
Abstract
Background
Driving is a complex task requiring the integrity and the cooperation of cognition, motor, and somatosensory skills, all of which are impacted by neurological diseases.
Objective
Identification of neurologist’s role when assessing fitness to drive of cognitively impaired individuals.
Methods
We performed a systematic review of the guidelines/recommendations (G/Rs) regarding the evaluation of driving fitness of patients with mild cognitive impairment (MCI) and/or dementia. Emphasis was put on the neurological and neuropsychological aspects of the evaluation.
Results
Eighteen G/Rs were included in the review (9 national guidelines, 5 recommendation papers, 3 consensus statements, and 1 position paper). All G/Rs referred to drivers with dementia and 9/18 referred to drivers with MCI. A common approach among G/Rs is the initial trichotomization of patients in safe to drive, unsafe to drive, and undetermined cases, which are referred to a second-line evaluator. First-line evaluators are general practitioners in 10/18 G/Rs; second-line evaluators are neurologists in 7/18 G/Rs. Specific neuropsychological tests are proposed in 11/18 G/Rs and relative cut-off values in 7/18. The most commonly used tests are the MMSE, TMT, and CDT. A thorough neurological examination is proposed in only 1/18 G/R.
Conclusion
Although extensive multi-disciplinary research has provided useful information for driving behavior of cognitively impaired individuals, we are still far from a widely accepted approach of driving ability evaluation in this increasing population. A comprehensive assessment from a multi-disciplinary team in which the neurologist plays a critical role seems to be required, although this has not yet been implemented in any G/Rs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Driving is a very complex task requiring the integrity and the cooperation of various functions [1]. These include cognition and behavior and motor and somatosensory skills, all of which are subject to neurological diseases [2]. The numerous methods proposed to evaluate an individual’s fitness to drive [3,4,5] can be divided in two broad categories: (a) indirect methods, which evaluate the above-mentioned functions, which are considered to be necessary for safe driving and consequently indirectly evaluate driving capacity. These comprise neuropsychological [6, 7] and neuropsychiatric assessment [8] along with sensory and motor assessment [9, 10] and driving profile questionnaires [11, 12], and (b) direct methods, which directly evaluate driving capacity and include on-road tests [13, 14] and driving simulator tests [15, 16].
Nowadays, driving is an essential part of almost every person’s life [17]. Especially for the elderly, it not only contributes to their everyday autonomy and quality of life, but it also boosts their self-esteem and their feeling of usefulness, for example, when they transport their grandchildren [18,19,20]. Driving cessation has been associated with adverse psychological effects, including social isolation and depressive symptomatology [17, 21, 22]. However, among the elderly drivers, quite a high percentage, up to 25%, suffers from cognitive impairment [23, 24]. This impairment may be mild, as in mild cognitive impairment (MCI) [25, 26], or serious, as in dementia, most commonly due to Alzheimer’s disease (AD), interfering with instrumental activities of daily living [27, 28]. The driving ability of cognitively impaired patients is of great clinical and public health importance, and extensive research has been conducted in this field [29,30,31,32,33,34]. Beyond the cognitive [35, 36], and neuropsychiatric symptoms [37, 38], patients with MCI or AD often present motor symptoms [10, 39, 40]. Thus, a thorough and comprehensive evaluation is required to decide whether a patient suffering from MCI or mild dementia is capable to drive [41, 42].
Many countries acknowledge the need for an official evaluation of a demented person’s driving ability and have proposed national guidelines and regulations [43,44,45]. In these guidelines, common patterns can be seen, such as the need for neuropsychological evaluation; frequent re-evaluation of driving fitness; and conditional driving licenses with certain restrictions, e.g., driving only during daylight or in prespecified familiar routes. Nevertheless, so far, no international consensus has been reached regarding the appropriate procedure needed to evaluate fitness to drive and the appropriate medical specialty responsible for this evaluation. Given the nature of the diseases (AD and MCI) and the parameters examined, which include cognition, behavior, and mobility, the evaluation is based on neurological and neuropsychological assessment. Therefore, neurologists should be well informed of the driving evaluation protocol in their country and should play a critical role in driving evaluations of these patient groups.
The aim of the current article is to identify the neurological aspects of fitness to drive evaluation among patients with AD or MCI. Thus, we critically review guidelines emphasizing on the neurologist’s role.
Methods
We designed the present systematic review article adhering to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [46], taking into account both the PRISMA checklist and the PRISMA flow diagram [47]. The search was initially applied to the US National Library of Medicine database (MEDLINE via Pubmed) using terms to identify cognitive impairment (“dementia” or “cognitive impairment” or “Alzheimer’s” or “Mild Cognitive Impairment”) in combination with terms referring to driving (“driving” or “automobile driving” or “motor vehicles” or “road safety”) and guidelines ("guidelines" or "consensus" or "statement" or “recommendation”). Then, we broadened our search to Google Scholar, keeping the above-mentioned search strategy. We did so in order to retrieve guidelines or consensus statements which may have not been published as scientific papers and thus may not be indexed in MEDLINE. Finally, we searched through the reference lists of the selected articles to identify articles meeting the inclusion criteria.
The articles included met the following criteria:
-
1)
They were consensus statements, recommendation papers, official guidelines, articles reviewing the above-mentioned guidelines or position papers, written by:
-
i.
A national committee or authority (e.g., Canadian Council of Motor Transport Administrators).
-
ii.
An international working group or a scientific society (e.g., American Academy of Neurology).
-
iii.
An expert on the subject “Driving and Cognitive Impairment”.
-
2)
The recommendations included referred to the following categories:
-
i.
Individuals with MCI.
-
ii.
ii) Individuals with AD or suffering from dementia not further specified.
-
3)
Only recommendations referring to active drivers of private vehicles were included, that is, commercial vehicle drivers were excluded.
To keep our search up to date, the most recent edition of each recommendation paper was included if more than one edition had been published. Articles published before 2008 and articles with no full text in English were excluded from further analysis. Last literature update was made in June 2020.
Figure 1 shows the procedure to obtain studies meeting our inclusion criteria (as described in PRISMA flow diagram). Through our initial search, we identified 237 articles, and after screening the titles and abstracts, we excluded 171 of them as they referred to irrelevant topics. We obtained full text of the remaining 66 articles, and we excluded 44 of them because they did not meet the inclusion criteria. We thoroughly assessed the 22 remaining articles, keeping 8 and excluding 14 of them due to various reasons. After inclusion of 10 additional articles, which were identified through the references list search, 18 articles were finally included in our systematic review.

The procedure to obtain studies meeting our inclusion criteria, based on PRISMA guidelines
After collecting the articles meeting our criteria, we performed a critical review and evaluation of the selected articles so as to answer the following questions: (1) Who are the authors or the authority responsible for each study and what is the type of each study (e.g., national guidelines, consensus paper)? (2) Which is the proposed procedure to evaluate driving fitness and what are the professions of the proposed evaluators? (3) What are the neurological or neuropsychological components of the evaluation? With respect to the last question, we focused on whether there were any specific neuropsychological tests proposed and any relative cut-off values.
Results
Of the 18 articles that were included in our systematic review, nine (50%) were national guidelines from:
-
1.
Australia [43] (Austroads and National Transport Commission, endorsed by Australian and New Zealand Association of Neurologists).
-
2.
Belgium [44] (dementia experts and the Belgian Road Safety Institute, endorsed by the Belgian Medical Association).
-
3.
Canada (one paper from the Canadian Medical Association [48]).
-
4.
Canada (one paper from the Canadian Council of Motor Transport Administrators [49]).
-
5.
Ireland [50] (National Office for Traffic Medicine, Royal College of Physicians of Ireland and Road Safety Authority).
-
6.
New Zealand [51] (New Zealand Transport Agency).
-
7.
UK [52] (Driver and Vehicle Licensing Agency with advice from Honorary Medical Advisory Panels).
-
8.
USA (one paper from the American Medical Association[53]).
-
9.
USA (one paper from the National Highway Traffic Safety Administration and the American Association of Motor Vehicle Administrators[54]).
We also included five recommendation papers (28%) [55,56,57,58,59], three consensus statements (17%) [60,61,62], and one position paper (5%) [63].
All articles (18/18, 100%) referred to drivers with dementia. Six of them (34%) referred to dementia due to AD [43, 44, 54, 55, 59, 61], whereas in twelve articles (66%), the cause of dementia was not further specified. Interestingly, only nine articles (50%) referred to drivers with MCI [44, 48,49,50, 52, 55, 57, 61, 62].
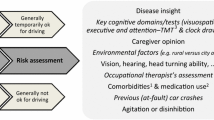
Description of the complete procedure of fitness to drive evaluation proposed in each article is beyond the goals of this paper. However, we need to highlight an approach which is proposed in eleven articles [43, 44, 48, 50, 51, 53,54,55,56, 58, 62] and seems to be the most commonly used approach in the literature [64]. According to this, patients are trichotomized by the initial evaluator in three groups: (a) safe to drive, (b) unsafe to drive, and (c) undetermined cases (Fig. 2).

The concept of trichotomization of patients regarding their driving fitness by the initial evaluator
Patients of the first group need a regular follow-up of driving fitness, while those of the second group need no further assessment. Patients of the third group are referred to the second-line evaluator (as described below). In two more articles [49, 52], patients are referred to transportation authorities upon diagnosis to make a final decision about fitness to drive, while in five articles [57, 59,60,61, 63], driving evaluation procedure is not analyzed. The need of frequent reevaluation of safe-to-drive patients is recognized in thirteen articles [43, 44, 48,49,50, 52, 54,55,56,57,58, 60, 63] (72%), and the proposed interval until re-assessment ranges from 6 months to 1 year. Restricted or conditional licenses are recommended in five articles [43, 44, 50, 55, 61] for drivers with cognitive impairment. Limitations include driving in a restricted perimeter, driving only in daylight, prohibited driving in highways, prohibited driving big vehicles, and maximum permitted speed of 80 km/h. On the other hand, in four articles [48, 49, 54, 63] (31%), conditional licenses as well as driving with a co-pilot are not regarded as protective measures and thus are contraindicated for drivers with cognitive impairment. This discrepancy depicts the lack of consensus in the literature, putting the issue of conditional licenses into a gray zone.
The proposed initial (first-line) and second-line evaluators (for undetermined cases) are presented in Table 1 for each article.
As far as the neurological and neuropsychological assessment is concerned, the need of cognitive evaluation is unanimously recognized in all included articles (100%). Nevertheless, specific neuropsychological tests or scales are proposed in only eleven articles [23, 43, 44, 48, 49, 53, 55,56,57,58, 62] (55%).
Among the neuropsychological tests, the Mini Mental State Examination (MMSE) is the most commonly used test, as it is proposed in seven articles [44, 48, 49, 54, 55, 57, 58] (39%), followed by the Trail Making Test (TMT) in six articles [48, 49, 53,54,55,56] (33%), the Clock Drawing Test (CDT) in five articles [48, 49, 53, 55, 62] (28%), and the Montreal Cognitive Assessment (MOCA) in four articles [48, 55, 58, 62] (22%).
The following tests are proposed in only one article each: the Ruler Drop Reaction Time Test (RDRT) [56], the Useful Field Of View Test (UFOV), the Judgment of Line Orientation Test (JLO), the Block Design Test (BDT), the Benton Visual Retention Test (BVRT), the Complex Figure Test (CFT), and the Facial Recognition Test (FRT) [54] (5%).
Regarding the functional scales used, the Clinical Dementia Rating Scale (CDR) and the Instrumental Activities of Daily Living Scale (IADL) are proposed in three articles each ([54, 55, 57] and [55, 56, 60], respectively).
Cut-off values for the above-mentioned neuropsychological tests are proposed in only seven articles (38%). Cut-off values for the MMSE are proposed in four articles [44, 54, 57, 58] (22%), and a score below 25/30 is generally considered as an indicator of unsafe driving. Cut-off scores for the TMT [53, 56] and the CDT [53, 62] are proposed in two articles each (11%) and for the MOCA [62] and the RDRT [56] in one article each (5%). The above-mentioned findings are summarized and analyzed further in Table 2.
Concerns of caregivers or relatives during the interview about patient’s fitness to drive are included in the assessment in nine articles [53,54,55,56,57,58, 60,61,62] (50%).
It is worth noting that a full neurological evaluation when assessing an individual’s fitness to drive is proposed in only one article, written by the American Medical Association (AMA) [53]. AMA proposes a tool called “Assessment of Driving related Skills” (ADReS), which assesses not only cognition but also motor/somatosensory function and vision. In one more article, the history of falls in drivers with cognitive impairment is recognized as a possible risk factor for unsafe driving [54]. Evaluation of functions necessary for safe driving (motor, sensory, vision, hearing) is proposed in seven articles [43, 49,50,51, 56, 57, 62] (39%). However, these recommendations are quite general and refer to every driver regardless of the underlying medical condition.
Discussion
This study aimed to make a systematic review of the existing guidelines/recommendations worldwide, regarding the evaluation of driving ability among patients with AD or MCI.
Our extensive review revealed a discrepancy between the great volume of research in the expanding field of assessing fitness to drive of patients with cognitive deficits and the small number of published guidelines/recommendations for this population. Although the extensive research uses a wide spectrum of methodologies such as driving simulator experiments and on-road tests, the existing published guidelines do not provide clear-cut indications for assessing driving abilities in everyday clinical practice. This is possibly due to methodological differences and inconclusive or inconsistent findings from the existing studies, which provide no clear-cut conclusions.
Eighteen articles met our inclusion criteria (Table 1) for guidelines/recommendations, coming from only seven countries which have published official guidelines. In these articles, the directives regarding the evaluation procedure and the recommended expertise of the evaluator of driving ability are highly heterogeneous. In addition, in two cases, published guidelines produced by certain National or International Scientific Working Groups [57, 58], are not further adopted in the official national guidelines [51, 53].
The concept of trichotomization of patients in three groups regarding their driving ability, safe to drive, unsafe to drive, and undetermined cases is a common pattern in 6 of the 18 articles of guidelines/recommendations (Fig. 2). The issue of the suggested initial evaluator remains controversial as GPs, occupational therapists, neurologists, and geriatricians are all found to be proposed as first-line evaluators across studies. Nevertheless, among them, GP is by far the most commonly encountered initial evaluator in guidelines/recommendations (10/18).
Neurologists are proposed in only one study as initial evaluators, whereas they are proposed as second-line evaluators in 40% of guidelines/recommendations, either alone or as members of a multi-disciplinary team.Concerning the utility of neuropsychological tests across the guidelines/recommendations, they are recommended in 11/18 publications. However, even in the publications where specific tests or scales are proposed, these recommendations are either empirical arbitrary or based on highly heterogeneous evidence, and relative cut-off values are frequently lacking. In addition, the neuropsychological tests proposed vary considerably (see Table 2) in 1/3 of the articles that include them. Thus, when assessing fitness to drive, no consensus has been reached either for the most appropriate neuropsychological tests or for the cut-off scores, even of the most commonly used tests, such as the MMSE and the TMT.
Furthermore, we need to highlight the complete absence in all articles (except for the AMA guidelines [53]) of a thorough neurological examination, in terms of motor and somatosensory skills evaluation. While a brief examination may be adequate for healthy elderly drivers, it is obvious that a full neurological assessment is crucial when evaluating the driving ability of a patient with cognitive impairment. Cognitive and motor impairment often co-exist, either as a single clinical entity (AD, normal pressure hydrocephalus, Parkinson’s disease, Lewy body dementia) or as a co-morbidity, especially among the elderly (degenerative arthritis, chronic heart failure, etc.) with more than one third of AD patients having also motor symptoms [65]). However, motor examination is neglected in memory clinics worldwide [66], and our review of guidelines/recommendations supports that finding, showing that neurological examination is neglected during the evaluation of driving fitness, as well.
Taking into consideration the progresses in the fields of cognitive neurology, neuropsychology, traffic science, and human factors psychology and the above-mentioned findings, a comprehensive assessment from a multi-disciplinary team in which the neurologist plays a critical role seems to be reasonable at the second level of assessment. However, our study depicts that this has not yet been implemented in the existing guidelines/recommendations. This multi-disciplinary team could consist of a GP [67], responsible for the various medical issues of the elderly other than those pertaining to dementia, e.g., vision or hearing impairment, heart problems; a transportation or occupational therapy expert [61], to address performance during an on-road or simulated driving test; a neuropsychologist [68], to perform and interpret neuropsychological tests relevant to driving fitness; and a neurologist [57, 69], responsible for evaluating motor-somatosensory skills, behavior, and cognition and integrating the results of the various assessments in a clinical judgment.
Thus, the “ideal” evaluation depends on each different situation. In the 1st level assessment, an initial general assessment, performed by the GP, followed by an assessment of key elements of safe driving, performed by the neurologist, may be sufficient in clear-cut cases. Nevertheless, this assessment must be based on (1) a complete neurological examination, (2) a short test of global cognition (e.g., MMSE, MoCA), (3) questioning the caregiver regarding patient’s everyday functionality (e.g., using the IADL scale), and (4) an interview with the patient and the caregiver focusing on patient’s driving status (history of crashes or near crashes during last year, worries about driving ability, etc.). If the 1st level assessment reveals abnormalities putting into question the driving ability, the patient should undergo 2nd level assessment including a comprehensive neuropsychological evaluation, mostly focused on executive and visuospatial functions. Tests that have been shown to be helpful in such cases include CDT, TMT-A and TMT-B, FAB, and JLO (Table 2). If there is still a doubt about driving fitness, a 3rd level assessment is warranted including either an on-road or a driving simulator test. Finally, it is important to note that even if fitness to drive is preserved, a re-assessment after 6 months is necessary for any patient with MCI or mild AD. This need for a frequent re-assessment is also evidenced by the high percentage of patients ceasing driving each year [25, 70].
An important issue that needs to be emphasized is the driving ability of patients with MCI. Despite their cognitive impairment, individuals with MCI remain relatively functional in their everyday life. However, many studies have shown that their driving ability is impaired, as even mild cognitive impairment may create difficulties with the complex and challenging task of driving [4, 11, 33, 37, 71]. Guidelines for drivers with MCI were included in only nine of the 18 articles. Most of them a priori approved MCI as a condition compatible with driving, provided that a more frequent re-assessment is performed in these patients. Nevertheless, recent knowledge coming from driving studies in this population has shown mild impairments in driving, suggesting that certain individualized restrictions could be applied in this at-risk population, such as, for example, driving at night-time and in highways [43, 44].
In conclusion, although extensive multi-disciplinary research has provided useful information for driving behavior of cognitively impaired older persons, we are still far from a widely accepted approach of driving ability evaluation in this increasing population [72].
Data availability
Not applicable.
Code availability
Not applicable.
References
Anstey KJ, Wood J, Lord S, Walker JG (2005) Cognitive, sensory and physical factors enabling driving safety in older adults. Clin Psychol Rev 25(1):45–65
Handley JD, Thomas RH, McKenna P, Hughes TAT (2017) On the road again: assessing driving ability in patients with neurological conditions. Pract Neurol 17(3):203–206
Piersma D, Fuermaier AB, de Waard D, Davidse RJ, de Groot J, Doumen MJ et al (2016) Prediction of fitness to drive in patients with Alzheimer’s dementia. PLoS One 11(2):e0149566
Hird MA, Egeto P, Fischer CE, Naglie G, Schweizer TA (2016) A systematic review and meta-analysis of on-road simulator and cognitive driving assessment in Alzheimer’s disease and mild cognitive impairment. J Alzheimers Dis 53(2):713–729
Hird MA, Vetivelu A, Saposnik G, Schweizer TA (2014) Cognitive, on-road, and simulator-based driving assessment after stroke. J Stroke Cerebrovasc Dis 23(10):2654–2670
Wolfe PL, Lehockey KA (2016) Neuropsychological assessment of driving capacity. Arch Clin Neuropsychol 31(6):517–529
Akinwuntan AE, Backus D, Grayson J, Devos H (2018) Validation of a short cognitive battery to screen for fitness-to-drive of people with multiple sclerosis. Eur J Neurol 25(10):1250–1254
Babulal GM, Stout SH, Head D, Holtzman DM, Fagan AM, Morris JC et al (2017) Neuropsychiatric symptoms and Alzheimer’s disease biomarkers predict driving decline: brief report. J Alzheimers Dis 58(3):675–680
Ranchet M, Akinwuntan AE, Tant M, Salch A, Neal E, Devos H (2016) Fitness-to-drive agreements after stroke: medical versus practical recommendations. Eur J Neurol 23(9):1408–1414
Scott KA, Rogers E, Betz ME, Hoffecker L, Li G, DiGuiseppi C (2017) Associations between falls and driving outcomes in older adults: systematic review and meta-analysis. J Am Geriatr Soc 65(12):2596–2602
Fragkiadaki S, Beratis IN, Kontaxopoulou D, Pavlou D, Andronas N, Papanicolaou A et al (2018) Self-awareness of Driving ability in the healthy elderly and patients with mild cognitive impairment (MCI). Alzheimer Dis Assoc Disord 32(2):107–113
Gooden JR, Ponsford JL, Charlton JL, Ross PE, Marshall S, Gagnon S et al (2017) Self-awareness and self-ratings of on-road driving performance after traumatic brain injury. J Head Trauma Rehabil 32(1):E50–E59
Carr DB, Barco PP, Wallendorf MJ, Snellgrove CA, Ott BR (2011) Predicting road test performance in drivers with dementia. J Am Geriatr Soc 59(11):2112–2117
Aslaksen PM, Orbo M, Elvestad R, Schafer C, Anke A (2013) Prediction of on-road driving ability after traumatic brain injury and stroke. Eur J Neurol 20(9):1227–1233
Imhoff S, Lavalliere M, Teasdale N, Fait P (2016) Driving assessment and rehabilitation using a driving simulator in individuals with traumatic brain injury: a scoping review. NeuroRehabilitation 39(2):239–251
Campos JL, Bédard M, Classen S, Delparte JJ, Hebert DA, Hyde N et al (2017) Guiding framework for driver assessment using driving simulators. Front Psychol 8:1428
Chihuri S, Mielenz TJ, DiMaggio CJ, Betz ME, DiGuiseppi C, Jones VC et al (2016) Driving cessation and health outcomes in older adults. J Am Geriatr Soc 64(2):332–341
Liddle J, Reaston T, Pachana N, Mitchell G, Gustafsson L (2014) Is planning for driving cessation critical for the well-being and lifestyle of older drivers? Int Psychogeriatr 26(7):1111–1120
Scott T, Liddle J, Mitchell G, Beattie E, Pachana N (2019) Implementation and evaluation of a driving cessation intervention to improve community mobility and wellbeing outcomes for people living with dementia: study protocol of the “CarFreeMe” for people with dementia program. BMC Geriatr 19(1):66
Carr DB, O’Neill D (2015) Mobility and safety issues in drivers with dementia. Int Psychogeriatr 27(10):1613–1622
Hill LJN, Pignolo RJ, Tung EE (2019) Assessing and counseling the older driver: a concise review for the generalist clinician. Mayo Clin Proc 94(8):1582–1588
Qin W, Xiang X, Taylor H (2020) Driving cessation and social isolation in older adults. J Aging Health 32(9):962–971
Carr DB, Ott BR (2010) The older adult driver with cognitive impairment: “it’s a very frustrating life.” JAMA 303(16):1632–1641
Chee JN, Rapoport MJ, Molnar F, Herrmann N, O’Neill D, Marottoli R et al (2017) Update on the risk of motor vehicle collision or driving impairment with dementia: a collaborative international systematic review and meta-analysis. Am J Geriatr Psychiatry 25(12):1376–1390
Connors MH, Ames D, Woodward M, Brodaty H (2017) Mild Cognitive impairment and driving cessation: a 3-year longitudinal study. Dement Geriatr Cogn Disord 44(1–2):63–70
Petersen RC, Lopez O, Armstrong MJ, Getchius TSD, Ganguli M, Gloss D et al (2018) Practice guideline update summary: mild cognitive impairment: report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology. Neurology 90(3):126–135
Connors MH, Ames D, Woodward M, Brodaty H (2018) Predictors of driving cessation in dementia: baseline characteristics and trajectories of disease progression. Alzheimer Dis Assoc Disord 32(1):57–61
McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR Jr, Kawas CH et al (2011) The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7(3):263–269
Beratis IN, Pavlou D, Papadimitriou E, Andronas N, Kontaxopoulou D, Fragkiadaki S et al (2017) Mild cognitive impairment and driving: does in-vehicle distraction affect driving performance? Accid Anal Prev 103:148–155
Jacobs M, Hart EP, Roos RAC (2017) Driving with a neurodegenerative disorder: an overview of the current literature. J Neurol 264(8):1678–1696
Piersma D, Fuermaier ABM, De Waard D, Davidse RJ, De Groot J, Doumen MJA et al (2018) Assessing fitness to drive in patients with different types of dementia. Alzheimer Dis Assoc Disord 32(1):70–75
Lovas J, Fereshtehnejad SM, Cermakova P, Lundberg C, Johansson B, Johansson K et al (2016) Assessment and reporting of driving fitness in patients with dementia in clinical practice: data from SveDem, the Swedish Dementia Registry. J Alzheimers Dis 53(2):631–638
Anstey KJ, Eramudugolla R, Chopra S, Price J, Wood JM (2017) Assessment of driving safety in older adults with mild cognitive impairment. J Alzheimers Dis 57(4):1197–1205
Eramudugolla R, Huque MH, Wood J, Anstey KJ 2020 On-road behavior in older drivers with mild cognitive impairment. J Am Med Dir Assoc
Piersma D, de Waard D, Davidse R, Tucha O, Brouwer W (2016) Car drivers with dementia: Different complications due to different etiologies? Traffic Inj Prev 17(1):9–23
Sachdev PS, Blacker D, Blazer DG, Ganguli M, Jeste DV, Paulsen JS et al (2014) Classifying neurocognitive disorders: the DSM-5 approach. Nat Rev Neurol 10(11):634–642
Beratis IN, Andronas N, Kontaxopoulou D, Fragkiadaki S, Pavlou D, Papatriantafyllou J et al (2017) Driving in mild cognitive impairment: the role of depressive symptoms. Traffic Inj Prev 18(5):470–476
Kales HC, Gitlin LN, Lyketsos CG (2014) Detroit Expert Panel on A, Management of neuropsychiatric symptoms of D. Management of neuropsychiatric symptoms of dementia in clinical settings: recommendations from a multidisciplinary expert panel. J Am Geriatr Soc. 62(4):762–9
Tolea MI, Morris JC, Galvin JE (2016) Trajectory of mobility decline by type of dementia. Alzheimer Dis Assoc Disord 30(1):60–66
Kueper JK, Speechley M, Lingum NR, Montero-Odasso M (2017) Motor function and incident dementia: a systematic review and meta-analysis. Age Ageing 46(5):729–738
Fuermaier ABM, Piersma D, de Waard D, Davidse RJ, de Groot J, Doumen MJA et al (2019) Driving difficulties among patients with Alzheimer’s disease and other neurodegenerative disorders. J Alzheimers Dis 69(4):1019–1030
Fuermaier AB, Piersma D, de Waard D, Davidse RJ, de Groot J, Doumen MJ et al (2017) Assessing fitness to drive-a validation study on patients with mild cognitive impairment. Traffic Inj Prev 18(2):145–149
Austroads 2017 Assessing fitness to drive for commercial and private vehicle drivers. 5th ed: National Library of Australia
Versijpt J, Tant M, Beyer I, Bier JC, Cras P, De Deyn PP et al (2017) Alzheimer’s disease and driving: review of the literature and consensus guideline from Belgian dementia experts and the Belgian road safety institute endorsed by the Belgian Medical Association. Acta Neurol Belg 117(4):811–819
Kim YJ, An H, Kim B, Park YS, Kim KW (2017) An international comparative study on driving regulations on people with dementia. J Alzheimers Dis 56(3):1007–1014
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 350:g7647
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4:1
Association CM (2012) CMA driver's guide: determining medical fitness to operate motor vehicles. 8th ed: Canadian Medical Association
(CCMTA) CCoMTA (2017) Determining Driver Fitness in Canada
National Office for Traffic Medicine RCoPoIRRSAR (2017) Sláinte agus Tiomáint: medical fitness to drive guidelines. 6th ed
Agency NZT (2014) Medical aspects of fitness to drive: a guide for health practitioners
Agency DaVL (2018) Assessing fitness to drive – a guide for medical professionals
Association AM (2010) Physician’s guide to assessing and counselingolder drivers. 2nd ed
Administrators NHTSAatAAoMV (2009) Driver fitness medical guidelines
Cameron DH, Zucchero Sarracini C, Rozmovits L, Naglie G, Herrmann N, Molnar F et al (2017) Development of a decision-making tool for reporting drivers with mild dementia and mild cognitive impairment to transportation administrators. Int Psychogeriatr 29(9):1551–1563
group ODTw (2009) The driving and dementia toolkit (for health professionals). 3rd ed
Iverson DJ, Gronseth GS, Reger MA, Classen S, Dubinsky RM, Rizzo M et al (2010) Practice parameter update: evaluation and management of driving risk in dementia: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 74(16):1316–1324
Hoggarth P, Innes C, Dalrymple-Alford J, Croucher M, Severinsen J, Gray J et al (2011) Assessment of older drivers in New Zealand: the current system, research and recommendations. Australas J Ageing 30(3):148–155
Martin AJ, Marottoli R, O'Neill D (2013) Driving assessment for maintaining mobility and safety in drivers with dementia. Cochrane Database Syst Rev. (8):CD006222.
Rapoport MJ, Chee JN, Carr DB, Molnar F, Naglie G, Dow J et al (2018) An international approach to enhancing a national guideline on driving and dementia. Curr Psychiatry Rep 20(3):16
Wheatley CJ, Carr DB, Marottoli RA (2014) National highway traffic safety a, American occupational therapy a, association for driver rehabilitation S. Consensus statements on driving for persons with dementia. Occup Ther Health Care. 28(2):132–9
Rapoport MJ, Naglie G, Herrmann N, Zucchero Sarracini C, Mulsant BH, Frank C et al (2014) Developing physician consensus on the reporting of patients with mild cognitive impairment and mild dementia to transportation authorities in a region with mandatory reporting legislation. Am J Geriatr Psychiatry 22(12):1530–1543
Australian, New Zealand Society for Geriatric M (2010) Australian and New Zealand Society for Geriatric Medicine position statement driving and dementia. Australas J Ageing. 29(3):137–41
Sg P, Ion B, Dionysia K, Stella F, Dimosthenis P, George Y (2016) Does the diagnosis of Alzheimer’s disease imply immediate revocation of a driving license? International Journal of Clinical Neurosciences and Mental Health 3(Suppl. 1):S02
Scarmeas N, Hadjigeorgiou GM, Papadimitriou A, Dubois B, Sarazin M, Brandt J et al (2004) Motor signs during the course of Alzheimer disease. Neurology 63(6):975–982
Costa A, Bak T, Caffarra P, Caltagirone C, Ceccaldi M, Collette F et al (2017) The need for harmonisation and innovation of neuropsychological assessment in neurodegenerative dementias in Europe: consensus document of the Joint Program for Neurodegenerative Diseases Working Group. Alzheimers Res Ther 9(1):27
Lee L, Molnar F (2017) Driving and dementia: Efficient approach to driving safety concerns in family practice. Can Fam Physician 63(1):27–31
Bernstein JPK, Calamia M, Meth MZ, Tranel D (2019) Recommendations for driving after neuropsychological assessment: a survey of neuropsychologists. Clin Neuropsychol 33(6):971–987
Caruana P, Hughes AR, Lea RA, Lueck CJ (2018) Australian driving restrictions: how well do neurologists know them? Intern Med J 48(9):1144–1149
Stamatelos P, Chatzaki P, Beratis I, Pavlou D, Andronas N, Fragkiadaki S, et al., editors (2021) Alzheimer’s dementia and predictors of driving cessation: results from a 4-year Longitudinal study 7th Congress of the European Journal of Neurology; Virtual Congress: European Journal of Neurology.
Hird MA, Vesely KA, Fischer CE, Graham SJ, Naglie G, Schweizer TA (2017) Investigating simulated driving errors in amnestic single- and multiple-domain mild cognitive impairment. J Alzheimers Dis 56(2):447–452
Classen S, Monahan M, Auten B, Yarney A (2014) Evidence-based review of interventions for medically at-risk older drivers. Am J Occup Ther 68(4):e107–e114
Adler G, Rottunda S, Dysken M (2005) The older driver with dementia: an updated literature review. J Safety Res 36(4):399–407
Logsdon RG, Teri L, Larson EB (1992) Driving and Alzheimer’s disease. J Gen Intern Med 7(6):583–588
Fox GK, Bowden SC, Bashford GM, Smith DS (1997) Alzheimer’s disease and driving: prediction and assessment of driving performance. J Am Geriatr Soc 45(8):949–953
Devlin A, McGillivray J, Charlton J, Lowndes G, Etienne V (2012) Investigating driving behaviour of older drivers with mild cognitive impairment using a portable driving simulator. Accid Anal Prev 49:300–307
Ott BR, Papandonatos GD, Davis JD, Barco PP (2012) Naturalistic validation of an on-road driving test of older drivers. Hum Factors. 54(4):663–74
Watanabe T, Konagaya Y, Yanagi T, Miyao M, Mukai M, Shibayama H (2012) Study of daily driving characteristics of individuals with dementia using video-recording driving recorders. J Am Geriatr Soc 60(7):1381–1383
Fitten LJ, Perryman KM, Wilkinson CJ, Little RJ, Burns MM, Pachana N et al (1995) Alzheimer and vascular dementias and driving. A prospective road and laboratory study. JAMA. 273(17):1360–5
Odenheimer GL, Beaudet M, Jette AM, Albert MS, Grande L, Minaker KL (1994) Performance-based driving evaluation of the elderly driver: safety, reliability, and validity. J Gerontol 49(4):M153–M159
Molnar F, Rapoport M, Roy M (2012) Driving and dementia : maximizing the utility of inoffice screening and assessment tools. Can Geriatr Soc J CME
Kawano N, Iwamoto K, Ebe K, Suzuki Y, Hasegawa J, Ukai K et al (2012) Effects of mild cognitive impairment on driving performance in older drivers. J Am Geriatr Soc 60(7):1379–1381
Staplin L, Lococo KH, Gish KW, Decina LE (2003) Model driver screening andevaluation program & Maryland pilot older driver study. NHTSA Report Number DOT HS 809 581 Washington, DC: National Highway Traffic Safety Administration
Stutts JC, Stewart JR, Martell C (1998) Cognitive test performance and crash risk in an older driver population. Accid Anal Prev 30(3):337–346
Tarawneh MS, Patrick TBishu, Ramaratnam RBallard, John L (1993) Factors associated with driving performance of older drivers. Transportation Research Record. 1405.
Ball KK, Roenker DL, Wadley VG, Edwards JD, Roth DL, McGwin G et al (2006) Can high-risk older drivers be identified through performance-based measures in a Department of Motor Vehicles setting? J Am Geriatr Soc 54(1):77–84
Grace J, Amick MM, D’Abreu A, Festa EK, Heindel WC, Ott BR (2005) Neuropsychological deficits associated with driving performance in Parkinson’s and Alzheimer’s disease. J Int Neuropsychol Soc 11(6):766–775
Hunt L, Morris JC, Edwards D, Wilson BS (1993) Driving performance in persons with mild senile dementia of the Alzheimer type. J Am Geriatr Soc 41(7):747–752
Uc EY, Rizzo M, Anderson SW, Shi Q, Dawson JD (2006) Unsafe rear-end collision avoidance in Alzheimer’s disease. J Neurol Sci 251(1–2):35–43
Szlyk JP, Myers L, Zhang Y, Wetzel L, Shapiro R (2002) Development and assessment of a neuropsychological battery to aid in predicting driving performance. J Rehabil Res Dev 39(4):483–496
De Raedt R, Ponjaert-Kristoffersen I (2000) The relationship between cognitive/neuropsychological factors and car driving performance in older adults. J Am Geriatr Soc 48(12):1664–1668
Rizzo M, Reinach S, McGehee D, Dawson J (1997) Simulated car crashes and crash predictors in drivers with Alzheimer disease. Arch Neurol 54(5):545–551
Uc EY, Rizzo M, Anderson SW, Shi Q, Dawson JD (2004) Driver route-following and safety errors in early Alzheimer disease. Neurology 63(5):832–837
Reger MA, Welsh RK, Watson GS, Cholerton B, Baker LD, Craft S (2004) The relationship between neuropsychological functioning and driving ability in dementia: a meta-analysis. Neuropsychology 18(1):85–93
Freund B, Gravenstein S, Ferris R, Burke BL, Shaheen E (2005) Drawing clocks and driving cars. J Gen Intern Med 20(3):240–244
Rebok GW, Keyl PM, Bylsma FW, Blaustein MJ, Tune L (1994) The effects of Alzheimer disease on driving-related abilities. Alzheimer Dis Assoc Disord 8(4):228–240
Brown LB, Ott BR, Papandonatos GD, Sui Y, Ready RE, Morris JC (2005) Prediction of on-road driving performance in patients with early Alzheimer’s disease. J Am Geriatr Soc 53(1):94–98
Duchek JM, Carr DB, Hunt L, Roe CM, Xiong C, Shah K et al (2003) Longitudinal driving performance in early-stage dementia of the Alzheimer type. J Am Geriatr Soc 51(10):1342–1347
Hunt LA, Murphy CF, Carr D, Duchek JM, Buckles V, Morris JC (1997) Environmental cueing may effect performance on a road test for drivers with dementia of the Alzheimer type. Alzheimer Dis Assoc Disord 11(Suppl 1):13–16
Hunt LA, Murphy CF, Carr D, Duchek JM, Buckles V, Morris JC (1997) Reliability of the Washington University road test. A performance-based assessment for drivers with dementia of the Alzheimer type. Arch Neurol. 54(6):707–12
Funding
This review is part of Dr. Stamatelos’ PhD project with title “Evaluation of driving behavior of patients with MCI, Dementia or Parkinson’s Disease: Diagnostic and Prognostic Markers” funded and supported by Alexander S. Onassis Public Benefit Foundation (Grant number: G ZN 060–1/2017–2018).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Data collection and analysis were performed by Petros Stamatelos and Sokratis G. Papageorgiou. The first draft of the manuscript was written by Petros Stamatelos, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
None.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Stamatelos, P., Economou, A., Stefanis, L. et al. Driving and Alzheimer’s dementia or mild cognitive impairment: a systematic review of the existing guidelines emphasizing on the neurologist’s role. Neurol Sci 42, 4953–4963 (2021). https://doi.org/10.1007/s10072-021-05610-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-021-05610-7