
Abstract
Background
The frequency of Huntington’s disease (HD) may vary considerably, with higher estimates in non-Asian populations. We have recently examined the prevalence of HD in the southern part of Sardinia, a large Italian Mediterranean island that is considered a genetic isolate. We observed regional microgeographic differences in the prevalence of HD across the study area similar to those recently reported in other studies conducted in European countries. To explore the basis for this variability, we undertook a study of the incidence of HD in Sardinia over a 10-year period, 2009 to 2018.
Methods
Our research was conducted in the 5 administrative areas of Sardinia island. Case patients were ascertained through multiple sources in Sardinia and Italy.
Results
During the incidence period 53 individuals were diagnosed with clinically manifested HD. The average annual incidence rate 2009–2018 was 2.92 per 106 persons-year (95% CI, 2.2 to 3.9). The highest incidence rate was observed in South Sardinia (6.3; 95% CI, 4.2–9.5). This rate was significantly higher (p<0.01) than the rates from Cagliari, Oristano, and Sassari provinces but did not significantly differ (p = 0.38) from the Nuoro rate.
Conclusions
The overall incidence of HD in Sardinia is close to the correspondent estimates in Mediterranean countries. Our findings highlight also the possibility of local microgeographic variations in the epidemiology of HD that might reflect several factors, including a possible founder effect in the rural areas of South Sardinia and Nuoro.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Huntington’s disease (HD) is a neurodegenerative disease caused by a fully penetrant autosomal dominant mutation in the huntingtin gene (HTT) localized on chromosome 4 [1]. This mutation encodes an expansion to 36 CAG triplet repeats or greater that provokes accumulation of the mutant Huntington protein in specific neuronal populations and progressively leads to neuronal degeneration [1]. Clinical symptoms usually manifest between 35 and 45 years of age (but can also occur in childhood or in the elderly) and may include chorea, psychiatric manifestations, cognitive dysfunctions up to dementia [1,2,3,4].
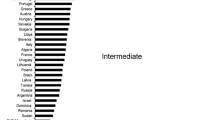
Although HD is considered a rare disease, its frequency may vary considerably with higher estimates in non-Asian populations [5,6,7,8,9]. Previous studies estimated average HD incidence at 0.5–1 per 106 persons-year in populations of Asian descent and at 1–8 per 106 persons-year in non-Asian populations and [6,7,8]. In Europe, the incidence of HD also varied widely with higher estimates in the UK, lower estimates in Finland, and intermediate estimates in Mediterranean countries like Greece and Spain [5,6,7,8,9]. In Italy, the only incidence study recently conducted in Northern Italy provided an incidence rate of 3 per 106 persons-year [9].
We have recently examined the prevalence of HD in a restricted area of Sardinia, a large Italian Mediterranean island characterized by genetic and socio-cultural isolation throughout the centuries [10]. Analysis of this population resulted in an overall prevalence rate of 5.98 × 105 [11], an estimate in line with the prevalence reported in several Mediterranean countries. However, we observed marked regional microgeographic differences in the prevalence of HD across the study area, similar to the findings from two recent studies that simultaneously assessed HD prevalence in neighboring regions of Finland [12] and Sweden [13].
In the present study, we assessed the incidence of HD in the overall Sardinia over a 10-year period (2009 to 2018) in order to compare the incidence of HD in this genetic and socio-cultural isolate with European countries [8, 9], and also to further explore the basis for the previously highlighted microgeographic variability in HD prevalence [11].
Methods
Our research was conducted in the 5 administrative areas of Sardinia island (Fig. 1). The Island covers a surface of about 24,040 km2. During the study period, population decreased from 1,672,404 (January 1, 2009) to 1,639,591 (December 31, 2018) inhabitants, with an average of 1,663,859 inhabitants at the middle of the period, 814,953 men and 848,906 women (Italian Statistical Institute: www. istat.it). Figure 1 also shows the medical facilities for HD across Sardinia. These included one laboratory providing genetic analysis for HD since 1993 (Binaghi Hospital, Cagliari), two tertiary referral centers for HD, the Institute of Neurology of the University of Cagliari and the Institutes of Neurology and Genetics of the University of Sassari, and 7 general neurology centers. All the aforementioned centers are part of the National Health System network with free access for Sardinian population.

Sardinia provinces and medical facilities for Huntington’s disease
To identify individuals with HD, we first referred to the one genetic laboratory and the two tertiary referral centers for HD. Additional cases were actively sought out through contact with the other public neurologic institutions in Sardinia, and with neurologists from tertiary referral centers in Italy where Sardinian HD patients could likely have been evaluated (Institute of Neurology from the Universities of Bononia, Genoa, Rome Sapienza, Rome Cattolica, and Naples “Federico II,” and the Neurologic Institutes C. Besta and Humanitas from Milan, Italy).
Patient records were reviewed in order to confirm the diagnosis that was accepted if the patient had a phenotype suggesting HD (i.e., chorea and/or psychiatric signs and/or cognitive decline) and an expansion of the CAG repeat in the HTT gene greater than 36. Age at disease onset was the age at first symptoms. Juvenile HD (onset < 21 years), late HD (onset > 60 years), and the rigid Westphal variant [2] were also taken into consideration. Asymptomatic individuals who screened positive at the genetic test were not included in this survey. Number of CAG repeats was also assessed in a sample of 63 normal subjects hosted in the study areas. The study was approved by the Institutional Review Board of the University Hospital of Cagliari.
An incident case was defined as any individual fulfilling the aforementioned criteria and who resided in the study area at the time of clinical onset in the incidence period (January 1 2009 to December 31 2018). The incidence of HD was calculated on the basis of the number of clinically symptomatic cases newly diagnosed by genetic testing per million inhabitants per year during the period 2009 to 2018. The average population was the population at the middle of the period. Data were computed for the whole region and for each of the five administrative areas. Age-adjusted incidence rates were adjusted by the direct method to the 2011–2020 European standard population [14]. In a sample of randomly selected 63 normal subjects who were born in the study area, mean number of CAG repeats was 17.6 + 2.2.
Data were expressed as mean and standard deviation (SD) unless otherwise indicated. Differences between groups were tested by the Mann-Whitney U test, while Spearman rho was computed to assess correlation between variables. Difference between two rates was checked by the statistical software MedCalc that uses the “Test based Method” and the “Exact Poisson Method” given by Sahai H and Khurshid A [15].
Results
During the incidence period, 53 individuals who resided in Sardinia (36 women and 17 men aged 55.7 + 14.1 years) were diagnosed with clinically manifested HD. Mean age of neurological symptom onset was 48.9 + 12.6 years and mean age at diagnosis was 50.3 + 13.7 years. There was 1 patient with juvenile onset (< 21 years) and 2 patients with late HD onset (> 60 years). All patients received genetic confirmation: mean number of CAG repeats was 42.9 + 2.4 in the HD allele, 17.8 + 2.4 in the normal allele (p < 0.001). The length of the CAG repeat in the expanded allele was inversely correlated with age at diagnosis (Spearman rho = −0.77, p<0.0001).
The average annual incidence rate 2009–2018 was 2.92 per 106 persons-year (95% CI, 2.2 to 3.9). Incidence tended to be higher (p = 0.01) in women (3.9 per 106 persons-year; 95% CI, 2.7 to 5.5) than in men (1.8 per 106 persons-year; 95% CI, 1.0 to 3.0), and in the age band 40 to 59 years (Fig. 2).

Age-specific average annual incidence rates (× 1,000,000 persons-year) in Sardinia, 2009–2018
Stratifying by Sardinian provinces (Table 1), the highest incidence rate was observed in South Sardinia (6.3; 95% CI, 4.2–9.5). This rate was significantly higher (p<0.01) than the rates from Cagliari (1.9; 95% CI, 1.1–3.9), Oristano (0.6; 95% CI, 0.1–3.5), and Sassari (2.2; 95% CI, 1.2–3.9) provinces but did not significantly differ (p = 0.38) from the Nuoro rate (3.2; 95% CI, 1.6–6.7). We did not observed any significant difference among provinces in regard to sex distribution, age at HD onset and mean CAG repeats in diseased and normal subjects from each study area (Table 1).
Among the 53 incident cases, 5 patients and their parents were Italians born outside Sardinia, whereas the remaining 48 cases were from Sardinian families. Among the 48 incident cases of Sardinian ancestry, 43 (from 22 families) had an established family history of HD while 5 cases were apparently sporadic. Parents of the 5 patients with negative family history were either alive or had died at the age of 65 years or older without symptoms compatible with HD. Since additional DNA molecular analysis aiming at identifying or excluding an intermediate allele in one or more asymptomatic first-degree relatives could not be carried out, these patients were considered “possible” new mutations.
Limiting analysis to the 48 patients of Sardinian origin, the average annual incidence rate was 2.65 per 106 persons-year (95% CI, 2.05–3.52). Most HD families of Sardinian ancestry (14/22, 64%) were concentrated in South Sardinia and Nuoro, two provinces that accounted for about one-third of the Sardinian population. Considering patients of Sardinian ancestry from these two areas together yielded a combined incidence rate of 5.2 per 106 persons-year (95% CI, 3.5–7.4), a rate that was significantly different (p= 0.01) from the correspondent Cagliari, Oristano, and Sassari rates.
Discussion
This study reports an average incidence rate of 2.92 per 106 persons-year in Sardinia over a 10-year period. Incidence was higher in women than in men and in the age band 40–59 years. Our analysis also highlighted regional variation in the incidence of HD across the 5 administrative areas of Sardinia, with the higher incidence rate in the provinces of South Sardinia and Nuoro.
The overall incidence rate observed in Sardinia was lower than the estimates recently reported in the UK and North America [6], higher than the estimates from Iceland, Finland, and Asian countries [6] and slightly lower than the estimates from other Mediterranean countries like, Greece and Spain [7, 8]. With regard to Italy, the Sardinian estimate was close to the incidence rate recently observed in the city of Ferrara (3 per 106 persons-year) [9].
To our knowledge, microgeographic variations in the incidence of HD have never been reported even though regional differences in the prevalence of HD have recently been observed in neighboring regions of Finland [12], Sweden [13], and Sardinia [11]. Indeed, the heterogeneity of the estimates of the incidence of HD in Cagliari and South Sardinia provinces is consistent with the varying prevalence rates of HD in the same areas [11]. The variability in the incidence of HD across Sardinia might merely be due to differences in the access to health care and diagnosis for HD patients. Localization of clinical and genetic point references for HD in Cagliari and Sassari, however, would have provided a greater incidence of HD in these areas, which it was not. Likewise, variability in genetic modifiers of the expression of the disease like specific haplotypes in the HTT gene and length of the CAG repeats in normal chromosomes [16, 17] is unlikely to be an explanation for the observed heterogeneity in the estimates of the incidence of HD. Although we did not assess specific risk haplotypes for HD, the CAG repeat length in normal alleles was uniform across Sardinia. It is interesting that 9% of the cases were from outside the Sardinian community, for which we have no explanation. However, limiting analysis to Sardinian patients did not modify the microgeographic variations in the incidence of HD highlighted in this study.
Regional differences in the epidemiology of HD have recently been associated with sociodemographic factors [18]. Hence the two administrative regions characterized by higher incidence (South Sardinia and Nuoro provinces) were rural areas with lower migratory fluxes, lower socioeconomic conditions, and less specialized health care. The provinces characterized by lower incidence (Cagliari, Oristano, and Sassari provinces), on the other hand, were more urban regions with a greater intensity of migratory fluxes, higher socioeconomic conditions, and more specialized health care. The higher incidence of HD and the greater concentration of HD families in more rural areas with lower migratory fluxes (South Sardinia and Nuoro provinces) would be consistent with a founder effect but also with possible differences in the expression of epigenetic disease modifiers. For instance, rural areas of Sardinia host several millions sheep and dairy intake has recently been associated with risk of phenoconversion in HD [19]. Interestingly, the combined incidence rate from these two areas was close to the incidence rates observed in Spain [7] and Greece [8]. This might suggest potential common modifiers of the expression of the disease in the Mediterranean area.
Our study may have limitations. Like previous epidemiological studies, this was a service-based study and incomplete case ascertainment would have likely occurred. Owing to the hypothesized rarity of HD, however, population-based study are difficult to perform and also ethically unfeasible. Although the frequency of underdiagnosis is difficult to quantify, our ascertainment methodology (the study was conducted by checking multiple data sources) probably limited ascertainment bias inherent to study design. Supporting this view, study population resembled the general population of HD cases for several demographic and clinical features, i.e., the higher incidence of the disease in the fourth to sixth decade [1], the frequency of patients with juvenile and late-onset HD [2, 3], and also the greater incidence in women than in men. Although information on gender distribution was inconsistent in most epidemiological studies, the largest study of Huntington’s disease epidemiology to date noted slightly higher HD frequency among women as compared to men [20]. We do not know whether the supposed isolated cases are indeed new mutations. However, our findings are in line with Falush et al. [20] who estimated that the new mutation rate for HD is likely to be 6 to 14% of currently known cases in each generation.
In conclusion, our findings highlight the possibility of geographic variations in the incidence of HD in Sardinia that might reflect several factors. Although the overall incidence of HD in Sardinia is lower than those found in the UK, Australia, and Americas, and higher than those of North Eastern Europe, Asia, and Africa, it is close, particularly in the more rural areas, to the correspondent estimates in other Mediterranean countries like Greece and Spain [5,6,7,8,9]. The homogeneity of incidence estimates in the Mediterranean area would also suggest potential common modifiers of expression of HD in this area. Among possible candidates, nutrients from the Mediterranean diet might affect HD clinical expression but, to date, only a few studies have explored the issue [21].
References
Bates GP, Dorsey R, Gusella JF, Hayden MR, Kay C, Leavitt BR, Nance M, Ross CA, Scahill RI, Wetzel R, Wild EJ, Tabrizi SJ (2015) Huntington disease. Nat Rev Dis Primers 1:15005
Quarrell O, O'Donovan KL, Bandmann O, Strong M (2012) The prevalence of juvenile Huntington’s disease: a review of the literature and meta-analysis. PLoS Curr 4:e4f8606b742ef3
Chaganti SS, McCusker EA, Loy CT (2017) What do we know about Late Onset Huntington’s Disease? J Huntingtons Dis 6:95–103
Capiluppi E, Romano L, Rebora P, Nanetti L, Castaldo A, Gellera C, Mariotti C, Macerollo A, Cislaghi MG (2020) Late-onset Huntington’s disease with 40-42 CAG expansion. Neurol Sci 41:869–876
Rawlins MD, Wexler NS, Wexler AR, Tabrizi SJ, Douglas I, Evans SJ, Smeeth L (2016) The prevalence of Huntington’s disease. Neuroepidemiology. 46(2):144–153
Wexler NS, Collett L, Wexler AR, Rawlins MD, Tabrizi SJ, Douglas I, Smeeth L, Evans SJ (2016) Incidence of adult Huntington’s disease in the UK: a UK-based primary care study and a systematic review. BMJ Open 6:e009070
Ramos-Arroyo MA, Moreno S, Valiente A (2005) Incidence and mutation rates of Huntington’s disease in Spain: experience of 9 years of direct genetic testing. J Neurol Neurosurg Psychiatry 76:337–342
Panas M, Karadima G, Vassos E et al (2011) Huntington’s disease in Greece: the experience of 14 years. Clin Genet 80:586–590
Carrassi E, Pugliatti M, Govoni V, Sensi M, Casetta I, Granieri E (2017) Epidemiological study of Huntington’s disease in the province of Ferrara, Italy. Neuroepidemiology. 49:18–23
Cavalli-Sforza LL, Piazza A (1993) Human genomic diversity in Europe: a summary of recent research and prospects for the future. Eur J Hum Genet 1:3–18
Muroni A, Murru MR, Sechi M, Ercoli T, Marrosu F, Bentivoglio AR, Petracca M, Maria Scaglione CL, Soliveri P, Cocco E, Pedron M, Murgia M, Deriu M, Cuccu S, Ulgheri L, Zuccato C, Defazio G (2020) Prevalence of Huntington’s disease in Southern Sardinia, Italy. Parkinsonism Relat Disord 80:54–57
Sipilä JO, Hietala M, Siitonen A, Päivärinta M, Majamaa K (2015) Epidemiology of Huntington's disease in Finland. Parkinsonism Relat Disord 21:46–49
Roos AK (2017) iklund L, Laurell K. Discrepancy in prevalence of Huntington’s disease in two Swedish regions. Acta Neurol Scand 136:511–515
Eurostat report 2013 (https://ec.europa.eu/eurostat/documents/3859598/5926869/KS-RA-13-028-EN.PDF/e713fa79-1add-44e8-b23d-5e8fa09b3f8f)
Sahai H, Khurshid A (1996) Formulae and tables for the determination of sample sizes and power in clinical trials for testing differences in proportions for the two-sample design: a review. Stat Med 15(1):1–21
Warby SC, Visscher H, Collins JA, Doty CN, Carter C, Butland SL, Hayden AR, Kanazawa I, Ross CJ, Hayden MR (2011) HTT haplotypes contribute to differences in Huntington disease prevalence between Europe and East Asia. Eur J Hum Genet 19:561–566
Ylönen S, Sipilä JOT, Hietala M, Majamaa K (2019) HTT haplogroups in Finnish patients with Huntington disease. Neurol Genet 5:e334
Bruzelius E, Scarpa J, Zhao Y, Basu S, Faghmous JH, Baum A (2019) Huntington’s disease in the United States: variation by demographic and socioeconomic factors. Mov Disord 34:858–865
Marder JA, Gu Y, Eberly S et al (2013) Relationship of Mediterranean diet and caloric intake to phenoconversion in Huntington disease. JAMA Neurol 70:1382–1388
Falush D, Almqvist EW, Brinkmann RR et al (2001) Measurement of mutational flow implies both a high new-mutation rate for Huntington disease and substantial underascertainment of late-onset cases. Am J Hum Genet 68:373–385
Christodoulou CC, Demetriou CA, Zamba-Papanicolaou E (2020) Dietary intake, Mediterranean diet adherence and caloric intake in Huntington’s disease: a review. Nutrients 12:2946–2971
Acknowledgements
We thank all the Sardinian HD patients and families for their closeness and trust.
Funding
This work was supported by Fondazione Banco di Sardegna (project number 2019.1850) to Dr Antonella Muroni and to Huntington Onlus, The Italian Network for Huntington’s disease, a lay patients association.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The study was approved by the local Institutional Review Board of University Hospital of Cagliari and all the procedures being performed were part of the routine care.
Conflict of interest
The authors declare no competing interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Muroni, A., Murru, M.R., Ulgheri, L. et al. Geographic differences in the incidence of Huntington’s disease in Sardinia, Italy. Neurol Sci 42, 5177–5181 (2021). https://doi.org/10.1007/s10072-021-05217-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-021-05217-y