
Abstract
In 1999, the costs of gastroenteritis in the Netherlands were estimated using data on hospitalizations from national registries, together with data on etiology and self-reported data on health care resource use in a community-based study. Now, more information on hospitalizations is available and these data were used to update the total costs of gastroenteritis in the Netherlands. The costs of severe gastroenteritis in the Netherlands were estimated in more depth using a hospital-based study, with patient questionnaires including a follow-up period of 6 months. The overall costs of gastroenteritis were calculated taking direct medical costs, direct non-medical costs, and indirect non-medical costs into account. The costs for severe gastroenteritis in 2009 were estimated at €2,203 per hospitalized child and €6,834 per hospitalized adult. The overall costs of gastroenteritis in 2009 were estimated at €611–695 million, which is €133–151 per gastroenteritis case or €37–42 per inhabitant. The total health care costs for gastroenteritis were about 50% higher in 2009 compared to 1999, which is mostly due to the rise in health care costs. The costs per gastroenteritis episode in adults are higher compared to children, mainly due to differences in the reasons for hospitalization and course of disease, and productivity losses.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Infectious gastroenteritis causes a considerable burden of morbidity and mortality worldwide. This burden is mainly due to the large number of cases affected, as the course of gastroenteritis in the majority of cases is mild and short-term, at least in the western world. In developing countries, gastroenteritis is a major cause of death, especially in young children [1]. The infectious causes of gastroenteritis include a wide array of bacteria, viruses, and parasites, with different capacities of causing severe illness. Vaccines against infectious gastroenteritis are scares; however, two vaccines against rotavirus are available (Rotarix™ and RotaTeq®) [2, 3]. The rotavirus causes gastroenteritis especially in infants and young children [4], but the virus can also cause disease in adults [5]. None of the two vaccines are included in the Dutch national childhood immunization program. One reason for not including it is that it is not expected to be cost-effective [6, 7]. The economic burden is one important input for the assessment of the cost-effectiveness of possible intervention measures for infectious gastroenteritis to support decision-making. In the Netherlands, earlier estimates showed an incidence of gastroenteritis of 283 per 1,000 person-years, which amounts to approximately 4.5 million episodes per year [8]. Only about 5% of the cases visited a general practitioner (GP) for their complaints [9]. Based on these data, the costs of all gastroenteritis were estimated at €345 million in 1999 [10]. In general, these costs were mainly driven by the hospitalized cases. Data on hospitalization for these cost estimates were taken from national registries, with incomplete information on the causative agent, and from a community-based study, in which hospitalizations were rarely reported. Therefore, a hospital-based study was conducted in the Netherlands to assess the incidence and etiology of gastroenteritis requiring hospitalization: the GEops study [11, 12]. In the GEops study, the incidence of severe gastroenteritis, which is defined as requiring hospitalization, was estimated at 2.92 per 1,000 children and 0.41–0.94 per 1,000 adults. Overall, 0.2–1.3% of the children and 0.01–0.1% of the adults with gastroenteritis will be hospitalized.
The aim of the present study is to present new estimations of the costs for all gastroenteritis in the Netherlands, as well as presenting the age group-dependent cost per case of severe gastroenteritis.
Methods
Cost per case of severe gastroenteritis
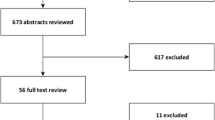
The data needed for the estimation of costs of severe gastroenteritis were collected as an integral part of the Dutch study of gastroenteritis requiring hospitalization (GEops study). The design and methods have been described in detail by Friesema et al. [11], and the results on incidence and etiology have been published elsewhere, separately for children [11] and adults [12]. In short, five general hospitals and one academic hospital enrolled patients to the study over a period of approximately one year between May 2008 and November 2009. Patients admitted to the hospital with symptoms of gastroenteritis were eligible for inclusion. Gastroenteritis was defined as: diarrhea (three or more episodes in 24 h), or vomiting (three or more episodes in 24 h), or diarrhea or vomiting together with two or more other symptoms (vomiting/diarrhea, stomach ache, abdominal cramps, nausea, fever, blood in stool, mucus in stool). This case definition was also used in the previous community- and GP-based studies [8, 13]. Inclusion consisted of obtaining written (parental) consent to provide epidemiological and clinical information, and collecting a fecal sample. Cases, or their parents, were asked to complete one questionnaire shortly after discharge from the hospital and another questionnaire at three months’ follow-up. For participants with possible complications at the three months’ follow-up, a second follow-up questionnaire was sent six months after the hospitalization. All three questionnaires contained items about the use of health care services, methods of transportation to the health care services, and absence from work by the participant or care-givers, to cover the whole episode of gastroenteritis.
Economic burden of gastroenteritis in the Netherlands
The costs of severe gastroenteritis were used to update the total economic burden of gastroenteritis in the Netherlands. Besides the data from the GEops study, the data used in the 1999 estimates were extracted from the publication of van den Brandhof et al. [10]. In 1999, hospital admissions were estimated by two different methods: using data from a community-based prospective cohort study [8] and extracting data from the National Medical Registry (NMR). The NMR is based upon diagnoses using ICD-9 codes. Gastroenteritis was defined as ICD-codes 001–009 and 558 [10]. We compared the hospitalization data from the NMR to the estimates from the GEops study, partly to be able to compare with the earlier cost estimates from 1999. The same cost items as in 1999 were included in order to allow comparison between the earlier and the current estimates. However, there are some exceptions: we did not include the costs of medication nor treatment by alternative health care providers (such as homeopaths) in the GEops study, as these were very rarely reported in the cohort study. In the cohort study, only three hospitalizations were reported. For the estimation of the total costs of gastroenteritis in the Netherlands, the incidence rates from the community-based prospective cohort study of 1999 were used [8] and applied to the structure of the population in 2009.
Unit costs
Costs were divided into direct medical costs (use of health care services), direct non-medical costs (transport costs), and indirect non-medical costs (costs of absence from work, productivity losses). Unit costs were gathered from Hakkart-van Roijen et al. [14] and expressed in 2009 prices (Table 1). Some assumptions about transportation costs had to be made: in the evenings and weekends, GPs can only be visited in specific GP centers which are mostly located next to the hospital: for these GP visits, the average distance to a hospital is used. The transport costs entails going by car (including parking fee) or taxi or coming with an ambulance. Productivity losses were estimated as absence from work for both participants as care-givers, using the friction cost method. Costs were calculated in hours absent from both paid and unpaid work due to care-giving, sick leave, or death. Productivity losses due to death were determined as an absence for 23 weeks [14], in accordance with the friction cost method.
Results
Cost per case of severe gastroenteritis
The number of GP visits, with a mean of two visits, preceding or following the hospitalization was similar for children and adults (Table 2). On average, the patients had visited their GP 0.9 times before they were admitted to a hospital. The visits in the evenings or weekends were mostly before admission. The outpatient clinic was mostly visited after discharge from the hospital. The length of the initial stay in the hospital was, on average, 2.6 days for children, and 6% of the children were rehospitalized with a subsequent stay of 3.7 days, which leads to an overall mean of 2.9 days of hospitalization. For adults, the initial length of hospitalization was 8.7 days, and 15% was readmitted for an average stay of 14.5 days, leading to an overall mean stay of 10.8 days. One adult was referred to a nursing home for 60 days after discharge from the hospital. A considerable number of adults (39%) were transported to the hospital by ambulance, whereas this was rare in children (1%). Parents were, on average, more than three days absent from work to having to take care of their sick child. In adult patients, the absence from work was for 80% the patient themselves, but only a quarter of the adult cases worked. Finally, one adult with Clostridium difficile died due to the complications of the gastroenteritis. The total costs were three times higher in the adults compared to the children; for the direct medical costs, this was actually four times higher. In adults, the highest costs were direct health care costs (81%), followed by indirect costs (15%). In children, the difference between these two cost components was smaller, with values of 62% and 37%, respectively.
Economic burden of gastroenteritis in the Netherlands
The hospitalization rate of gastroenteritis in the NMR registry in 1999 was estimated at 1.2%, 0.1%, and 0.5% for the age groups 0–4 years, 5–17 years, and 18 years and older, respectively [10]. The hospitalization rates of gastroenteritis for these age groups in the GEops study in 2008/2009 were estimated at 1.3%, 0.2%, and 0.01–0.1%, respectively [11, 12]. As the incidence of severe gastroenteritis in adults was difficult to estimate and very likely underestimated [12], the highest estimate of 0.1% was used for the cost calculations. In 2009, an estimated 4.6 million episodes of gastroenteritis occurred; 18% of these episodes were in children younger than 5 years of age, 19% in the older children, and 64% in adults. The average costs per case in 2009 are presented in Table 3. Costs for hospital admissions were comparable within the age group 5–17 years, but were lower for both the other age groups when using the GEops study results compared to the NMR registry data. Overall, gastroenteritis in adults showed the highest financial burden, with €148–174 per case, followed by €126 per case for the age group 5–17 years and €83–95 per case for children aged 0–4 years. Absence from paid employment was the main cost component for all three age groups. The overall costs of gastroenteritis in the Netherlands in 2009 were estimated at €610.7–694.8 million, which is, on average, €133–151 per community case or €37–42 per inhabitant.
Rotavirus was, for 60% of the hospitalizations, the most important pathogen in children hospitalized with gastroenteritis [11]. Based upon the Sensor and the GEops studies, we assumed that 60% of the hospital admission costs and 17% of the other costs in the age group 0–4 years is caused by rotavirus, and 22% and 3% of the costs, respectively, in the adults [8, 11, 12]. In the age group 5–17 years, the impact of the costs for rotavirus was negligible. This resulted in costs due to a rotavirus infection of €16.9 million, of which €7.6 million were hospital costs, for the age group 0–4 years, and €16.6 million, of which €4.2 million were hospital costs, in adults (persons older than 17 years of age).
Discussion
Costs for severe gastroenteritis in 2009 were estimated at €2,203 per hospitalized child and €6,834 per hospitalized adult. The higher cost for adults are explained by the longer stay in the hospital and more frequent visits to the outpatient clinic because of common underlying diseases and more common presentation with serious symptoms and complications [12]. Children were mostly hospitalized because of dehydration [11]. Furthermore, children often recovered quicker than adults. In children with gastroenteritis requiring hospitalization, a relatively large part (37%) of the costs was due to absence from work by their parents. The costs due to absence from work was lower in adults with gastroenteritis requiring hospitalization, because only 25% of these cases worked. In the total costs of all gastroenteritis, absence from work was the largest component, especially in adults. This is in line with other studies: the largest part of the costs is attributable to productivity losses, both for cases and for care-givers [15, 16].
The total cost of gastroenteritis in the Netherlands in 2009 was estimated at €611–695 million. In 1999, these costs were estimated at €345 million, which would correspond with €426 million when corrected for inflation over these 10 years. This means that the costs in this 10-year period have increased by at least 43%, mainly due to the rise in health care costs. For example, the costs of a GP visit and one day of hospitalization increased by 69% and 94%, respectively, between 1999 [10] and 2009 [14]. The total health care expenses in the Netherlands increased between 1999 and 2008 by 84%, of which 40% and 44% were caused by an increase in the use of health care facilities and a rise in prices, respectively [17, 18].
Interestingly, the number of hospital days for children younger than 5 years in 1999 (NMR data) was estimated at 5 days, whereas the GEops study in 2009 estimated a mean admission period of 2.9 days. In adults, the length of hospitalization was 14 days in 1999 and 10.9 days in 2009. This reflects the general trend of limiting the duration of hospital stay for patients [19]. Furthermore, the NMR data gave a hospitalization rate of 0.5% for adults compared to 0.13% based upon the GEops study. The differences between the GEops and NMR data will, at least partly, be caused by different definitions of gastroenteritis. The ICD codes for gastroenteritis used in the NMR are rather non-specific, and, thus, will include non-infectious gastroenteritis. The GEops study was specifically aimed at infectious gastroenteritis, but was based upon the enrolment of cases in six hospitals, which, in theory, is prone to selection bias and incomplete recruitment. When assuming that the incidence for adults as estimated in the GEops study was an underestimation and the incidence based upon the NMR data was an overestimation, the real costs of gastroenteritis in adults would have been between €434 million and €509 million in 2009. Furthermore, it should be noticed that, for the calculation of the total number of community cases in 2009, the gastroenteritis incidence rates from the community study of 1999 were used and applied to the 2009 population. Because of trends in underlying pathogens (for instance, the increase of laboratory-based surveillance for norovirus), the overall estimates might not perfectly reflect the true current situation. However, as no updated overall estimates of gastroenteritis at the community level were available, the previous ones were used as the best proxy.
The vaccination of infants against rotavirus is not part of the National Immunization Programme in the Netherlands. A cost-effectiveness analysis of such a vaccination was conducted over the years 1996–2007 and concluded that implementing the vaccination would not be cost-effective [6]. The estimated costs for rotavirus were, in an unvaccinated Dutch population, estimated to be €25 million per year, of which €7.5 million were hospital-related. In the present study, the corresponding costs were €33.6 million and €11.8 million, respectively. Although these are higher than the figures reported in the cost-effectiveness study, they are within the reported 95% percentile (€12–39 million [6]). According to the sensitivity analysis presented in the cost-effectiveness study, the vaccination strategy could be cost-effective if there would be a substantial herd immunity effect. A herd immunity effect entails that there is less transmission of the virus due to the vaccination in young children, which, in turn, also protects non-vaccinated (older) individuals. The costs for rotavirus are equally as large as those for small children in the present calculations, mainly due to longer hospitalization in adults. A reduced transmission of the virus could possibly lower the burden of disease and the costs in the older age groups.
In the GEops study, medication use was included in the questionnaire, but was hardly reported. Even in the hospital, the use of antibiotics or similar treatment was limited, and medication costs are included in the cost for one treatment day in the hospital. Alternative treatment was not inquired, as it was hardly reported in the previous community-based study. In both the present study as in the study of 1999, non-specified over-the-counter medication and direct out-of-pocket expenses were disregarded.
Estimations of the costs of gastroenteritis are scarcely found in the literature. Furthermore, comparison of the costs of gastroenteritis between countries is often difficult, as costs for health care facilities differ widely, various costs are included, and different methods are used. In Canada, the costs were estimated to be between €186–208 per inhabitant [15, 16], which is higher than the estimate of €37–42 per inhabitant in the Netherlands. The main difference was the estimated number of episodes of gastroenteritis per person-year, namely, 1.3 episodes in Canada (based on retrospective surveys) versus 0.3 episodes in the Netherlands.
In conclusion, gastroenteritis is associated with a considerable burden of disease in the Netherlands and considerable costs. The total health care costs for gastroenteritis requiring hospitalization are three times higher per adult case compared to a child, mainly due to differences in the clinical presentation at hospitalization and the course of disease. Overall, the economic burden of gastroenteritis in the Netherlands has increased by about 50% in a 10-year period up to over €600 million annually, mostly due to the increasing costs of health care.
References
Ahs JW, Tao W, Löfgren J, Forsberg BC (2010) Diarrheal diseases in low- and middle-income countries: incidence, prevention and management. Open Infect Dis J 4:113–124
McCormack PL, Keam SJ (2009) Rotavirus vaccine RIX4414 (Rotarix): a review of its use in the prevention of rotavirus gastroenteritis. Paediatr Drugs 11:75–88
Plosker GL (2010) Pentavalent rotavirus vaccine (RotaTeq): A review of its use in the prevention of rotavirus gastroenteritis in Europe. Drugs 70:1165–1188
Desselberger U, Wolleswinkel-van den Bosch J, Mrukowicz J, Rodrigo C, Giaquinto C, Vesikari T (2006) Rotavirus types in Europe and their significance for vaccination. Pediatr Infect Dis J 25:S30–S41
Anderson EJ, Weber SG (2004) Rotavirus infection in adults. Lancet Infect Dis 4:91–99
Mangen MJ, van Duynhoven YT, Vennema H, van Pelt W, Havelaar AH, de Melker HE (2010) Is it cost-effective to introduce rotavirus vaccination in the Dutch national immunization program? Vaccine 28:2624–2635
Zomer TP, van Duynhoven YTHP, Mangen MJJ, van der Maas NAT, Vennema H, Boot H, de Melker HE (2008) Assessing the introduction of universal rotavirus vaccination in the Netherlands. Vaccine 26:3757–3764
de Wit MA, Koopmans MP, Kortbeek LM, Wannet WJ, Vinjé J, van Leusden F, Bartelds AI, van Duynhoven YT (2001) Sensor, a population-based cohort study on gastroenteritis in the Netherlands: incidence and etiology. Am J Epidemiol 154:666–674
de Wit MA, Kortbeek LM, Koopmans MP, de Jager CJ, Wannet WJ, Bartelds AI, van Duynhoven YT (2001) A comparison of gastroenteritis in a general practice-based study and a community-based study. Epidemiol Infect 127:389–397
van den Brandhof WE, De Wit GA, de Wit MA, van Duynhoven YT (2004) Costs of gastroenteritis in The Netherlands. Epidemiol Infect 132:211–221
Friesema IH, de Boer RF, Duizer E, Kortbeek LM, Notermans DW, Norbruis OF, Bezemer DD, van Heerbeek H, van Andel RN, van Enk JG, Fraaij PL, Koopmans MP, Kooistra-Smid AM, van Duynhoven YT (2011) Etiology of acute gastroenteritis in children requiring hospitalization in the Netherlands. Eur J Clin Microbiol Infect Dis. doi:10.1007/s10096-011-1320-0
Friesema IHM, de Boer RF, Duizer E, Kortbeek LM, Notermans DW, Smeulders A, Bogerman J, Pronk MJH, Uil JJ, Brinkman K, Koopmans MPG, Kooistra-Smid AMD, van Duynhoven YTHP; on behalf of the GEops Working Group (2011) Aetiology of acute gastroenteritis in adults requiring hospitalization in the Netherlands. Epidemiol Infect. doi:10.1017/S0950268811002652
de Wit MA, Koopmans MP, Kortbeek LM, van Leeuwen NJ, Bartelds AI, van Duynhoven YT (2001) Gastroenteritis in sentinel general practices, The Netherlands. Emerg Infect Dis 7:82–91
Hakkart-van Roijen L, Tan SS, Bouwmans CAM (2011) Handleiding voor kostenonderzoek. Methoden en standaard kostprijzen voor economische evaluaties in de gezondheidszorg. Geactualiseerde versie 2010 [Guidelines for cost research, methods and guideline prices for economic evaluations in health care. Actualized version 2010]. College voor Zorgverzekeringen, Diemen, The Netherlands
Henson SJ, Majowicz SE, Masakure O, Sockett PN, MacDougall L, Edge VL, Thomas MK, Fyfe M, Kovacs SJ, Jones AQ (2008) Estimation of the costs of acute gastrointestinal illness in British Columbia, Canada. Int J Food Microbiol 127:43–52
Majowicz SE, McNab WB, Sockett P, Henson TS, Doré K, Edge VL, Buffett MC, Fazil A, Read S, McEwen S, Stacey D, Wilson JB (2006) Burden and cost of gastroenteritis in a Canadian community. J Food Prot 69:651–659
Statistics Netherlands StatLine (2011) Care accounts; expenditure (in current and constant prices) and financing. http://statline.cbs.nl/statweb/. Accessed 26 January 2011
Statistics-Netherlands (2009) Gezondheid en zorg in cijfers 2009 [Health and care in figures 2009]. Centraal Bureau voor de Statistiek, Den Haag/Heerlen, the Netherlands
van Pelt W, Friesema I, Doorduyn Y, de Jager C, van Duynhoven Y (2009) Trends in Gastro-enteritis in Nederland. Notitie met betrekking tot 2007 [Trends in gastro-enteritis in the Netherlands. Report with regard to 2007]. RIVM, Bilthoven, the Netherlands
Acknowledgment
The authors would like to thank the staff of the hospitals for the inclusion of the patients in the present study. We are grateful to Carolien de Jager for her assistance in the preparation and during the execution of the study.
This study was financed by the Ministry of Public Health, the Netherlands.
Conflicts of interest
None declared.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
This work was completed on behalf of the GEops Working Group. Additional members of the GEops Working Group are: Erwin Duizer, Laetitia M. Kortbeek, Daan W. Notermans, Marion P.G. Koopmans, Richard F de Boer, A. Mirjam D. Kooistra-Smid, Obbe F. Norbruis, Desirée D.L. Bezemer, Annika Smeulders, Pieter L.A. Fraaij, Jolanda Bogerman, Hanneke van Heerbeek, Marjolijn J.H. Pronk, J. Gert van Enk, Jan J. Uil, Robert N.J. van Andel, Kees Brinkman.
Rights and permissions
About this article
Cite this article
Friesema, I.H.M., Lugnér, A.K., van Duynhoven, Y.T.H.P. et al. Costs of gastroenteritis in the Netherlands, with special attention for severe cases. Eur J Clin Microbiol Infect Dis 31, 1895–1900 (2012). https://doi.org/10.1007/s10096-011-1518-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-011-1518-1