
Abstract
Introduction
The debate continues as to whether laparoscopic total Nissen (LNF) versus partial posterior Toupet fundoplication (LTF) leads to better outcomes in the surgical treatment of axial hiatal hernia with gastroesophageal reflux disease. In the most recent meta-analysis including 13 RCTs with 1564 patients, no significant difference was found between the two procedures in terms of perioperative complications and recurrent reflux rates. Further comparative analyses are urgently needed.
Methods
This retrospective analysis of prospectively recorded data from the Herniamed Registry compared the perioperative and 1-year follow-up outcomes after total Nissen versus partial Toupet fundoplication. Propensity score matching was chosen as the statistical method. Matching was performed for n = 2290 pairs.
Results
No systematic discrepancy was found between the Nissen and Toupet fundoplication for any of the outcome parameters (intraoperative complications LNF 2.10% vs LTF 1.48%, general complications 2.27% vs 2.88%, postoperative complications 1.44% vs 1.18%, complication-related reoperation 1.00% vs 0.91%, recurrence on 1-year follow-up 6.55% vs 5.33%, pain on exertion on 1-year follow-up 12.49% vs 9.52%, pain at rest on 1-year follow-up 10.44 vs 9.52% and pain requiring treatment on 1-year follow-up 9.61% vs 8.17%). Also the postoperative dysphagia rate showed with 5.34% after LNF and with 4.64% after LTF no significant difference.
Conclusion
The findings presented here did not show any significant difference up to 1 year after Nissen or Toupet fundoplication. This is in concordance with the findings of the meta-analyses. However, the perioperative and 1-year follow-up outcomes demonstrate that both operation techniques should be carried out by experienced surgeons.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastroesophageal reflux disease (GERD) is one of the most common diseases encountered by gastroenterologists, surgeons and primary care physicians [1]. The global prevalence of GERD is 13.98%; in Europe, the prevalence is 14.12% and in North America 19.55% [2]. The estimated number of persons with GERD is 1.03 billion.
According to the World Gastroenterology Organization Global Guidelines, the core principles of GERD management entail lifestyle interventions and reduction of esophageal luminal acid either by local acid neutralization or by suppression of gastric acid secretion using medical treatment, or, rarely, antireflux surgery [3]. Surgical intervention may be considered in large hiatal hernia causing volume-related reflux symptoms with evidence of aspiration or cardia dysfunction, noncompliance with medical treatment, side effects of medical therapy, esophagitis refractory to medical treatment or persistent symptoms caused by refractory GERD [3].
In the surgical guidelines for management of GERD, SAGES recommends either partial or complete fundoplication [4]. If reflux rather than dysphagia is the patient’s main symptom, complete fundoplication should be carried out [4]. If the risk of dysphagia is to be kept to a minimum, partial fundoplication should be given preference [4].
At a multi-society consensus conference, a conditional recommendation with moderate certainty of evidence stated that a patient with GERD would be more likely to benefit from partial rather than complete fundoplication [5]. That recommendation is based on six meta-analyses [7,8,9,10,11,12].
The maximum number of available RCTs is 13 studies with 1564 patients [8]. In that meta-analysis, no significant difference was found in the perioperative complications or the recurrent reflux rates. Often, however, only relatively small subgroups are available to answer individual questions [7]. There is also a paucity of routine comparative clinical studies.
This analysis of prospectively recorded data retrospectively compared Nissen with Toupet fundoplication using propensity score matching. Only patients with axial hiatal hernia and reflux disease and for whom no mesh was used for hiatoplasty reinforcement were included in the present analysis. The main focus of analysis was on the perioperative and 1-year follow-up outcome.
Methods
Registry design
Herniamed is an Internet-based hernia registry in which hospitals and independent surgeons in Germany, Austria and Switzerland can voluntarily document their routine hernia operations. A contract is made with every responsible surgeon where the latter commits to ensuring that data on the hernia operations carried out in the hospital/surgical clinics are completely and correctly entered into the Herniamed Registry. As a prerequisite for documentation in the Herniamed Registry, all patients must sign a separate consent form agreeing to their data being processed in the Herniamed Registry and indicating their acceptance of the follow-up procedure. As part of the information provided to patients regarding participation in the Herniamed Registry, they are told to inform the treating hospital or the treating clinic about any problem occurring after hernia repair. If problems occur after the hernia operation, the patient should attend the treating hospital or surgical clinic for examination.
All complications are recorded up to postoperative day 30. To ensure that all postoperative complications are in fact recorded, the patient is asked about them again on 1-year follow-up. On 1-year follow-up, patients and their primary care physicians are sent a questionnaire asking them about pain and recurrent reflux. If such problems are experienced, patients are requested to attend the hospital/medical practice for further diagnostic examination. Studies have revealed that follow-up by means of a questionnaire sent to the patient and/or their primary care physician is effective [13].
The findings reported in the returned questionnaires are entered into a database by the treating hospital/medical practice and are then available for pseudonymous statistical analysis.
The present analysis of prospectively recorded data retrospectively compared the outcomes of patients with axial hiatal hernia who underwent laparoscopic Nissen or Toupet fundoplication without the use of a mesh for hiatoplasty.
Inclusion criteria for the analysis
From the processed data with a total of 1,152,149 cases, patients were selected for analysis based on the following inclusion criteria:
-
Hiatal hernia operations
-
The entry-state key of the patient master data as well as of the operation data shows status complete, i.e., only completely documented cases for obligatory entries
-
Patients at least 16 years old (only valid entries on age)
-
Only elective hernias
-
Only primary procedures
-
Only procedures with axial location (type I)
-
Only patients with reflux
-
Only operations with Nissen or Toupet fundoplication
-
Only laparoscopic procedures
-
Only procedures without a mesh
-
Operation date up to and including 28/02/2022
-
1-year follow-up with fully documented visits
Methodology
All analyses were performed with the software SAS 9.4 (SAS Institute Inc., Cary, NC, USA) and intentionally calculated to a full significance level of 5%, i.e., they were not corrected in respect of multiple tests, and each p value ≤ 0.05 represents a significant result.
Data processing
Individual outcome and also independent variables (risk factors, complications) were summarized to global variables. A general, intra- or postoperative complication or risk factor was deemed present if at least one single item applied.
Descriptive and unadjusted statistics
Categorical patient data were presented as absolute and relative frequencies.
For continuous data the mean and standard deviation, or for log-transformed data in case of non-normal distribution, the mean and range (because the range is not symmetrical after back transformation) were presented.
Unadjusted analyses were carried out for analysis of the comparison groups in respect of the individual matching parameters. These were used to describe the patient cohort before matching. For categorical parameters, the asymptotic Chi-square test was performed. For continuous parameters, the robust t test (Satterthwaite) was used.
Propensity score matching
Nissen and Toupet fundoplication outcomes were compared using first a propensity score matching to compare patients with balanced co-variable profiles. Propensity scores were generated using a logistic regression model (Nissen vs. Toupet) with the following matching variables:
-
Age in years
-
Defect size in cm2—logarithmized
-
BMI [underweight/normal weight/overweight/obesity]
-
ASA [I/II/III–IV]
-
Preoperative pain [yes/no/unknown]
-
Regurgitation/reflux [yes/no]
-
Dysphagia [yes/no]
-
Pain [yes/no]
-
Anemia [yes/no]
-
Lung disorders [yes/no]
-
Risk factors [yes/no]
Risk factors were deemed to be present if at least one of the following risk factors applied
-
COPD [yes/no]
-
Diabetes mellitus [yes/no]
-
Aortic aneurysm [yes/no]
-
Immunosuppression [yes/no]
-
Corticoids [yes/no]
-
Smoking abuse [yes/no]
-
Coagulopathy [yes/no]
-
Platelet aggregation inhibitors (discontinued less than seven days ago [yes/no]
-
Coumarin derivatives (quick/INR not in normal range) [yes/no]
-
Non-vitamin K antagonist oral anticoagulants (NOAKs, e.g., Xarelto) discontinued < 2 days [yes/no]*
-
Liver cirrhosis [yes/no]*
*since database update (February 2022).
In addition, the following fixed matching variable was specified:
-
Gender [male/female]*
which had to have the same category in the matched pair.
Propensity score matching was performed using greedy algorithm and a caliper of 0.2 standard deviations. The balance of the matched sample was checked using standardized differences (also given for the pre-matched sample) that should not exceed 10% (< 0.1) after matching.
Analysis of outcome parameters after matching
Matched samples were then analyzed via McNemar’s exact test (test for systematic deviation between the paired patients) for the following perioperative and 1-year follow-up outcomes:
-
Intraoperative complications
-
Postoperative complications
-
General complications
-
Complication-related reoperations
-
1-year follow-up
-
Pain at rest
-
Pain on exertion
-
Pain requiring treatment
-
Recurrence
-
Trocar hernia
-
Secondary hemorrhage
-
Blood effusion
-
Infection
The results obtained are presented as the concordant cases as well as non-diagonal elements (disadvantageous cases) of the 2 × 2 frequency table, the corresponding p values and the odds ratio (OR) estimates for matched samples with corresponding 95% confidence interval.
In addition, the ORs are illustrated in a forest plot for all outcome parameters.
Results
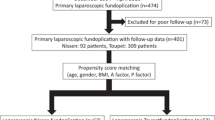
Patient selection was made in accordance with the patient inclusion flowchart presented in Fig. 1. Following patient selection, 5281 patients were finally enrolled in the analysis to study the relation of the operation technique as well as of other potential influencing variables of the outcome parameters. Here, Nissen fundoplication was used in 2560 (48.5%) cases and Toupet fundoplication in 2721 (51.5%) cases.

Patient inclusion flowchart
Descriptive statistics and unadjusted analyses before matching
In this section, differences between the operation techniques for the matching variables were analyzed. Table 1 presents the descriptive statistics as well as the unadjusted test results for the continuous variables age and defect size. Table 2 shows the corresponding values for the categorical variables. Unadjusted analysis of the relationship between the comparison groups and the intraoperative, general and postoperative complications, complication-related reoperations, recurrences, pain at rest, pain on exertion and pain requiring treatment as well as trocar hernias, secondary hemorrhage, blood effusions and infections on 1-year follow-up before matching is shown in Table 3.
Matching
Propensity score matching of the 2560 cases treated with Nissen technique with the 2721 cases with the Toupet technique was performed for n = 2290 (89.5%) patients. The standardized differences of the matching variables both before (original sample) and after (matched sample) matching are shown in Fig. 2.

Scatter plot of standardized differences before and after matching
For all the matching variables, the standardized difference after matching is less than 10%, indicating good balancing of the variables included in the model.
Statistical analyses
Table 4 gives a summary of the analysis results of the comparison groups for the various outcome parameters. Here, analysis focused on whether there were systematic differences in the outcomes of the Nissen versus Toupet fundoplication operations. No systematic discrepancy was found between the comparison groups for any of the outcome parameters (Table 4, Fig. 3). Also the postoperative dysphagia rate showed with 5.34% after LNF and with 4.64% after LTF no significant difference (p = 0.289).

Forest plot of adjusted odds ratio (OR) including confidence intervals for perioperative and 1-year follow-up outcomes comparing Nissen versus Toupet fundoplication
Recurrent reflux following LNF (n = 150) was diagnosed only radiologically in 58 cases (38.7%), in 28 cases (18.7%) radiologically and endoscopically, in 57 cases (38.0% only endoscopically and in 7 cases (4.7%) only clinically. In the patient population following LTF (n = 122), recurrent reflux was found by endoscopy only in 61 cases (50.0%), by endoscopy and radiology in 21 cases (17.2%) and clinically in 21 (17.2%) cases.
Standardized differences for patients with and without follow-up-Information
Figure 4 shows the results of the standardized differences for patients with (n = 5281) and without (n = 2804) follow-up information. Standardized differences above a value of 10% were found only for age. The patients in the analysis population were on average 3.6 years older. Standardized differences of less than 0.1 were found for all other variables, including the perioperative complication rates, and are thus not suggestive of any bias in patient selection.

Scatter plot of standardized differences between patients with and without follow-up information
Discussion
Analysis after propensity score matching using prospectively recorded data from the Herniamed Registry demonstrates that for comparative patient cohorts, there was no significant difference between Nissen and Toupet fundoplication with respect to the perioperative and 1-year follow-up outcomes. But this applies only for patients with type I axial hiatal hernias and reflux disease and without mesh augmentation of hiatoplasty.
The perioperative complication rate for both operation techniques was around 6% and additionally 5% for postoperative dysphagia. The complication-related reoperation rate was around 1%. The recurrent reflux rate, in the majority of cases proven by radiology or endoscopy, was around 6% after 1 year for both techniques. Around 8% of patients still reported pain requiring treatment after Nissen or Toupet fundoplication. Pain on exertion was even over 11%. A recent meta-analysis also found a reflux recurrence rate of 11.5% for the Nissen fundoplication and 9.6% for the Toupet fundoplication with no significant difference in the short term [7]. In the long-term follow-up, the reflux recurrence rate also showed no significant difference (LNF 17.3% vs LTF 13.2%) [7]. We do not conclude equality from our data, but that there was no significant difference. There is no prediction on 5-year results from our 1-year follow-up data.
Likewise, the rate of chest pain in the meta-analysis was over 12% [7]. This highlights the fact that surgical treatment of GERD by means of laparoscopic Nissen or Toupet fundoplication is associated with a not inconsiderable postoperative complication rate as well as recurrence and pain rate. Accordingly, surgery should be indicated for GERD on the basis of the international guidelines [1, 2, 4,5,6]. Similarly, the operation technique should be selected in accordance with the recommendations. If the main focus is on treatment of the reflux, preference should be given to Nissen fundoplication, and if the risk of dysphagia is to be kept to a minimum, the recommendation is more for Toupet fundoplication [4]. Due to a lack of evidence, the role of robotic fundoplication cannot yet be evaluated at present [4]. According to the guidelines, surgical repair is as effective as conservative treatment provided that the patients are carefully selected for the operation and the procedure is carried out by an experienced surgeon [14]. The learning curve in antireflux laparoscopic surgery is considered as particularly steep [15]. Registry analyses have weaknesses. First, there is the issue of data accuracy and completeness. All participating institutions have signed a contract with Herniamed stating that the surgeon is responsible for data accuracy and completeness. At the time of audits for certification of hernia centers, the auditor can check data entries in Herniamed.
The Herniamed Registry has been validated against data from the statutory health insurance funds, thus attesting to the necessary accuracy. Since 1-year follow-up information is not available for one-third of patients, it is necessary to rule out selection bias. On analysis of the standardized differences for patients with and without follow-up, values below 0.1 were routinely found, also for the perioperative complication rates, which argue against selection bias.
In summary, it can be stated that for axial hiatal hernia with GERD and appropriate surgical indication based on fundus manometry test results, no systematic differences between the Nissen and Toupet operation could be found. Since the perioperative complications as well as the recurrence and pain rates are of relevance, these operations should be performed by experienced surgeons.
Data availability
The data that support the findings of this study are available from the corresponding author (FK) upon reasonable request.
References
Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ (2022) ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 117:27–56. https://doi.org/10.14309/ajg.0000000000001538
Nirwan JS, Hasan SS, Babar ZU, Conway BR, Ghori MU (2020) Global prevalence and risk factors of gastro-oesophageal reflux disease (GORD): systematic review with meta-analysis. Sci Rep 10:5814. https://doi.org/10.1038/s41598-020-62795-1
Hunt R, Armstrong D, Katelaris P, Afihene M, Bane A, Bhatia S, Chen MH, Choi MG, Melo AC, Fock KM, Ford A, Hongo M, Khan A, Lazebnik L, Lindberg G, Lizarzabal M, Myint T, Moraes-Filho JP, Salis G, Lin JT, Vaidya R, Abdo A, LeMair A (2017) World gastroenterology organisation global guidelines: GERD global perspective on gastroesophageal reflux disease. J Clin Gastroenterol 51:467–478. https://doi.org/10.1097/MCG.0000000000000854
Slater BJ, Dirks RC, McKinley SK, Ansari MT, Kohn GP, Thosani N, Qumseya B, Billmeier S, Daly S, Crawford C, Ehlers PA, Hollands C, Palazzo F, Rodriguez N, Train A, Wassenaar E, Walsh D, Pryor AD, Stefanidis D (2021) SAGES guidelines for the surgical treatment of gastroesophageal reflux (GERD). Surg Endosc 35:4903–4917. https://doi.org/10.1007/s00464-021-08625-5
Slater BJ, Collings A, Dirks R, Gould JC, Qureshi AP, Juza R, Rodríguez-Luna MR, Wunker C, Kohn GP, Kothari S, Carslon E, Worrell S, Abou-Setta AM, Ansari MT, Athanasiadis DI, Daly S, Dimou F, Haskins IN, Hong J, Krishnan K, Lidor A, Litle V, Low D, Petrick A, Soriano IS, Thosani N, Tyberg A, Velanovich V, Vilallonga R, Marks JM (2023) Multi-society consensus conference and guideline on the treatment of gastroesophageal reflux disease (GERD). Surg Endosc 37:781–806. https://doi.org/10.1007/s00464-022-09817-3
McKinley SK, Dirks RC, Walsh D, Hollands C, Arthur LE, Rodriguez N, Jhang J, Abou-Setta A, Pryor A, Stefanidis D, Slater BJ (2021) Surgical treatment of GERD: systematic review and meta-analysis. Surg Endosc 35:4095–4123. https://doi.org/10.1007/s00464-021-08358-5
Li G, Jiang N, Chendaer N, Hao Y, Zhang W, Peng C (2023) Laparoscopic nissen versus toupet fundoplication for short- and long-term treatment of gastroesophageal reflux disease: a meta-analysis and systematic review. Surg Innov 30:15533506231165828. https://doi.org/10.1177/15533506231165829
Tian ZC, Wang B, Shan CX, Zhang W, Jiang DZ, Qiu M (2015) A meta-analysis of randomized controlled trials to compare long-term outcomes of nissen and toupet fundoplication for gastroesophageal reflux disease. PLoS ONE 29(10):e0127627. https://doi.org/10.1371/journal.pone.0127627
Du X, Hu Z, Yan C, Zhang C, Wang Z, Wu J (2016) A meta-analysis of long follow-up outcomes of laparoscopic Nissen (total) versus Toupet (270°) fundoplication for gastro-esophageal reflux disease based on randomized controlled trials in adults. BMC Gastroenterol 2(16):88. https://doi.org/10.1186/s12876-016-0502-8
Tan G, Yang Z, Wang Z (2011) Meta-analysis of laparoscopic total (Nissen) versus posterior (Toupet) fundoplication for gastro-oesophageal reflux disease based on randomized clinical trials. ANZ J Surg 81:246–252. https://doi.org/10.1111/j.1445-2197.2010.05481.x
Broeders JA, Mauritz FA, Ahmed Ali U, Draaisma WA, Ruurda JP, Gooszen HG, Smout AJ, Broeders IA, Hazebroek EJ (2010) Systematic review and meta-analysis of laparoscopic Nissen (posterior total) versus Toupet (posterior partial) fundoplication for gastro-oesophageal reflux disease. Br J Surg 97:1318–1330. https://doi.org/10.1002/bjs.7174
Rausa E, Ferrari D, Kelly ME, Aiolfi A, Vitellaro M, Rottoli M, Bonitta G, Bona D (2023) Efficacy of laparoscopic Toupet fundoplication compared to endoscopic and surgical procedures for GERD treatment: a randomized trials network meta-analysis. Langenbecks Arch Surg 408(1):52. https://doi.org/10.1007/s00423-023-02774-y
Baucom RB, Ousley J, Feurer ID, Beveridge GB, Pierce RA, Holzman MD, Sharp KW, Poulose BK (2016) Patient reported outcomes after incisional hernia repair—establishing the ventral hernia recurrence inventory. Am J Surg 212:81–88. https://doi.org/10.1016/j.amjsurg.2015.06.007
Katz PO, Gerson LB, Vela MF (2015) Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 108:308–328. https://doi.org/10.1038/ajg.2012.444
Kapoor T, Deschamps C (2017) Secrets for successful antireflux surgery: learning curve. Ann Laparosc Endosc Surg 2:90. https://doi.org/10.21037/ales.2017.05.01
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Köckerling reports grants to fund Herniamed from Johnson&Johnson, Norderstedt, Karl Storz, Tuttlingen, MenkeMed, Munich, and DB Karlsruhe, as well as personal fees from DB Karlsruhe. All other authors have nothing to disclose.
Ethical approval
Only cases of routine hernia surgery were documented in the Herniamed Registry and all patients have signed a special informed consent declaration agreeing to participate. The Herniamed Registry has ethical approval (BASEC Nr. 2016—00123; 287/2017 BO2; F-2022-111).
Human and animal rights
This article does not contain any study with animals performed by any of the authors.
Informed consent
All patients with routine hernia surgery documented in the Herniamed Registry have signed an informed consent declaration agreeing to participate.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Köckerling, F., Jacob, D., Adolf, D. et al. Laparoscopic total (Nissen) versus posterior (Toupet) fundoplication for gastroesophageal reflux disease: a propensity score-matched comparison of the perioperative and 1-year follow-up outcome. Hernia (2024). https://doi.org/10.1007/s10029-024-02988-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10029-024-02988-z