
Abstract
The purpose of this investigation was to provide a comprehensive review of the pathogenic role and spectrum of disease of milleri group streptococci, with special attention to bloodstream invasion and to possible differential roles among the three species. All consecutive isolates of milleri group streptococci from any anatomic source, during a 37-month period, in a tertiary care teaching hospital in Tel-Aviv, Israel, were thoroughly investigated. Identification to the species level was performed by an automated system.Streptococcus anginosus constituted 82% of the 245 patient-unique isolates from hospitalized patients. All nonurinary isolates were involved in pyogenic infections mostly originating from the gastrointestinal tract, with bacteremia in 28 cases. The 71 urinary isolates represented either urinary tract infection or nonsignificant bacteriuria. No specific association could be detected between species and the infection site, except for a higher relative representation of Streptococcus constellatus in bacteremia. Milleri group streptococci are common in clinical practice and play a different pathogenic role to other viridans streptococci. Due to their invariable association with pyogenic processes, their presence in blood warrants immediate focus identification. In addition, they have a previously unappreciated clinical niche concerning urinary tract infection. The identification of viridans streptococci to the species level is of paramount clinical significance.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Streptococcus anginosus, Streptococcus constellatus, and Streptococcus intermedius, collectively termed “S. anginosus group” or “Streptococcus milleri group” (SMG), constitute three genetically distinct but phenotypically heterogeneous groups of microorganisms with variable hemolytic, biochemical, and Lancefield group patterns [1–4]. Until the 2000s, most clinical microbiology laboratories did not routinely distinguish SMG species from among other commensal viridans streptococci, mainly because of the labor-intensive techniques required and the confusing results concerning terminology and classification [1], and partly because of the low awareness of the clinical significance of such distinction. With the advent of automated identification systems, especially their second and third generations, the identification of viridans streptococci to the species level became more widely available, mostly in well-equipped academic laboratories. Furthermore, awareness of their particular pathogenicity compared to other viridans streptococci provoked renewed interest in this specific group of microorganisms [2]. Although the unique propensity of SMG to cause pyogenic infection was known for years [3, 4], the entire clinical spectrum has not been widely studied, even recently. Clinical studies performed before the wide availability of advanced automated systems mostly included selected isolates for which a clinical situation urged microbiological workup, such as cases of bacteremia [5–10]. Other reports mostly dealt with either single-source isolates (thoracic cavity, brain, appendix, perianal site, sinuses, etc.) or specific groups of patients (pediatric population, solid organ recipients, cystic fibrosis patients, etc.) [11–22], but population-based comprehensive clinical studies on all-source isolates of SMG are still scarce [23–26].
This study investigated the epidemiology, sources, and foci of infection and clinical relevance of all consecutive isolates of SMG during a period of three years in a large, tertiary care university hospital in Tel-Aviv, Israel, providing a comprehensive review of the pathogenic role and the spectrum of disease of SMG in an everyday clinical setting.
Materials and methods
Patients and clinical data collection
The Tel-Aviv Sourasky Medical Center is a 1,150-bed tertiary care teaching hospital located in central Tel-Aviv and serving a population of about 700,000, with approximately 90,000 admissions annually. All cases with growth of SMG (S. anginosus, S. constellatus, and S. intermedius) from any specimen during a 37-month period (1/12/00 to 31/12/03) were included in this study. In case of more than one isolate per patient, it was counted only once, thus, computing only patient-unique isolates. The medical records and infectious diseases files of the patients were reviewed, pertinent demographic, bacteriological, and clinical data were collected, and the presumptive focus of infection was determined by an infectious diseases specialist, considering all of the available information together.
Bacteriological methods
Isolates were identified by standard bacteriologic methods and the automated VITEK 2 system (bioMérieux, Durham, NC, USA), and in accordance with the Clinical and Laboratory Standards Institute (CLSI) guidelines. Streptococci were identified to the species level by the use of the ID-GP card within the VITEK 2 system. Blood cultures were incubated in the BacT/ALERT system (bioMérieux, Durham, NC, USA).
Definitions
Community-acquired (CA) infection was defined when the specimen was taken within the first 72 h of admission.
Hospital-acquired (HA) infection was defined when the specimen was taken after the first 72 h or when the infection has developed following recent previous hospitalization.
Mixed infection was defined when additional microorganisms grew from the specimen that grew SMG or from another specimen taken from the same site on the same date.
Urinary tract infection (UTI) was defined in patients who had SMG growing from urine in counts of at least 104 cells/ml (or from blood in the absence of clinical findings suggesting another focus of infection), and had urinary symptoms and/or inflammatory findings in urinalysis. Otherwise, the growth of SMG from urine was defined as nonsignificant bacteriuria.
Statistical analysis
Comparisons among patient groups for categorical variables were performed using Chi-square analysis or Fisher’s exact test, as applicable.
Results
A total of 346 patient-unique isolates of SMG were consecutively recovered during the 37-month study period. Clinical information from hospital records could be retrieved for 245 patients who were hospitalized either at the time of specimen collection or shortly before or after this date. No clinical information could be retrieved for 101 patients, most of whom were not hospitalized. The annual incidence of SMG isolation was estimated to be 8.8/10,000 hospital admissions.
The 245 hospitalized patients included 110 (45%) men and 135 women. The mean age was 53 ± 22, range 2 months to 94 years, median 55. Ninety-eight (40%) patients were 61 years or older, 75 (31%) were 40–60 years old, 55 (22%) were 19–39 years old, and 17 (7%) patients were 18 years or younger (seven of whom were under 10 years old).
S. anginosus was, by far, the most common species with 202 (82%) isolates, followed by S. constellatus (11%) and S. intermedius (6%) (Table 1).
One hundred and thirty-eight (56%) patients had one or more underlying conditions; 50 had malignant diseases (half of which were tumors of the gastrointestinal tract), 30 had diabetes mellitus, seven were injecting illicit drugs, seven had obstructive uropathy, five had kidney transplant, five had inflammatory bowel disease, and others had various additional co-morbidities.
The most common source of isolation of SMG was pus from various anatomic locations (appendix, perianal site, intraabdominal collection, and others), constituting together 35% (86/245) of cases, closely followed by urine with 29% (71/245) of cases (Table 1). Isolation from blood constituted 11% (28/245) of cases.
Of note, there was a higher relative representation of S. constellatus among blood isolates than that among the total isolates (8/28, 29% vs. 28/245, 11%, p < 0.01), whereas S. intermedius was recovered from wounds more often than its relative proportion among all isolates (6/41, 15% vs. 15/245, 6%, p = 0.05).
Seventy-one patients had SMG growing from urine, 22 of whom had UTI and 49 were defined as having nonsignificant bacteriuria. Among the 24 patients with true UTI (including two with bacteremia and no bacteriuria), six patients had various relevant associated conditions: nephrolithiasis (3), other obstructive uropathy (2), and bladder tumor (1), and five others had recurrent UTI without underlying cofactors. The 24 species from UTI cases were S. anginosus (21), S. constellatus (2), and S. intermedius (1), and three of the S. anginosus cases were mixed with E. coli (2) and Proteus (1).
The 49 patients with nonsignificant bacteriuria (20% of 245 patients, 42 women and seven men) were hospitalized for various noninfectious diagnoses, although four of them were admitted with suspected infectious diarrhea that resolved rapidly (one of whom had Campylobacter in stool). Nine of the 49 patients had various conditions that could be linked with bacteriuria [kidney transplant (5), bladder tumor (2), and nephrolithiasis (2)].
The focus of infection and place of acquisition of the infection could be identified in virtually all of the 196 patients with clinically significant SMG infection (excluding the 49 nonsignificant bacteriuria cases) (Table 2).
One hundred and forty four patients (73% of 196) had CA infections, most of whom had a spontaneous purulent focus of infection originating from the gastrointestinal tract. Perianal abscesses, appendicitis, cholangitis, peritonitis, and liver abscesses constituted together 47% (67/144) of the CA infections. Except for UTI (16%), other foci were also associated with pus formation (empyema, diabetic septic foot, tooth abscess, etc.) (Table 2).
Fifty-two patients (27% of 196) had HA infections that mostly developed as complications of surgery (43/52, 83%), particularly in abdominal operations (Table 2). All other nonsurgical infections were also purulent processes, except for one UTI (not associated with urinary catheter). There was no difference in the distribution of SMG species between HA and CA cases.
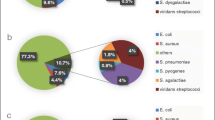
Eighty-seven patients (44% of 196) had mixed infection, yielding 106 additional microorganisms: Escherichia coli (42), Klebsiella-Enterobacter (16), Pseudomonas (8), Proteus-Morganella-Providencia (6), other Gram-negative (5), Staphylococcus aureus (12), various streptococci (9), Enterococcus (7), and Candida (1). Six (21%) of the 28 bacteremic patients had mixed infections that were included in the above list of additional microorganisms. They included: S. aureus in a case of pulmonary infection, streptococcus group G in a case of an upper arm abscess in a drug addict, Candida in a case of an intraabdominal abscess, S. bovis in a case of liver abscess, E. coli and Proteus in a case of cholangitis, and Klebsiella in a case of unknown focus (due to paucity of clinical information). Among the 49 patients who had nonsignificant bacteriuria, only five had additional growth of E. coli in urine. Mixed infection was slightly more prevalent among HA infections (28/52, 54% vs. 59/144, 41%), but it did not reach statistical significance.
Twenty-eight of the 196 patients (14%) were bacteremic with SMG growing from blood, 21 of whom had an identified focus of infection (Table 2). The same species grew from the focus of infection and from blood in three cases (diabetic finger, intraabdominal abscess, and surgical wound), and one patient with phlegmonous appendicitis had growth from blood and urine but not from the site of infection. Seven patients had bacteremia with no identified focus (one of whom was neutropenic), mostly due to lack of information.
Three patients died during hospitalization, all of whom had S. anginosus monomicrobial bacteremia.
Discussion
Although molecular techniques are considered to be the most sensitive and specific methods for the identification of viridans streptococci to the species level, the VITEK 2 GP identification card was found to provide reliable results for the identification of Gram-positive cocci under routine laboratory conditions, correctly identifying more than 94% of the isolates tested [27]. Another study that compared pyrosequencing of the 16S rRNA gene to the VITEK 2 system in diagnosing alpha-hemolytic streptococci showed some false-negative results for the latter [28], but, to the best of our knowledge, no false-positive results were described with the VITEK 2 system for the identification of SMG. The implication of this is that our estimates may be either a modest underestimation or a true assessment of the extent of SMG infection.
The annual incidence of SMG isolation was estimated here to be 8.8/10,000 hospitalized patients in a tertiary care institute. The only study that estimated the population-based incidence of SMG infection found it to be 8.65/100,000 population in the Calgary Health Region, Alberta, Canada [26]. Moreover, this incidence was significantly higher than that of each of the other individual pyogenic streptococcus species, such as group A, B, and C + G (4.27, 3.13, and 2.24/100,000, respectively) [26]. This unexpectedly high frequency demonstrates the importance of SMG as a pathogen, deserving the designation of “the unrecognized pathogen” [29] and “the elusive pathogen” [2].
Demographically, our study showed that SMG infection was distributed among all age groups, with some preponderance for adults and the elderly. The few other studies supplying patients’ demography gave similar results [3, 23, 26]. However, a series of 188 children collected over a period of 6.5 years at Boston’s Children’s Hospital suggests that SMG infection is not uncommon among children as well [18]. In contrast to other studies which demonstrated significant male predominance [18, 23, 24, 26], the present study found a slight female preponderance (1.2:1), but this disappeared when the nonsignificant bacteriuria group was excluded.
A high frequency of underlying conditions seems to characterize SMG infections. More than half (56%) of the patients in this study, as well as 66–77% in other series, had at least one co-morbidity or a risk factor [3, 23], many of which were associated with undergoing surgery.
When dealing with purulent infections, it is not surprising that many of the infections (44% in this study) were polymicrobial. Most other studies found even higher proportions of 46–76% of mixed infections [3, 18, 23, 25]. Enterobacteriaceae, bowel anaerobes, and Eikenella were the most common co-pathogens in the other studies, while Enterobacteriaceae, S. aureus, and various other streptococci were more prevalent in the present study.
A unique finding of the present study is the large group of isolates cultured from urine, none of which represented a purulent focus in the urinary system. Although SMG is not known to be associated with UTI, single cases of true UTI were reported in previous studies among clinically significant SMG isolates [9, 23, 26], and larger numbers of isolates from “genitourinary source” without providing clinical information or with designations of “no disease” or “questionable significance” were reported in a few other publications [3, 4, 24, 25]. All of the 22 patients diagnosed here as having SMG UTI by urine culture had pure growth (except for three mixed cultures) of at least 104 cells/ml, and had signs and symptoms of UTI. Many of these had short hospitalization with no alternative diagnosis, while a few had more complicated courses due to their co-morbidities. Could any of these urine isolates represent a purulent focus somewhere else with undetected, low-grade bacteremia and secondary bacteriuria? Such a scenario is theoretically plausible, especially when considering the patient who had phlegmonous appendicitis and SMG growing only from blood and urine. However, none of the other 71 patients with urinary isolates had any clinical hint for the presence of another focus of infection. The limited referral to urine isolates in previous studies might be due to not performing species identification on streptococci from urine or to not investigating the clinical significance of such a finding. These data represent a previously unappreciated clinical role of SMG in causing UTI.
Also challenging is the question as to whether there was a differential pathogenic role among the three species. The literature review suggested wide variability in the association between any particular species and the source of isolation, but most connections did not hold across studies. It was claimed that S. intermedius was more frequently isolated from infections of the CNS and liver, S. constellatus more often from blood and respiratory infections, and S. anginosus from most categories excluding CNS infection [4, 18, 24]. Claridge et al. found that S. anginosus was significantly less associated with abscesses than the other species [25]. The present findings could support only the association of S. constellatus with bacteremia, but other associations could not be verified. If any of the species were less involved in abscesses in the present study, it was S. intermedius (and not S. anginosus) that was more prevalent among wound cultures than among true abscesses, a difference that does not seem to be of great importance. Jackson et al. demonstrated that S. intermedius was more prevalent in children [20]; however, no age–species predilection was noted in the present study and no information about species was given in the large collection of SMG from children [18]. These large variations among studies may possibly reflect random differences between the specific case mix.
Bacteremia was detected in 11% (28/245) of the total series or 14% when calculated only among clinical significant isolates. Similar proportions of 7% and 12%, respectively, were reported in the largest published collection of 518 consecutively recovered all-source isolates [24]. A larger proportion of isolates from blood (27%) was described in only one study among 122 clinically significant isolates [25]. Other large collections (one among children) reported bacteremia in 3% only [4, 10, 18].
Six studies describing only SMG bacteremia [5–10] were summarized together with data from the present study, encompassing collectively 215 bacteremic patients (Table 3). Not surprisingly, the vast majority of cases represented secondary invasion from purulent foci in various systems, which indicates the importance of focus identification in such cases. Endocarditis, being absent from our series, constituted only 4% of total, and was significantly represented (6/32) in only one study [6]. Most features of infection in these seven series on bacteremia were not essentially different from each other. Wide age range, male predominance, multiplicity of underlying conditions, presence of polymicrobial growth in about one quarter of cases, and predominance of CA infection were similar. The average mortality of 16% in bacteremia stands in contrast with the absence of mortality in nonbacteremic cases. Indeed, all three fatal cases in the present series involved bacteremia (S. anginosus alone).
In summary, milleri (anginosus) group streptococci were demonstrated to be pyogenic pathogens, not uncommon in clinical practice, infecting all types of patients and involving multiple body sites. In addition, a significant part of the cases involved UTI, a previously almost unrecognized clinical mode of SMG behavior. It seems that identification of viridans streptococci to the species level has paramount importance in appreciating their clinical role and pathogenicity.
References
Facklam R (2002) What happened to the streptococci: overview of taxonomic and nomenclature changes. Clin Microbiol Rev 15:613–630
Piscitelli SC, Shwed J, Schreckenberger P, Danziger LH (1992) Streptococcus milleri group: renewed interest in an elusive pathogen. Eur J Clin Microbiol Infect Dis 11:491–498
Gossling J (1988) Occurrence and pathogenicity of the Streptococcus milleri group. Rev Infect Dis 10:257–285
Whiley RA, Beighton D, Winstanley TG, Fraser HY, Hardie JM (1992) Streptococcus intermedius, Streptococcus constellatus, and Streptococcus anginosus (the Streptococcus milleri group): association with different body sites and clinical infections. J Clin Microbiol 30:243–244
Jacobs JA, Pietersen HG, Stobberingh EE, Soeters PB (1994) Bacteremia involving the “Streptococcus milleri” group: analysis of 19 cases. Clin Infect Dis 19:704–713
Casariego E, Rodriguez A, Corredoira JC, Alonso P, Coira A, Bal M, López MJ, Varela J (1996) Prospective study of Streptococcus milleri bacteremia. Eur J Clin Microbiol Infect Dis 15:194–200
Salavert M, Gómez L, Rodriguez-Carballeira M, Xercavins M, Freixas N, Garau J (1996) Seven-year review of bacteremia caused by Streptococcus milleri and other viridans streptococci. Eur J Clin Microbiol Infect Dis 15:365–371
Bert F, Bariou-Lancelin M, Lambert-Zechovsky N (1998) Clinical significance of bacteremia involving the “Streptococcus milleri” group: 51 cases and review. Clin Infect Dis 27:385–387
Weightman NC, Barnham MR, Dove M (2004) Streptococcus milleri group bacteraemia in North Yorkshire, England (1989–2000). Indian J Med Res 119(Suppl):164–167
Stelzmueller I, Pfausler B, Fille M, Dossett LA, Bonatti H (2009) Streptococcus milleri group isolates from blood cultures: consider surgical sepsis. Surg Infect (Larchmt) 10:259–263
Stelzmueller I, Biebl M, Berger N, Eller M, Mendez J, Fille M, Angerer K, Schmid T, Lorenz I, Margreiter R, Bonatti H (2007) Relevance of group milleri streptococci in thoracic surgery: a clinical update. Am Surg 73:492–497
Ripley RT, Cothren CC, Moore EE, Long J, Johnson JL, Haenel JB (2006) Streptococcus milleri infections of the pleural space: operative management predominates. Am J Surg 192:817–821
Kowlessar PI, O’Connell NH, Mitchell RD, Elliott S, Elliott TS (2006) Management of patients with Streptococcus milleri brain abscesses. J Infect 52:443–450
Hardwick RH, Taylor A, Thompson MH, Jones E, Roe AM (2000) Association between Streptococcus milleri and abscess formation after appendicitis. Ann R Coll Surg Engl 82:24–26
Stelzmueller I, Aigner F, Albright J, Margreiter R, Fille M, Swenson BR, Dossett L, Bonatti H (2010) Group Milleri Streptococci in perianal infections. Colorectal Dis 12:e121–e127
Rankhethoa NM, Prescott CA (2008) Significance of Streptococcus milleri in acute rhinosinusitis with complications. J Laryngol Otol 122:810–813
Hirai T, Kimura S, Mori N (2005) Head and neck infections caused by Streptococcus milleri group: an analysis of 17 cases. Auris Nasus Larynx 32:55–58
Belko J, Goldmann DA, Macone A, Zaidi AKM (2002) Clinically significant infections with organisms of the Streptococcus milleri group. Pediatr Infect Dis J 21:715–723
Stelzmueller I, Fille M, Hager J, Dossett L, Sifri CD, Bonatti H (2009) Group Milleri Streptococci in paediatric infections. Eur J Pediatr Surg 19:21–24
Jackson DS, Welch DF, Pickett DA, Mukwaya GM, Kuhls TL (1995) Suppurative infections in children caused by non-beta-hemolytic members of the Streptococcus milleri group. Pediatr Infect Dis J 14:80–82
Stelzmueller I, Berger N, Wiesmayr S, Eller M, Tabarelli W, Fille M, Margreiter R, Bonatti H (2007) Group milleri streptococci: significant pathogens in solid organ recipients. Transpl Int 20:51–56
Parkins MD, Sibley CD, Surette MG, Rabin HR (2008) The Streptococcus milleri group—an unrecognized cause of disease in cystic fibrosis: a case series and literature review. Pediatr Pulmonol 43:490–497
Molina JM, Leport C, Bure A, Wolff M, Michon C, Vilde JL (1991) Clinical and bacterial features of infections caused by Streptococcus milleri. Scand J Infect Dis 23:659–666
Jacobs JA, Pietersen HG, Stobberingh EE, Soeters PB (1995) Streptococcus anginosus, Streptococcus constellatus and Streptococcus intermedius. Clinical relevance, hemolytic and serologic characteristics. Am J Clin Pathol 104:547–553
Claridge JE 3rd, Attorri S, Musher DM, Hebert J, Dunbar S (2001) Streptococcus intermedius, Streptococcus constellatus, and Streptococcus anginosus (“Streptococcus milleri group”) are of different clinical importance and are not equally associated with abscess. Clin Infect Dis 32:1511–1515
Laupland KB, Ross T, Church DL, Gregson DB (2006) Population-based surveillance of invasive pyogenic streptococcal infection in a large Canadian region. Clin Microbiol Infect 12:224–230
Funke G, Funke-Kissling P (2005) Performance of the new VITEK 2 GP card for identification of medically relevant gram-positive cocci in a routine clinical laboratory. J Clin Microbiol 43:84–88
Haanperä M, Jalava J, Huovinen P, Meurman O, Rantakokko-Jalava K (2007) Identification of alpha-hemolytic streptococci by pyrosequencing the 16S rRNA gene and by use of VITEK 2. J Clin Microbiol 45:762–770
Ruoff KL (1988) Streptococcus anginosus (“Streptococcus milleri”): the unrecognized pathogen. Clin Microbiol Rev 1:102–108
Conflict of interest
All authors: none.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Siegman-Igra, Y., Azmon, Y. & Schwartz, D. Milleri group streptococcus—a stepchild in the viridans family. Eur J Clin Microbiol Infect Dis 31, 2453–2459 (2012). https://doi.org/10.1007/s10096-012-1589-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-012-1589-7