
Abstract
Infections with dermatophytes are more prevalent in the elderly than in non-elderly adults; risk factors include local trophic disturbances, underlying diseases such as diabetes and a reduced oxygen supply due to diminished blood circulation. Vaginal mycoses are seldom found. In systemic yeast infections in patients of advanced age, Candida glabrata plays a relatively important role. The dimorphic fungus Coccidioides immitis is more prevalent in the elderly in endemic areas. Although there is no higher susceptibility to moulds in this age group, there are certain situations increasing the risk. The manifestations and symptoms of infection often differ from those of younger patients, which may hamper diagnosis. Deficits in organ function may influence the antifungal drug therapy. Preventive measures such as altering the social environment, avoiding malnutrition, as well as efforts to retard immunosenescence and to improve hygiene are important.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Problem
The elderly population has been steadily growing in developed countries over the past few decades. There are several factors which contribute to the increased susceptibility to certain infections in the elderly (over 60 years of age) and very elderly (over 85 years of age) populations (Table 1). Biological changes and co-morbidities associated with advanced age may adversely affect the immunological response to infection. Especially in the frail, these factors may aggravate the course of the infectious disease. Infections in the elderly are not only more prevalent, but are also associated with higher morbidity and mortality. Moreover, the manifestations and symptoms of infection in the elderly are often different from those of non-elderly adults, which make diagnosis more difficult. For example, non-specific symptoms of infections such as fever may be absent or lessened [1, 2].
These general considerations, plus additional unique features, also apply in the case of fungal infections. In addition to the general increased susceptibility of the elderly, the development of mycoses is also affected by particular attributes of the various pathogens, the potential sites of infection, as well as host factors. The social situation, for example, long-term care settings and nursing homes, also plays a critical role [3].
Localised, cutaneous infections
There are at least two processes which contribute to aging of the skin: the intrinsic and extrinsic aging processes. The intrinsic process refers to natural aging, whereas the extrinsic aging process is due to damage from ultraviolet light irradiation, as well as mechanical and inflammatory irritation [4]. A loss of cell density and other structural components such as elastin fibres and water content reduce the thickness of aging skin, even though the proportion of fat tissue may increase in general. As a consequence, the barrier function of the skin may be impaired [5]. Dry skin, which leads to an increased vulnerability of the skin and impairment of local innate and non-specific resistance mechanisms, occurs as a result of the reduced function of sebaceous and sweat glands [4]. The characteristic pale appearance of aged skin is caused by a hampered vascular supply. Clinically relevant impairment of vascular supply, such as that caused by diabetes, interrupts essential elements of the immune system, including the recruitment and function of platelets, leukocytes, monocytes and lymphocytes, as well as humoral components such as fibrinogen, complement and antibodies [6, 7]. These alterations may not only result in a greater vulnerability but also in a compromise in the skin’s ability to repair itself. Wound healing is impaired.
In the elderly population, there is an increased prevalence of infection of the skin and nails by fungi, dermatophytes, as well as yeasts [8, 9]. Onychomycosis is especially common in the elderly [10]. It has been estimated that up to 60% of people over 65 years of age have dystrophic nails due to a fungal infection or concomitant with a fungal infection; toenails are three times more likely to be affected than fingernails, with no gender differences [11]. Angiopathy, peripheral neuropathy from diabetes and a decreased growth rate of nails contribute to the increased susceptibility of the elderly to fungal infection of the nails [11, 12]. Poor vision and arthralgia, and in some cases physical disability, make it difficult for the elderly to cut the thickened, infected toenails themselves [10]. Since intervention tends to be delayed, the fungal infection is more likely to progress, so that advanced stages of infection are often observed in elderly patients. In such cases, there is an increased risk of transmission of the pathogens to other nails. In particular, infected fingernails can serve as sources for satellite depositions on distant sites of the skin.
The skin in the vicinity of infected nails is also often infected by fungi. When skin in the interdigital areas is macerated concurrent with neglected hygiene, dermatophytes, predominantly Trichophyton rubrum residing in the nails, may spread to the skin. Intertriginous candidosis is also common in the elderly. Seebacher et al. [13] reported that 31% of 187 nursing home inhabitants between 65 and 98 years of age had a culture-proven Candida infection. Such an intertrigo may serve as a portal of entry of other pathogens, which may complicate the course of the fungal infection. Tinea pedis is one of the most important risk factors for erysipelas of the lower legs [14–16]. An intertriginous fungal infection of the foot extending to the sole causes squamous and hyperkeratotic dermatosis [17]. The moccasin pattern is most commonly caused by Trichophyton rubrum and represents a mildly erythematous, scaly, pruritic infection of one or both plantar surfaces [18]. Another pattern is inflammatory, mainly due to Trichophyton mentagrophytes. Finally, the ulcerative pattern of infection is most often seen in elderly patients with additional predisposing factors, such as diabetes [18].
Candida infections of the vulva rather than the vagina are common in elderly women [19]. Candidal superinfections of the skin can also cause skin ulcers of the lower legs in the elderly [18]. Infected pressure ulcers are of particular concern. Areas of necrosis due to the compression of soft tissue between bony prominences and external surfaces which lead to aggravated disturbances in the blood circulation and lymph drainage will occur, especially when those situations may persist for a long time. Inevitably, this may result in tissue damage presenting either as relatively minor lesions of the surface or even as massive necrosis involving deep tissues. Yeasts, in conjunction with aerobic and anaerobic bacteria, may colonise such wounds and induce further damage. From these wounds, micro-organisms may spread to other sites. In particular, decubitus ulcers most commonly affect the sacrum or hips in elderly patients, especially in diabetic patients and those with impaired motility [20], and may represent the source for vaginal or vulval colonisation or even disseminated disease with Candida spp. [21]. Candida albicans ranks among the ten most common pathogens in surgical site infections. Obviously, in the elderly, there are several risk factors predisposing such infections [22, 23].
The prevalence of lipophilic yeasts such as Malassezia furfur is rather high in young persons, an age group for which superficial infections are very commonly diagnosed. In the elderly, when the activity of the sebaceous glands decreases, the number of colonising yeasts decrease concomitantly. Hence, Pityriasis versicolor less frequently affects older individuals [4, 24].
Localised infections of mucous membranes
Sinusitis
After the inhalation of spores, fungal balls can develop in the nasal sinuses, predominantly in the sphenoid sinuses, particularly in elderly people [25]. Although, in general, these fungal masses do not cause overt symptoms, their surgical removal by transnasal endoscopic sphenoidectomy is recommended because of the risk of pathogens penetrating into tissue and triggering an invasive fungal infection, resulting in ophthalmoplegia, ptosis and visual abnormalities. This is caused because of the connections between sphenoidal sinuses and adjacent anatomical structures, such as the cavernous sinus, internal carotis, optic nerve and brain.
Oropharyngeal infections
Saliva rinses micro-organisms out of the oral cavity. In addition, it contains several proteins, such as lysozyme, and oligopeptides which regulate the balance among microbial flora. The most important risk factor for oral candidiasis in the elderly may be associated with hyposalivation. Compared with the controls, individuals with hyposalivation tend to harbour a lower number and proportion of anaerobic Fusobacterium nucleatum on the tongue and, conversely, an increased number of enterococci in the vestibular region.
In the supragingival plaques of teeth, the numbers of Streptococcus mutans and Lactobacillus spp. are significantly increased, while the number of C. albicans also tends to be higher [26]. Candida spp. are also often associated with root caries, particularly in elderly people over 70 years of age [27].
Yeasts easily colonise the gingival mucosa. For users of dental devices, which become a reservoir that favours their reproduction, the incidence is much higher [27]. Consequently, in people with advanced age, the frequency of oral colonisation with Candida spp., especially C. albicans, is definitely increased [27]. One reason for this is poor denture hygiene [28]. Ill-fitting dental prostheses may irritate the gingival mucosa, resulting in a vulnerable site where yeasts easily grow. Further conditions are poor oral hygiene, the use of antibiotics and, in particular, treatment with cytostatic agents [27, 29].
Oral thrush begins with punctual white coatings on the tongue, the soft and hard palate, buccal mucosa or the gingival mucosa. These lesions may become confluent, spreading and inducing large, reddened areas with a white coating. Since the inflamed mucosa is highly vulnerable, bleeding may occur once the film is removed mechanically. The patient complains of paresthesias rather than pain.
Besides denture stomatitis and thrush, Candida may also induce and aggravate angular cheilitis (perlèches) [30], which is often seen in aged people, complicating anaemia and iron loss.
Bronchial tract
It is quite natural that yeasts are carried to the bronchial tract when a high fungal load exists in the oral cavity. Although in such a situation yeasts are commonly found in sputum, a yeast bronchitis or even pneumonia is quite uncommon in immunocompetent individuals; such a mere colonisation does not require an antifungal therapy [31]. Only occasionally, for example, in leukopaenic individuals, is there a concern that yeasts may penetrate into the mucosa or expand into the lower respiratory tract and induce an inflammatory reaction there.
Mould infections are acquired primarily by inhalation. Hence, in some cases, a local colonisation of the bronchial tract may be followed by an invasion into the mucosal layer, in particular when a local lesion has developed, for example, after device-assisted ventilation over a long period. However, localised infections only generally occur in severely compromised patients (for example, with neutropenia <500/µl).
Intestinal infections
In the gastrointestinal tract of the elderly, physiological changes include decreased acid secretion by the gastric mucosa, which facilitates the passage of microbes. In consequence, certain microbes, including yeasts, can take advantage of new ecological niches, leading to a shift in the composition of gut flora upon age [32]. Since the bowel content of non-digested foodstuffs may influence the growth of Candida in the gut lumen, as shown in animal experiments [33], an overgrowth might be the consequence of the partial lack of digestive enzymes in the gut, lending to plenty of nutrients available for yeasts in the colon. The increase of Candida cells may still be promoted when antibiotics are given, which will alter the physiological, competitive bacterial gut flora [34]. Such collateral damage is particularly seen when a patient receives broadspectrum antibiotics (including ceftriaxone or ciprofloxacin), which will be eliminated predominantly via the intestinal tract. However, such an overgrowth of yeasts is not a disease in itself, but, rather, a consequence of other pathological alterations. Consequently, the correct reasons have to be attacked therapeutically; treatment with antifungal agents will help transiently at best. In contrast, elevated numbers of yeasts in the colon may have beneficial, i.e. probiotic, effects. For example, the binding capacity of mannans in the surface layer of yeast cells may help neutralise enteropathogenic bacteria such as Escherichia coli, as well as certain bacterial and fungal toxins [35–38]. Indeed, it is a common clinical practice to treat such patients, especially those suffering with Clostridium difficile-associated diarrhoea, with probiotics such as living yeasts (for example, Saccharomyces cerevisiae, sometimes erroneously named as Saccharomyces boulardii) [39]. Although probiotics are considered to be safe, their use in particular groups of patients should be carefully deliberated [40]. Indeed, even Saccharomyces may result in a fungaemia in debilitated aged individuals [41].
Vaginitis/vulvitis
The vaginal environment changes dramatically with the withdrawal of oestrogen. Along with physical and chemical changes in the vagina during aging, an overall decrease in the normal Lactobacillus-dominant flora occurs. The incidence of vaginal colonisation with Candida spp. in post-menopausal woman is even higher than in controls [21]. C. glabrata is by far the most common species isolated [21]. The warm and moist environment in the perineal area created by diaper use in incontinent individuals, together with decubitus ulcers and immobilisation common in elderly patients receiving long-term care, are other factors responsible for the high occurrence of vaginal colonisation with Candida in this group.
In post-menopausal females, C. albicans adherence to vaginal epithelial cells is, however, lower than for their fecund controls [42]. Furthermore, it has to be kept in mind that C. albicans possesses an oestrogen receptor [43] and its stimulation increases the virulence of the fungi [44]. Thus, vulvovaginal candidiasis still occurs in menopausal women, but less commonly than in younger women [45]. In particular, recurrent vaginal candidiasis is uncommon but may develop, especially in women following a hysterectomy [19].
Whereas vaginal mycosis is a disease of pre-menopausal women, vulval mycosis is a problem in post-menopausal women [19]. Erythematous patches with satellite pustules accompanied by pruritus are often misdiagnosed when no cultural examination has been undertaken [46].
Balanitis
Age is not a risk factor for candidal balanitis, but men found to have diabetes mellitus are more susceptible. Hence, in this group, the portion of older people was significantly higher [47]. By the way, Candida infection of the glans penis is more commonly seen in uncircumcised men.
Invasive fungal infections
Nosocomial infections are generally more common in older people [48]. This is not only because of an increased hospitalisation rate, but due to the increased risk of infection per day of hospitalisation [49]. This also applies to invasive mycoses, especially Candida infections, which are a particular problem in hospital settings [50].
Indeed, several immune defence mechanisms may be impaired in old age. Whereas the number of cells of the innate immune system (granulocytes, macrophages and natural killer cells) and the adaptive immune system (T-cells and B-cells) are not decreased, their functional capacities such as phagocytosis, killing of micro-organisms and production of and response to certain cytokines may be impaired. Hence, immunosenescence results in populating immune tissues with less functional T-cells (and perhaps B-cells and dendritic cells). These poorly functioning cells produce more type 2 cytokines and fewer type 1, leading to a decreased Th1 response and an increased Th2 response, which impacts on the defence against various micro-organisms, including fungi. The problem is that, in an individual patient, the progress of immunosenescence is difficult to define. Impaired immunity, distinct from immunosenescence, correlates more with infectious disease than chronologic age [51]. One remarkable reason for dysfunction of the immune system besides immunosenescence, and possibly more important for increased susceptibility to infectious diseases in general, is malnutrition [52, 53]. Many elderly people suffer a deficiency of protein, which leads to a loss of skeletal muscle, and of essential elements such as zinc and selenium. Furthermore, malnutrition is not only a major risk factor for infection. Alongside infection, the metabolic demand is increased and this, in turn, aggravates malnutrition. Whereas in developing countries malnutrition affects primarily children, in industrialised nations, this problem is especially relevant in a geriatric context because of a lack of nutritional reserves.
Not all aged individuals are overtly immunosuppressed, meaning that advanced age is not a risk factor for invasive fungal infections in itself. For example, invasive fungal infections are rather uncommon in community settings. On the other hand, it is quite conceivable that debilitating diseases arising progressively with growing age result in frequent hospital stays. Along with compromised defence systems, this may be a reason for why both aspergillosis and candidiasis—the most relevant invasive fungal infections—are predominant in aged people [54]. Laupland et al. [55] reported in a five-year retrospective study in Canada, that the elderly (and the very young) were at the highest risk for invasive Candida infections. Lin et al. [56] stated that elderly patients (over 80 years of age) with B-cell lymphoma suffer more frequently from fungal infections than younger patients. Older age is a definite risk factor for candidaemia [57, 58]. Overall, mortality attributable to systemic Candida infection is rather high and appears to be higher in the elderly population [59]. This increased risk of infection is a direct consequence of the higher prevalence of colonisation with Candida spp. in aged people [29].
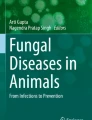
Figure 1 shows that C. glabrata fungaemia is more often seen in older patients (over 60 years of age) [60–62] and is associated with a higher mortality rate [63], which is possibly due to a lower susceptibility to azole antifungals.

Age-dependant increase of the prevalence of C. glabrata and of fluconazole-resistant C. glabrata in candidaemia (according to [58])
Urinary tract infection with Candida spp. is often suspected because fungi are frequently detected in urine. There are, however, no solid criteria to differentiate between mere colonisation and genuine urinary tract infection [46, 64, 65]. Most senior patients with candiduria are asymptomatic. However, when complaints such as fever, flank pain, nausea and vomiting are reported—problems associated with bacterial pyelonephritis—an antifungal therapy is required. In exceptional cases, a fungal ball comprised of a network of fungal hyphae may obstruct the urinary tract and may serve as a source for dissemination. The most common yeast isolated from urine is C. albicans, whereas in young children, C. parapsilosis is found more often [61, 64, 65].
Cryptococcosis, although a rare event, may occur more frequently in older persons. Furthermore, atypical manifestations such as pulmonary infections are found more often than in their younger counterparts. Furthermore, mortality is higher in the aged population [46].
Endemic fungal infections, for example, with Coccidioides immitis, a dimorphic fungus, play an increasing role in certain countries (for example, in the south-western states of the USA). Older age groups (over 65 years of age) are more often hospitalised because of this fungal infection [66, 67]. Whereas in non-immunocompromised patients these infections remain mostly asymptomatic, in immunocompromised subjects, namely AIDS patients and organ transplant recipients, these infections often result in severe diseases affecting the lungs and various other organs, such as skin, bone, central nervous system (CNS) and prostate. It has been suggested that the increased susceptibility of older people to this opportunistic fungus is a consequence of immunosenescence, in particular of the cellular immune system, which is primarily involved in the defence against C. immitis [68]. In contrast, blastomycosis, a rare but important fungal infection in south central and mid-western USA as well as South America, affects all ages equally [69].
Fulminant pulmonary aspergillosis may occur in aged individuals treated with a short-term regimen of corticosteroids because of underlying chronic lung disease [70]. The higher vulnerability of aged subjects could also be confirmed in animal experiments [71]. Old rats challenged with an inflammatory component were less able to produce IL-10 and, consequently, developed an exceedingly inflammatory reaction, leading to severe lung damage.
Diagnostic and antifungal therapy in the elderly
In principle, the same diagnostic tools are valid for the diagnosis of fungal infections of persons with advanced age as of younger people.
As stated already, the clinical symptoms of infections in the elderly may be present in atypical and non-classical fashions and are, thus, misleading. Furthermore, non-specific signs, for example, fever (the cardinal sign of infection), may be absent or blunted in a considerable number of elderly patients [72]. The interpretation of C-reactive protein (CRP) levels in aged people is hampered by the fact that various factors besides inflammation may contribute to increased serum levels [73]. Similarly, other products of macrophages and leukocytes, such as IL-6, TNF and YKL-40, may be elevated in the serum of aged people. But these findings suggest that they might serve as prognostic and sensitive biomarkers for all problems and not exclusively infections or even fungal infections [74].
Hence, a microbiological proof is urgently needed. Since the detection of serum antibodies is of relatively low importance in the diagnosis of fungal infections, the cultural proof is of utmost importance. A particular aspect is the preponderance of certain fungal strains being more resistant to antifungals in aged patients. C. glabrata, for example, is relatively frequently found to be so (Fig. 1) [60, 62, 63].
The basic principles of therapy are the same irrespective of age. However, there are some peculiarities in aged people which influence the pharmacology of antifungals. Age-related changes in the functions and composition of the human body require adjustments of drug selection and dosage for older individuals. Unfortunately, little data on this issue are available, since very few elderly patients are enrolled in clinical trials and few clinical trials are designed specifically for this population.
The bioavailability of orally-applied drugs is dependent on the chemical composition of the drug and also on the activities of the intestinal tract [75]. In fact, the absorption of actively transported substances may be diminished in the elderly. However, most drugs are absorbed by passive diffusion, meaning that the general intestinal absorption of most drugs is not altered in the elderly [76]. The gastrointestinal absorption of the lipophilic drug itraconazole is highly variable in young adults already (for example, absorption can be improved when taken with acid beverages such as Coca-Cola). The major site of itraconazole absorption is possibly the proximal segment of the duodenum, where a relatively low pH still exists, allowing itraconazole to be dissolved [77]. Since seniors often show a lack of gastric acid, the bioavailability of itraconazole might be reduced. Hence, elderly people should prefer the oral liquid solution (cyclodextrin), which is more avidly taken up. In all cases, a therapeutic drug monitoring is recommended.
Aging is associated with definite changes in body composition (for example, the loss of skeletal muscle leading to sarcopaenia and gains in visceral fat content). The water distribution volume also decreases with age. Hence, the distribution volume of hydrophilic compounds is reduced in the elderly, whereas that of lipophilic drugs is increased [76]. This may lead to altered serum levels as well as to altered half-lives of special drugs [78], which also endorses therapeutic drug monitoring. When considering the volume of distribution, it is important to remember that elderly people may have significantly reduced body weight, which may suggest a risk factor for overmedication [78].
Furthermore, the metabolism of various compounds in the liver changes with advancing years because the activity of the enzymes involved, such cytochrome P450, diminishes with age. This is one cause of the higher levels of voriconazole found in elderly patients [79]. Over- or underexposure of voriconazole may have clinical implications. High serum levels of voriconazole are correlated with adverse neurological effects, such as hallucinations [80]. In contrast, posaconazole (another triazole) given over several months for the treatment of coccidioidomycoses, although not a good substrate for cytochrome P450, was well tolerated [81]. Itraconazole should be used with caution in patients with a history of liver impairment [78]. However, the pharmacokinetics of echinocandins, which are not metabolised by liver enzymes, is independent of age [82, 83]. Indeed, caspofungin was well tolerated in older patients [84].
Kidney function may also be affected. A reduction of the glomerular filtration rate is observed with increasing age, leading to a reduced creatinine clearance. Drug excretion via the kidneys declines with age, meaning that the elderly should be treated as renally insufficient patients [76]. The serum concentrations of electrolytes may be critical, so, often, a hyperosmolarity, in particular, a hyperkalaemia, is more common [85, 86]. This delicate balance may be easily impeded by drugs, in particular, amphotericin B. In addition, therapeutic target concentrations of drugs are hard to define because of marked variations in the elderly population.
Furthermore, elderly people take more drugs because of various co-morbidities, possibly interacting with antifungals and modifying serum drug concentrations and their toxicities. Indeed, polypharmacy is a common problem in the elderly [78]. For example, both voriconazole and fluconazole interfere with the hepatic degradation of antidepressants, such as diazepam [87], which are common therapeutics in the elderly. This also means that therapeutic drug monitoring should be considered in such cases. Adverse reactions to drugs are more severe and frequent in the elderly, who are also less likely to report them [75, 76].
A particular problem, especially in home health care, is compliance with prescribed drugs [88]. Intentional or unintentional abuse may occur. Furthermore, understanding how and when doses should be taken may become a problem. Those factors have a powerful influence on the efficiency of an antifungal therapy, as well as on its tolerability.
The various azole derivatives (fluconazole, itraconazole, voriconazole and posaconazole), and especially the echinocandins (caspofungin [84], micafungin and anidulafungin), are best suited for treating invasive fungal infections, as long as the pathogens are susceptible to the agents.
Although candiduria is common among older patients, in most cases, it is a non-specific finding that occurs because of contamination of a urine sample and colonisation of an indwelling catheter and/or the bladder. Most patients are merely colonised and do not require antifungal therapy. Removing predisposing factors, such as indwelling catheters and antibiotics, will clear candiduria in almost 50% of asymptomatic patients. For the few patients with symptomatic Candida urinary tract infections, a variety of treatment options are available. Fluconazole is the antifungal agent of choice, achieving high urine concentrations with the oral formulation. Amphotericin, newer azole agents and echinocandins are not recommended for the treatment of urinary tract infections since they are not eliminated via the kidney and, thus, fail to achieve adequate urine concentrations [46].
Local infections with dermatophytes, yeasts and moulds can be treated either by systemically or locally applied antifungal agents. Since onychomycosis is not self-healing, elderly people—in particular, diabetic patients—should be treated to prevent secondary bacterial infections and subsequent serious complications. Terbinafine is the drug of choice since it has greater cure rates and fewer drug interactions than itraconazole [15]. In general, topical nail lacquers, such as amorolfine and ciclopirox, are not practical for the elderly because of the frequency of daily application over a long duration of time [15]. For the treatment of mucosal infections with yeasts, polyenes such as amphotericin B or nystatin are used because these bulky compounds remain unabsorbed and generate fewer adverse effects.
Several antiseptics also dispose of high antimycotic activities. In aged people, antiseptics with low tissue irritability, such as povidone–iodine, octenidine or polyhexanide, can be used effectively.
Prevention
Doctor awareness of this particular entity should be stronger. It should be known that even a Tinea pedis is not a banal disease but may have serious consequences when it serves as a portal of entry for menacing pathogens such as hemolytic streptococci inducing erysipelas [14, 16]. In hospitals, education of the medical staff is mandatory, since it is well-known that fungal infections may be nosocomial [89].
Early and rational treatment of wounds infected with fungi accompanied by adequate wound care reduces the risk of spreading. Adjunctive measurements such as debridement, wound dressings and negative pressure wound therapy to ameliorate the vascular circulation will further support healing and spreading.
Cleaning hands with alcoholic disinfectants can help avoid the transfer of Candida spp., while care must be taken to avoid transferring Candida infections on toothbrushes and other basic utensils. Anthropophilic dermatophytes can be transmitted by the same vehicles. The infecting organisms thrive in warm, moist environments, such as gymnasium floors, swimming pool decks and carpeted bathrooms. Equally, socks and closed-toe shoes can be contaminated with spores of dermatophytes and may provide the source of re-infection if left untreated. Disinfection of environmental sites, for example, with quaternary ammonium, sodium hypochlorite, chlorine dioxide or peroxides, may also be helpful in certain cases. Antifungal powder in shoes may be an alternative to disinfectants. Wearing protective footwear when in public areas can help to avoid infections with dermatophytes.
Infections of pets, such as guinea pigs, cats and dogs, or farm animals with dermatophytes are rather common and some of these zoophilic pathogens may be transmitted to humans. Wearing gloves during gardening may protect against infections with geophilic dermatophytes.
Patients themselves can achieve an increased resistance to infection with dermatophytes when they take care of their skin integrity, including preventing skin dehydration [4].
Since an oral colonisation with Candida spp. can be a source for a systemic infection when conditions are favourable [28], denture cleanliness is regarded as a proper prevention. Less than 20% of dentures worn by the elderly are properly cleaned. More and better cleaning will reduce the prevalence of Candida spp. [28].
Several philosophies and ideas exist on how to restore youth and minimise immunosenescence. Chin et al. [90] have reported that physical exercise may slow or even help prevent the age-related decline in immune response.
Malnutrition is prevalent in elderly populations. Although recommended nutritional advice is often complicated and contradictory, the survival of frail, very old, hospitalised patients from any kind of disease is significantly lower in malnourished patients and patients at risk of malnutrition than in well-nourished patients [91]. In recent times, the role of probiotics is often discussed [32].
Conclusion
Conclusively, patients and doctors need to pay more attention to this pathologic entity because, as the number of aged people in developed countries continues to increase, so, mycoses in the elderly will become an even more common problem.
References
Gavazzi G, Krause KH (2002) Ageing and infection. Lancet Infect Dis 2:659–666
Htwe TH, Mushtaq A, Robinson SB et al (2007) Infection in the elderly. Infect Dis Clinics North Am 21:711–743
Garibaldi RA (1999) Residential care and the elderly: the burden of infection. J Hosp Infect 43(Suppl):S9–S18
Hornstein OP (2002) Hautkrankheiten und Hautpflege im Alter. Wissenschaftliche Verlagsgesellschaft, Stuttgart
Grove GL (1989) Physiologic changes in older skin. Clin Geriatr Med 5:115–125
Harris NR, Rumbaut RE (2001) Age-related responses of the microcirculation to ischemia-reperfusion and inflammation. Pathophysiology 8:1–10
Castle SC, Uyemura K, Makinodan T (2007) Impaired immunity and increased risk of infections in older adults: impact of chronic disease on immunosenescence. In: Yoshikawa TT, Ouslander JG (eds) Infection management for geriatrics in long-term care facilities, 2nd edn. Informa Healthcare, New York, London, pp 49–70
Yalçin B, Tamer E, Toy GG et al (2006) The prevalence of skin diseases in the elderly: analysis of 4099 geriatric patients. Int J Dermatol 45:672–676
Kılıç A, Gül Ü, Aslan E et al (2008) Dermatological findings in the senior population of nursing homes in Turkey. Arch Gerontol Geriatr 47:93–98
Piérard G (2001) Onychomycosis and other superficial fungal infections of the foot in the elderly: a pan-European survey. Dermatology 202:220–224
Mügge C, Haustein U-F, Nenoff P (2006) Causative agents of onychomycosis—a retrospective study. J Dtsch Dermatol Ges 4:218–228
Seebacher C, Brasch J, Abeck D et al (2007) Onychomycosis. Mycoses 50:321–327
Seebacher C, Abeck D, Brasch J et al (2006) Candidiasis of the skin. J Dtsch Dermatol Ges 4:591–596
Korting HC, Schaller M (2001) New developments in medical mycology. Hautarzt 52:91–97
Loo DS (2007) Onychomycosis in the elderly: drug treatment options. Drugs Aging 24:293–302
Roldan YB, Mata-Essayag S, Hartung C (2000) Erysipelas and tinea pedis. Mycoses 43:181–183
Seebacher C, Korting HC, Abeck D et al (2005) Tinea der freien Haut. J Dtsch Dermatol Ges 3:921–926
Martin ES, Elewski BE (2002) Cutaneous fungal infections in the elderly. Clin Geriatr Med 18:59–75
Ventolini G, Baggish MS (2005) Post-menopausal recurrent vaginal candidiasis: effect of hysterectomy on response to treatment, type of colonization and recurrence rates post-treatment. Maturitas 51:294–298
Klein NC, Cunha BA (2001) Skin and soft tissue infections. In: Yoshikawa TT, Norman DC (eds) Infectious diseases in the aging. Humana, Totowa, NJ, pp 139–145
Dan M, Segal R, Marder V et al (2006) Candida colonization of the vagina in elderly residents of a long-term-care hospital. Eur J Clin Microbiol Infect Dis 25:394–396
Mangram AJ, Horan TC, Pearson ML et al (1999) Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol 20:250–278
Anderson DJ, Kaye KS (2007) Skin and soft tissue infections in older adults. Clin Geriatr Med 23:595–613
Faergemann J, Aly R, Maibach HI (1983) Quantitative variations in distribution of Pityrosporum orbiculare on clinically normal skin. Acta Derm Venereol 63:346–348
Bowman J, Panizza B, Gandhi M (2007) Sphenoid sinus fungal balls. Ann Otol Rhinol Laryngol 116:514–519
Almståhl A, Wikström M (2005) Microflora in oral ecosystems in subjects with hyposalivation due to medicines or of unknown origin. Oral Health Prev Dent 3:67–76
Zaremba ML, Daniluk T, Rozkiewicz D et al (2006) Incidence rate of Candida species in the oral cavity of middle-aged and elderly subjects. Adv Med Sci 51(Suppl 1):233–236
Kanli A, Demirel F, Sezgin Y (2005) Oral candidosis, denture cleanliness and hygiene habits in an elderly population. Aging Clin Exp Res 17:502–507
Fanello S, Bouchara JP, Sauteron M et al (2006) Predictive value of oral colonization by Candida yeasts for the onset of a nosocomial infection in elderly hospitalized patients. J Med Microbiol 55:223–228
Reinel D, Plettenberg A, Seebacher C et al (2004) Oral candidiasis. J Dtsch Dermatol Ges 2:874–876
Wood GC, Mueller EW, Croce MA et al (2006) Candida sp. isolated from bronchoalveolar lavage: clinical significance in critically ill trauma patients. Intensive Care Med 32:599–603
Bartosch S, Woodmansey EJ, Paterson JC et al (2005) Microbiological effects of consuming a synbiotic containing Bifidobacterium bifidum, Bifidobacterium lactis, and oligofructose in elderly persons, determined by real-time polymerase chain reaction and counting of viable bacteria. Clin Infect Dis 40:28–37
Buddington KK, Donahoo JB, Buddington RK (2002) Dietary oligofructose and inulin protect mice from enteric and systemic pathogens and tumor inducers. J Nutr 132:472–477
Samonis G, Gikas A, Toloudis P et al (1994) Prospective study of the impact of broad-spectrum antibiotics on the yeast flora of the human gut. Eur J Clin Microbiol Infect Dis 13:665–667
Gedek BR (1991) Regulierung der Darmflora über die Nahrung. Zentralbl Hyg Umweltmed 191:277–301
Hof H (1995) Pilze im Darm. Was nun? Med Welt 46:219–221
Bueno DJ, Casale CH, Pizzolitto RP et al (2007) Physical adsorption of aflatoxin B1 by lactic acid bacteria and Saccharomyces cerevisiae: a theoretical model. J Food Prot 70:2148–2154
Shetty PH, Hald B, Jespersen L (2007) Surface binding of aflatoxin B1 by Saccharomyces cerevisiae strains with potential decontaminating abilities in indigenous fermented foods. Int J Food Microbiol 113:41–46
Thompson I (2008) Clostridium difficile-associated disease: update and focus on non-antibiotic strategies. Age Ageing 37:14–18
Boyle RJ, Robins-Browne RM, Tang ML (2006) Probiotic use in clinical practice: what are the risks? Am J Clin Nutr 83:1256–1264
Cherifi S, Robberecht J, Miendje Y (2004) Saccharomyces cerevisiae fungemia in an elderly patient with Clostridium difficile colitis. Acta Clin Belg 59:223–224
Segal E, Soroka A, Schechter A (1984) Correlative relationship between adherence of Candida albicans to human vaginal epithelial cells in vitro and candidal vaginitis. Sabouraudia 22:191–200
Zhao X, Malloy PJ, Ardies CM et al (1995) Oestrogen-binding protein in Candida albicans: antibody development and cellular localization by electron immunocytochemistry. Microbiology 141:2685–2692
Zhang X, Essmann M, Burt ET et al (2000) Estrogen effects on Candida albicans: a potential virulence-regulating mechanism. J Infect Dis 181:1441–1446
Nyirjesy P (2007) Postmenopausal vaginitis. Curr Infect Dis Rep 9:480–484
Kauffman CA, Hedderwick SA (2007) Fungal infections. In: Yoshikawa TT, Ouslander JG (eds) Infection management for geriatrics in long-term care facilities, 2nd edn. Informa Healthcare, New York, London, pp 445–464
Waugh MA, Evans EG, Nayyar KC et al (1978) Clotrimazole (Canesten) in the treatment of candidal balanitis in men. With incidental observations on diabetic candidal balanoposthitis. Br J Vener Dis 54:184–186
Ohlsen K, Hacker J (2005) Infections in the elderly. Int J Med Microbiol 294:471–472
Emori TG, Banerjee SN, Culver DH et al (1991) Nosocomial infections in elderly patients in the United States, 1986–1990. National Nosocomial Infections Surveillance System. Am J Med 91:289S–293S
Zilberberg MD, Shorr AF, Kollef MH (2008) Secular trends in candidemia-related hospitalization in the United States, 2000–2005. Infect Control Hosp Epidemiol 29:978–980
Castle SC, Uyemura K, Fulop T et al (2007) Host resistance and immune responses in advanced age. Clin Geriatr Med 23:463–479
Mazari L, Lesourd BM (1998) Nutritional influences on immune response in healthy aged persons. Mech Ageing Dev 104:24–40
de Jong N, Gibson RS, Thomson CD et al (2001) Selenium and zinc status are suboptimal in a sample of older New Zealand women in a community-based study. J Nutr 131:2677–2684
Lamagni TL, Evans BG, Shigematsu M et al (2001) Emerging trends in the epidemiology of invasive mycoses in England and Wales (1990–9). Epidemiol Infect 126:397–414
Laupland KB, Gregson DB, Church DL et al (2005) Invasive Candida species infections: a 5 year population-based assessment. J Antimicrob Chemother 56:532–537
Lin PC, Hsiao LT, Poh SB et al (2007) Higher fungal infection rate in elderly patients (more than 80 years old) suffering from diffuse large B cell lymphoma and treated with rituximab plus CHOP. Ann Hematol 86:95–100
Luzzati R, Amalfitano G, Lazzarini L et al (2000) Nosocomial candidemia in non-neutropenic patients at an Italian tertiary care hospital. Eur J Clin Microbiol Infect Dis 19:602–607
Pfaller MA, Diekema DJ (2007) Epidemiology of invasive candidiasis: a persistent public health problem. Clin Microbiol Rev 20:133–163
Pappas PG, Rex JH, Lee J et al (2003) A prospective observational study of candidemia: epidemiology, therapy, and influences on mortality in hospitalized adult and pediatric patients. Clin Infect Dis 37:634–643
Pfaller MA, Diekema DJ (2002) Role of sentinel surveillance of candidemia: trends in species distribution and antifungal susceptibility. J Clin Microbiol 40:3551–3557
Pfaller MA, Diekema DJ, Jones RN et al (2002) Trends in antifungal susceptibility of Candida spp. isolated from pediatric and adult patients with bloodstream infections: SENTRY Antimicrobial Surveillance Program, 1997 to 2000. J Clin Microbiol 40:852–856
Diekema DJ, Messer SA, Brueggemann AB et al (2002) Epidemiology of candidemia: 3-year results from the emerging infections and the epidemiology of Iowa organisms study. J Clin Microbiol 40:1298–1302
Malani A, Hmoud J, Chiu L et al (2005) Candida glabrata fungemia: experience in a tertiary care center. Clin Infect Dis 41:975–981
Yang YL, Cheng HH, Lo HJ; Tsary Hospitals (2006) Distribution and antifungal susceptibility of Candida species isolated from different age populations in Taiwan. Med Mycol 44:237–242
Malani AN, Kauffman CA (2007) Candida urinary tract infections: treatment options. Expert Rev Anti Infect Ther 5:277–284
Park BJ, Sigel K, Vaz V et al (2005) An epidemic of coccidioidomycosis in Arizona associated with climatic changes, 1998–2001. J Infect Dis 191:1981–1987
Sunenshine RH, Anderson S, Erhart L et al (2007) Public health surveillance for coccidioidomycosis in Arizona. Ann N Y Acad Sci 1111:96–102
Ampel NM (2007) The complex immunology of human coccidioidomycosis. Ann N Y Acad Sci 1111:245–258
Bradsher RW Jr (2008) Pulmonary blastomycosis. Semin Respir Crit Care Med 29:174–181
Cornet M, Mallat H, Somme D et al (2003) Fulminant invasive pulmonary aspergillosis in immunocompetent patients—a two-case report. Clin Microbiol Infect 9:1224–1227
Corsini E, Di Paola R, Viviani B et al (2005) Increased carrageenan-induced acute lung inflammation in old rats. Immunology 115:253–261
Norman DC (2000) Fever in the elderly. Clin Infect Dis 31:148–151
Lind L, Siegbahn A, Hulthe J, Elmgren A (2008) C-reactive protein and e-selectin levels are related to vasodilation in resistance, but not conductance arteries in the elderly: the Prospective Investigation of the Vasculature in Uppsala Seniors (PIVUS) study. Atherosclerosis 199:129–137
Johansen JS, Pedersen AN, Schroll M et al (2008) High serum YKL-40 level in a cohort of octogenarians is associated with increased risk of all-cause mortality. Clin Exp Immunol 151:260–266
Ritz P, Vellas B (2007) Pharmacokinetics and drug toxicity in elderly patients: a case for geriatric core data in clinical trials. J Nutr Health Aging 11:261–264
Turnheim K (2003) When drug therapy gets old: pharmacokinetics and pharmacodynamics in the elderly. Exp Gerontol 38:843–853
Lohitnavy M, Lohitnavy O, Thangkeattiyanon O et al (2005) Reduced oral itraconazole bioavailability by antacid suspension. J Clin Pharm Ther 30:201–206
Flammiger A, Maibach H (2006) Drug dosage in the elderly: dermatological drugs. Drugs Aging 23:203–215
Hope WW, Denning DW (2004) Invasive aspergillosis: current and future challenges in diagnosis and therapy. Clin Microb Infect 10:2–4
Imhof A, Schaer DJ, Schanz U et al (2006) Neurological adverse events to voriconazole: evidence for therapeutic drug monitoring. Swiss Med Wkly 136:739–742
Stevens DA, Rendon A, Gaona-Flores V et al (2007) Posaconazole therapy for chronic refractory coccidioidomycosis. Chest 132:952–958
Dowell JA, Knebel W, Ludden T et al (2004) Population pharmacokinetic analysis of anidulafungin, an echinocandin antifungal. J Clin Pharmacol 44:590–598
Nguyen TH, Hoppe-Tichy T, Geiss HK et al (2007) Factors influencing caspofungin plasma concentrations in patients of a surgical intensive care unit. J Antimicrob Chemother 60:100–106
Dinubile MJ, Strohmaier KM, Lupinacci RJ et al (2008) Efficacy and safety of caspofungin therapy in elderly patients with proven or suspected invasive fungal infections. Eur J Clin Microbiol Infect Dis 27:663–670
Beck LH (2000) The aging kidney. Defending a delicate balance of fluid and electrolytes. Geriatrics 55:26–28, 31–32
Luckey AE, Parsa CJ (2003) Fluid and electrolytes in the aged. Arch Surg 138:1055–1060
Saari TI, Laine K, Bertilsson L et al (2007) Voriconazole and fluconazole increase the exposure to oral diazepam. Eur J Clin Pharmacol 63:941–949
Claesson S, Morrison A, Wertheimer AI et al (1999) Compliance with prescribed drugs: challenges for the elderly population. Pharm World Sci 21:256–259
Fanello S, Bouchara JP, Jousset N et al (2001) Nosocomial Candida albicans acquisition in a geriatric unit: epidemiology and evidence for person-to-person transmission. J Hosp Infect 47:46–52
Chin A, Paw MJ, de Jong N et al (2000) Immunity in frail elderly: a randomized controlled trial of exercise and enriched foods. Med Sci Sports Exerc 32:2005–2011
Kagansky N, Berner Y, Koren-Morag N et al (2005) Poor nutritional habits are predictors of poor outcome in very old hospitalized patients. Am J Clin Nutr 82:784–791
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hof, H. Mycoses in the elderly. Eur J Clin Microbiol Infect Dis 29, 5–13 (2010). https://doi.org/10.1007/s10096-009-0822-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-009-0822-5