–6. doi:10.1016/j.diagmicrobio.2009.08.014
Eveillard M, Schmit JL, Eb F (2002) Antimicrobial Use prior to the acquisition of multiresistant bacteria. Infect Control Hosp Epidemiol 23(3):155–158
Grüneberg RN, Shaw EJ (1976) The influence of antibiotic treatment on resistance patterns of coliform bacilli in childhood urinary-tract infection. J Med Microbiol 9(2):233–237. doi:10.1099/00222615-9-2-233
Kaye KS, Cosgrove S, Harris A, Eliopoulos GM, Carmeli Y (2001) Risk factors for emergence of resistance to broad-spectrum cephalosporins among Enterobacter spp. Antimicrob Agents Chemother 45:2628–2630. doi:10.1128/AAC.45.9.2628-2630.2001
Chung A, Perera R, Brueggemann AB, Elamin AE, Harnden A, Mayon-White R et al (2007) Effect of antibiotic prescribing on antibiotic resistance in individual children in primary care: prospective cohort study. BMJ 335(7617):429. doi:10.1136/bmj.39274.647465.BE
Lepelletier D, Caroff N, Riochet D, Bizouarn P, Bourdeau A, Le Gallou F et al (2006) Risk-factors for gastrointestinal colonisation with resistant Enterobacteriaceae among hospitalised patients: a prospective study. Clin Microbiol Infect 12(10):974–979. doi:10.1111/j.1469-0691.2006.01474.x
Rodríguez-Baño J, Alcalá JC, Cisneros JM, Grill F, Oliver A, Horcajada JP et al (2008) Community infections caused by extended-spectrum β-lactamase-producing Escherichia coli. Arch Intern Med 168(17):1897–1902. doi:10.1001/archinte.168.17.1897
Razazi K, Derde LP, Verachten M, Legrand P, Lesprit P, Brun-Buisson C (2012) Clinical impact and risk factors for colonization with extended-spectrum β-lactamase-producing bacteria in the intensive care unit. Intensive Care Med 38(11):1769–1778. doi:10.1007/s00134-012-2675-0
Grimes DA, Schulz KF (2002) Cohort studies: marching towards outcomes. Lancet 359(9303):341–345. doi:10.1016/S0140-6736(02)07500-1
Woodward M (2004) Epidemiology: study design and data analysis, 2nd edn. Taylor & Francis, Boca Raton
Kaye KS, Harris AD, Samore M, Carmeli Y (2005) The case–case–control study design: addressing the limitations of risk factor studies for antimicrobial resistance. Infect Control Hosp Epidemiol 26(4):346–351
Schulz KF, Grimes DA (2002) Case–control studies: research in reverse. Lancet 359(2):431–434. doi:10.1016/S0140-6736(02)07605-5
Harris AD, Karchmer TB, Carmeli Y, Samore MH (2001) Methodological principles of case–control studies that analyzed risk factors for antibiotic resistance: a systematic review. Clin Infect Dis 32(4):1055–1061. doi:10.1086/319600
D’Agata EMC (2005) Methodologic issues of case–control studies: a review of established and newly recognized limitations. Infect Control Hosp Epidemiol 26:338–341. doi:10.1086/502548
Harris AD, Samore MH, Lipsitch M, Kaye KS, Perencevich E, Carmeli Y (2002) Control-group selection importance in studies of antimicrobial resistance: examples applied to Pseudomonas aeruginosa, Enterococci, and Escherichia coli. Clin Infect Dis 34(12):1558–1563. doi:10.1086/340533
D’Agata EMC, Cataldo MA, Cauda R, Tacconelli E (2006) The importance of addressing multidrug resistance and not assuming single-drug resistance in case–control studies. Infect Control Hosp Epidemiol 27:670–674. doi:10.1086/505917
Harris AD, Carmeli Y, Samore MH, Kaye KS, Perencevich E (2005) Impact of severity of illness bias and control group misclassification bias in case–control studies of antimicrobial-resistant organisms. Infect Control Hosp Epidemiol 26(4):342–345
Beekmann SE, Diekema DJ, Heilmann KP, Richter SS, Doern GV (2006) Macrolide use identified as risk factor for macrolide-resistant Streptococcus pneumoniae in a 17-center case–control study. Eur J Clin Microbiol Infect Dis 25:335–339. doi:10.1007/s10096-006-0137-8
Troillet N, Samore MH, Carmeli Y (1997) Imipenem-resistant Pseudomonas aeruginosa: risk factors and antibiotic susceptibility patterns. Clin Infect Dis 25(5):1094–1098. doi:10.1086/516092
Seaton RA, Steinke DT, Phillips G, MacDonald T, Davey PG (2000) Community antibiotic therapy, hospitalization and subsequent respiratory tract isolation of Haemophilus influenzae resistant to amoxycillin: a nested case–control study. J Antimicrob Chemother 46:307–309
Loeb MB, Craven S, McGeer AJ, Simor AE, Bradley SF, Low DE et al (2003) Risk factors for resistance to antimicrobial agents among nursing home residents. Am J Epidemiol 157(1):40–47. doi:10.1093/aje/kwf173
Hillier S, Roberts Z, Dunstan F, Butler C, Howard A, Palmer S (2007) Prior antibiotics and risk of antibiotic-resistant community-acquired urinary tract infection: a case–control study. J Antimicrob Chemother 60:92–99. doi:10.1093/jac/dkm141
Steinke DT, Seaton RA, Phillips G, MacDonald TM, Davey PG (2001) Prior trimethoprim use and trimethoprim-resistant urinary tract infection: a nested case–control study with multivariate analysis for other risk factors. J Antimicrob Chemother 47:781–787
Colodner R, Nuri Y, Chazan B, Raz R (2008) Community-acquired and hospital-acquired candiduria: comparison of prevalence and clinical characteristics. Eur J Clin Microbiol Infect Dis 27:301–305. doi:10.1007/s10096-007-0438-6
Bhavnani SM, Drake JA, Forrest A, Deinhart JA, Jones RN, Biedenbach DJ et al (2000) A nationwide, multicenter, case–control study comparing risk factors, treatment, and outcome for vancomycin-resistant and -susceptible enterococcal bacteremia. Diagn Microbiol Infect Dis 36:145–158. doi:10.1016/S0732-8893(99)00136-4
Costelloe C, Lovering A, Montgomery A, Lewis D, McNulty C, Hay AD (2012) Effect of antibiotic prescribing in primary care on meticillin-resistant Staphylococcus aureus carriage in community-resident adults: a controlled observational study. Int J Antimicrob Agents 39:135–141. doi:10.1016/j.ijantimicag.2011.09.022
Arason VA, Sigurdsson JA, Erlendsdottir H, Gudmundsson S, Kristinsson KG (2006) The role of antimicrobial Use in the epidemiology of resistant pneumococci: a 10-year follow up. Microb Drug Resist 12:169–176. doi:10.1089/mdr.2006.12.169
Lo W-T, Lin W-J, Tseng M-H, Lu J-J, Lee S-Y, Chu M-L et al (2007) Nasal carriage of a single clone of community-acquired methicillin-resistant Staphylococcus aureus among kindergarten attendees in northern Taiwan. BMC Infect Dis 7:51. doi:10.1186/1471-2334-7-51
Woerther P-L, Angebault C, Lescat M, Ruppé E, Skurnik D, Mniai AE et al (2010) Emergence and dissemination of extended-spectrum beta-lactamase-producing Escherichia coli in the community: lessons from the study of a remote and controlled population. J Infect Dis 202(4):515–523. doi:10.1086/654883
Cook TD, Campbell DT (1986) The causal assumptions of quasi-experimental practice. Synthese 68:141–180. doi:10.1007/BF00413970
Harbour R, Miller J (2001) A new system for grading recommendations in evidence based guidelines. BMJ 323(11):334–336. doi:10.1136/bmj.323.7308.334
Guyatt GH, Haynes RB, Jaeschke RZ, Cook DJ, Green L, Naylor CD et al (2000) Users’ guides to the medical literature. XXV. Evidence-based medicine: principles for applying the users’ guides to patient care. JAMA 284(10):1290–1296. doi:10.1001/jama.284.10.1290
Concato J, Shah N, Horwitz RI (2000) Randomized, controlled trials, observational studies, and the hierarchy of research designs. N Engl J Med 342(25):1887–1892. doi:10.1056/NEJM200006223422507
Ghaffar F, Friedland IR, Katz K, Muniz LS, Smith JL, Davis P et al (1999) Increased carriage of resistant non-pneumococcal alpha-hemolytic streptococci after antibiotic therapy. J Pediatr 135:618–623
Malhotra-Kumar S, Lammens C, Coenen S, Van Herck K, Goossens H (2007) Effect of azithromycin and clarithromycin therapy on pharyngeal carriage of macrolide-resistant streptococci in healthy volunteers: a randomised, double-blind, placebo-controlled study. Lancet 369(9560):482–490. doi:10.1016/S0140-6736(07)60235-9
Nord CE, Peterson J, Ambruzs M, Fisher AC (2009) Levofloxacin versus azithromycin on the oropharyngeal carriage and selection of antibacterial-resistant streptococci in the microflora of healthy adults. Curr Med Res Opin 25:1461–1467. doi:10.1185/03007990902953468
Schrag SJ, Peña C, Fernández J, Sánchez J, Gómez V, Pérez E et al (2001) Effect of short-course, high-dose amoxicillin therapy on resistant pneumococcal carriage: a randomized trial. JAMA 286(1):49–56. doi:10.1001/jama.286.1.49
Toltzis P, Dul M, O’Riordan MA, Toltzis H, Blumer JL (2007) Comparative effects of single-dose ceftriaxone versus three oral antibiotic regimens on stool colonization by resistant bacilli in children. Pediatr Infect Dis J 26:25–30. doi:10.1097/01.inf.0000247130.11902.64
Berg HF, Tjhie JHT, Scheffer G-J, Peeters MF, van Keulen PHJ, Kluytmans JAJW et al (2004) Emergence and persistence of macrolide resistance in oropharyngeal flora and elimination of nasal carriage of Staphylococcus aureus after therapy with slow-release clarithromycin: a randomized, double-blind, placebo-controlled study. Antimicrob Agents Chemother 48:4183–4188. doi:10.1128/AAC.48.11.4183-4188.2004
Kastner U, Guggenbichler JP (2001) Influence of macrolide antibiotics on promotion of resistance in the oral flora of children. Infection 29:251–256. doi:10.1007/s15010-001-1072-3
Chang S-C, Hsieh S-M, Chen M-L, Sheng W-H, Chen Y-C (2000) Oral fusidic acid fails to eradicate methicillin-resistant Staphylococcus aureus colonization and results in emergence of fusidic acid-resistant strains. Diagn Microbiol Infect Dis 36:131–136. doi:10.1016/S0732-8893(99)00116-9
Gribble MJ, Chow AW, Naiman SC, Smith JA, Bowie WR, Sacks SL et al (1983) Prospective randomized trial of piperacillin monotherapy versus carboxypenicillin–aminoglycoside combination regimens in the empirical treatment of serious bacterial infections. Antimicrob Agents Chemother 24(3):388–393. doi:10.1128/AAC.24.3.388
Schulz KF, Grimes DA (2002) Generation of allocation sequences in randomised trials: chance, not choice. Lancet 359(9305):515–519. doi:10.1016/S0140-6736(02)07683-3
Schulz KF, Grimes DA (2002) Allocation concealment in randomised trials: defending against deciphering. Lancet 359(16):614–618. doi:10.1016/S0140-6736(02)07750-4
Schulz KF, Chalmers I, Hayes RJ, Altman DG (1995) Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 273(5):408–412
Schulz KF, Grimes DA (2002) Blinding in randomised trials: hiding who got what. Lancet 359(9307):696–700. doi:10.1016/S0140-6736(02)07816-9
Schulz KF (1996) Randomised trials, human nature, and reporting guidelines. Lancet 348(9027):596–598. doi:10.1016/S0140-6736(96)01201-9
Harris AD, Bradham DD, Baumgarten M, Zuckerman IH, Fink JC, Perencevich EN (2004) The use and interpretation of quasi-experimental studies in infectious diseases. Clin Infect Dis 38(11):1586–1591. doi:10.1086/420936
Harris AD, Lautenbach E, Perencevich E (2005) A systematic review of quasi-experimental study designs in the fields of infection control and antibiotic resistance. Clin Infect Dis 41(7):77–82. doi:10.1086/430713
de Bruin MA, Riley LW (2007) Does vancomycin prescribing intervention affect vancomycin-resistant enterococcus infection and colonization in hospitals? A systematic review. BMC Infect Dis 7:24. doi:10.1186/1471-2334-7-24
Shardell M, Harris AD, El-Kamary SS, Furuno JP, Miller RR, Perencevich EN (2007) Statistical analysis and application of quasi experiments to antimicrobial resistance intervention studies. Clin Infect Dis 45(7):901–907. doi:10.1086/521255
Harbarth S, Samore MH (2008) Interventions to control MRSA: high time for time-series analysis? J Antimicrob Chemother 62(3):431–433. doi:10.1093/jac/dkn240
Sundqvist M, Geli P, Andersson DI, Sjölund-Karlsson M, Runehagen A, Cars H et al (2010) Little evidence for reversibility of trimethoprim resistance after a drastic reduction in trimethoprim use. J Antimicrob Chemother 65:350–360. doi:10.1093/jac/dkp387
Lafaurie M, Porcher R, Donay J-L, Touratier S, Molina J-M (2012) Reduction of fluoroquinolone use is associated with a decrease in methicillin-resistant Staphylococcus aureus and fluoroquinolone-resistant Pseudomonas aeruginosa isolation rates: a 10 year study. J Antimicrob Chemother 67:1010–1015. doi:10.1093/jac/dkr555
Gottesman BS, Carmeli Y, Shitrit P, Chowers M (2009) Impact of quinolone restriction on resistance patterns of Escherichia coli isolated from urine by culture in a community setting. Clin Infect Dis 49(6):869–875. doi:10.1086/605530
Madaras-Kelly KJ, Remington RE, Lewis PG, Stevens DL (2006) Evaluation of an intervention designed to decrease the rate of nosocomial methicillin-resistant Staphylococcus aureus infection by encouraging decreased fluoroquinolone use. Infect Control Hosp Epidemiol 27(2):155–169
Bradley SJ, Wilson ALT, Allen MC, Sher HA, Goldstone AH, Scott GM (1999) The control of hyperendemic glycopeptide-resistant Enterococcus spp. on a haematology unit by changing antibiotic usage. J Antimicrob Chemother 43(2):261–266. doi:10.1093/jac/43.2.261
Lipworth AD, Hyle EP, Fishman NO, Nachamkin I, Bilker WB, Marr AM et al (2006) Limiting the emergence of extended-spectrum β-lactamase-producing Enterobacteriaceae: influence of patient population characteristics on the response to antimicrobial formulary interventions. Infect Control Hosp Epidemiol 27(3):279–286
Borer A, Eskira S, Nativ R, Saidel-Odes L, Riesenberg K, Livshiz-Riven I et al (2011) A multifaceted intervention strategy for eradication of a hospital-wide outbreak caused by carbapenem-resistant Klebsiella pneumoniae in Southern Israel. Infect Control Hosp Epidemiol 32:1158–1165. doi:10.1086/662620
Toltzis P, Yamashita T, Vilt L, Green M, Morrissey A, Spinner-Block S et al (1998) Antibiotic restriction does not alter endemic colonization with resistant gram-negative rods in a pediatric intensive care unit. Crit Care Med 26:1893–1899
Charbonneau P, Parienti JJ, Thibon P, Ramakers M, Daubin C, du Cheyron D et al (2006) Fluoroquinolone use and methicillin-resistant Staphylococcus aureus isolation rates in hospitalized patients: a quasi experimental study. Clin Infect Dis 42(6):778–784. doi:10.1086/500319
de Man P, Verhoeven BAN, Verbrugh HA, Vos MC, van den Anker JN (2000) An antibiotic policy to prevent emergence of resistant bacilli. Lancet 355:973–978. doi:10.1016/S0140-6736(00)90015-1
Butler CC, Dunstan F, Heginbothom M, Mason B, Roberts Z, Hillier S et al (2007) Containing antibiotic resistance: decreased antibiotic-resistant coliform urinary tract infections with reduction in antibiotic prescribing by general practices. Br J Gen Pract 57:785–792
Goossens H, Ferech M, Vander Stichele R, Elseviers M; ESAC Project Group (2005) Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet 365(9459):579–587. doi:10.1016/S0140-6736(05)17907-0
Donnan PT, Wei L, Steinke DT, Phillips G, Clarke R, Noone A et al (2004) Presence of bacteriuria caused by trimethoprim resistant bacteria in patients prescribed antibiotics: multilevel model with practice and individual patient data. BMJ 328(7451):1297
Vander Stichele RH, Elseviers MM, Ferech M, Blot S, Goossens H; ESAC Project Group (2004) European Surveillance of Antimicrobial Consumption (ESAC): data collection performance and methodological approach. Br J Clin Pharmacol 58(4):419–428. doi:10.1111/j.1365-2125.2004.02164.x
Greenland S, Robins J (1994) Invited commentary: ecologic studies—biases, misconceptions, and counterexamples. Am J Epidemiol 139(8):747–760
Harbarth S, Harris AD, Carmeli Y, Samore MH (2001) Parallel analysis of individual and aggregated data on antibiotic exposure and resistance in gram-negative bacilli. Clin Infect Dis 33(9):1462–1468. doi:10.1086/322677
Muller A, Mauny F, Talon D, Donnan PT, Harbarth S, Bertrand X (2006) Effect of individual- and group-level antibiotic exposure on MRSA isolation: a multilevel analysis. J Antimicrob Chemother 58(4):878–881. doi:10.1093/jac/dkl343
Campbell MJ, Donner A, Klar N (2007) Developments in cluster randomized trials and Statistics in Medicine. Stat Med 26:2–19. doi:10.1002/sim.2731
Klar N, Donner A (2001) Current and future challenges in the design and analysis of cluster randomization trials. Stat Med 20:3729–3740. doi:10.1002/sim.1115
Loeb MB (2002) Application of the development stages of a cluster randomized trial to a framework for valuating complex health interventions. BMC Health Serv Res 2(1):13
de Smet AMGA, Kluytmans JAJW, Cooper BS, Mascini EM, Benus RFJ, van der Werf TS et al (2009) Decontamination of the digestive tract and oropharynx in ICU patients. N Engl J Med 360(1):20–31. doi:10.1056/NEJMoa0800394
de Smet AMGA, Kluytmans JAJW, Blok HEM, Mascini EM, Benus RFJ, Bernards AT et al (2011) Selective digestive tract decontamination and selective oropharyngeal decontamination and antibiotic resistance in patients in intensive-care units: an open-label, clustered group-randomised, crossover study. Lancet Infect Dis 11:372–380. doi:10.1016/S1473-3099(11)70035-4
Skalet AH, Cevallos V, Ayele B, Gebre T, Zhou Z, Jorgensen JH et al (2010) Antibiotic selection pressure and macrolide resistance in nasopharyngeal Streptococcus pneumoniae: a cluster-randomized clinical trial. PLoS Med 7(12):e1000377. doi:10.1371/journal.pmed.1000377
Parm Ü, Metsvaht T, Sepp E, Ilmoja M-L, Pisarev H, Pauskar M et al (2010) Impact of empiric antibiotic regimen on bowel colonization in neonates with suspected early onset sepsis. Eur J Clin Microbiol Infect Dis 29:807–816. doi:10.1007/s10096-010-0931-1
Hadorn DC, Baker D, Hodges JS, Hicks N (1996) Rating the quality of evidence for clinical practice guidelines. J Clin Epidemiol 49:749–754. doi:10.1016/0895-4356(96)00019-4
Harris RP, Helfand M, Woolf SH, Lohr KN, Mulrow CD, Teutsch SM et al (2001) Current methods of the U.S. Preventive Services Task Force: a review of the process. Am J Prev Med 20:21–35. doi:10.1016/S0749-3797(01)00261-6
McKee M, Britton A, Black N, McPherson K, Sanderson C, Bain C (1999) Methods in health services research. Interpreting the evidence: choosing between randomised and non-randomised studies. BMJ 319(7205):312–315
Demissie K, Mills OF, Rhoads GG (1998) Empirical comparison of the results of randomized controlled trials and case–control studies in evaluating the effectiveness of screening mammography. J Clin Epidemiol 51:81–91. doi:10.1016/S0895-4356(97)00243-6
LeLorier J, Grégoire G, Benhaddad A, Lapierre J, Derderian F (1997) Discrepancies between meta-analyses and subsequent large randomized, controlled trials. N Engl J Med 337(8):536–542. doi:10.1056/NEJM199708213370806
Blettner M, Sauerbrei W, Schlehofer B, Scheuchenpflug T, Friedenreich C (1999) Traditional reviews, meta-analyses and pooled analyses in epidemiology. Int J Epidemiol 28(1):1–9. doi:10.1093/ije/28.1.1
Lau J, Ioannidis JP, Schmid CH (1998) Summing up evidence: one answer is not always enough. Lancet 351(9096):123–127. doi:10.1016/S0140-6736(97)08468-7
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D et al (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA 283(15):2008–2012. doi:10.1001/jama.283.15.2008
Ioannidis JP, Cappelleri JC, Lau J (1998) Meta-analyses and large randomized, controlled trials. N Engl J Med 338(1):59. doi:10.1056/NEJM199801013380112, author reply 61–62
Stroup DF, Thacker SB, Olson CM, Glass RM, Hutwagner L (2001) Characteristics of meta-analyses related to acceptance for publication in a medical journal. J Clin Epidemiol 54:655–660. doi:10.1016/S0895-4356(00)00362-0
Tacconelli E, De Angelis G, Cataldo MA, Pozzi E, Cauda R (2008) Does antibiotic exposure increase the risk of methicillin-resistant Staphylococcus aureus (MRSA) isolation? A systematic review and meta-analysis. J Antimicrob Chemother 61:26–38. doi:10.1093/jac/dkm416
Carmeli Y, Samore MH, Huskins C (1999) The association between antecedent vancomycin treatment and hospital-acquired vancomycin-resistant enterococci: a meta-analysis. Arch Intern Med 159(20):2461–2468
Gafter-Gvili A, Paul M, Fraser A, Leibovici L (2007) Effect of quinolone prophylaxis in afebrile neutropenic patients on microbial resistance: systematic review and meta-analysis. J Antimicrob Chemother 59(1):5–22. doi:10.1093/jac/dkl425
Bliziotis IA, Samonis G, Vardakas KZ, Chrysanthopoulou S, Falagas ME (2005) Effect of aminoglycoside and beta-lactam combination therapy versus beta-lactam monotherapy on the emergence of antimicrobial resistance: a meta-analysis of randomized, controlled trials. Clin Infect Dis 41(15):149–158. doi:10.1086/430912
Counsell C (1997) Formulating questions and locating primary studies for inclusion in systematic reviews. Ann Intern Med 127(5):380–387
Meade MO, Richardson WS (1997) Selecting and appraising studies for a systematic review. Ann Intern Med 127(7):531–537
Lau J, Ioannidis JPA, Schmid CH (1997) Quantitative synthesis in systematic reviews. Ann Intern Med 127(9):820–826
Thompson SG (1994) Systematic review: why sources of heterogeneity in meta-analysis should be investigated. BMJ 309(6965):1351–1355. doi:10.1136/bmj.309.6965.1351
Higgins JPT, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21(11):1539–1558. doi:10.1002/sim.1186
Weinstein RA, Bonten MJM, Austin DJ, Lipsitch M (2001) Understanding the spread of antibiotic resistant pathogens in hospitals: mathematical models as tools for control. Clin Infect Dis 33(10):1739–1746. doi:10.1086/323761
Grundmann H, Hellriegel B (2006) Mathematical modelling: a tool for hospital infection control. Lancet Infect Dis 6:39–45. doi:10.1016/S1473-3099(05)70325-X
D’Agata EMC, Magal P, Olivier D, Ruan S, Webb GF (2007) Modeling antibiotic resistance in hospitals: the impact of minimizing treatment duration. J Theor Biol 249(3):487–499. doi:10.1016/j.jtbi.2007.08.011
Geli P, Laxminarayan R, Dunne M, Smith DL (2012) “One-Size-Fits-All”? Optimizing treatment duration for bacterial infections. PLoS One 7:e29838. doi:10.1371/journal.pone.0029838
D’Agata EMC, Dupont-Rouzeyrol M, Magal P, Olivier D, Ruan S (2008) The impact of different antibiotic regimens on the emergence of antimicrobial-resistant bacteria. PLoS One 3:e4036. doi:10.1371/journal.pone.0004036
Bonhoeffer S, Lipsitch M, Levin BR (1997) Evaluating treatment protocols to prevent antibiotic resistance. Proc Natl Acad Sci U S A 94(22):12106–12111
Bergstrom CT, Lo M, Lipsitch M (2004) Ecological theory suggests that antimicrobial cycling will not reduce antimicrobial resistance in hospitals. Proc Natl Acad Sci U S A 101(36):13285–13290. doi:10.1073/pnas.0402298101
Kouyos RD, Abel Zur Wiesch P, Bonhoeffer S (2011) Informed switching strongly decreases the prevalence of antibiotic resistance in hospital wards. PLoS Comput Biol 7(3):e1001094. doi:10.1371/journal.pcbi.1001094
Acknowledgement
We would like to thank Dr. François Rousset for critically reading this manuscript.
Conflict of interest
All authors: no reported conflicts.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Angebault, C., Andremont, A. Antimicrobial agent exposure and the emergence and spread of resistant microorganisms: issues associated with study design. Eur J Clin Microbiol Infect Dis 32, 581–595 (2013). https://doi.org/10.1007/s10096-012-1795-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-012-1795-3