
Abstract
Introduction
There are few, controversial, and limited studies on factors associated with the perception of profile beauty. Moreover, no study has ever assessed the role of laterality in esthetic judgment. Hence, this clinical trial was conducted.
Methods
Photographs of 6 patients (3 women) with normal lip position (Ricketts norm = 0 mm) and facial convexity (Legan-Burstone norm = 12°) were digitally manipulated to create two series of 9 gradient images each, with convexity changes of 2° and anteroposterior lip modifications of 1 mm. Half of profiles were flipped horizontally. Laypeople (n = 35), orthodontists (n = 19), and maxillofacial surgeons (n = 10) selected the esthetically acceptable images (6912 esthetic evaluations [2 parameters × 6 sets × 9 images × 64 judges]). Effects of photogrammetric stimuli and other factors on judges’ zone of esthetical acceptability (ZA) and its midrange were assessed statistically (α = 0.05).
Results
Orthodontists and surgeons had respectively the broadest and narrowest ZAs (p < 0.05, ANOVA). Mean midranges of surgeons, orthodontists, and laypeople were respectively 0.27 ± 1.35, 0.56 ± 1.46, and 0.41 ± 1.77 mm for males’ lower lips (p = 0.710, ANOVA); 0.27 ± 1.10, − 0.44 ± 0.91, and 0.03 ± 1.56 mm for females’ lower lips (p = 0.034); 10.40 ± 3.17°, 11.09 ± 2.86°, and 11.57 ± 3.84° for men’s profile convexity (p = 0.246); 10.27 ± 3.20°, 11.05 ± 1.87°, and 11.13 ± 3.26° for women’s profile convexity (p = 0.346). Judges’ gender did not affect their esthetic perception (p > 0.1). When patients’ left side of face was visible, judges’ esthetic preference parameters shifted towards a less convex profile and a narrower ZA (p < 0.05).
Conclusion
Slightly protruded lips (for men) and slightly less convex profiles (for men/women) might be favored by all groups. Women’s esthetic lip positions might differ among groups. Judges’ gender might not be a determinant. Subjects’ face side can influence judges’ esthetic perception of facial convexity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Esthetics is a Greek word meaning pleasing to the senses; it is a subjective phenomenon and can vary from person to person, depending on numerous factors such as fashions, geography, culture, socioeconomic status, education, gender, age, maturity, education, or even morphologic properties of faces of the referees, or geographic areas; therefore, it is possible for the majority of a society to prefer thicker lips, while in another population, thinner lips may be more commonly regarded as desirable [1,2,3,4,5,6,7,8,9,10,11,12].
The attractiveness and beauty of the face affects the shaping of personality and social relationships. The lips are a major factor in the beauty of the face, attracting most of the audience’s attention (besides the eyes) [13]. In fact, the main motive of about 80% of adults who seek orthodontic treatment for themselves or their children is to enhance facial attractiveness regardless of the structure and function of the underlying orofacial area [14].
Because of internationalization and ease of immigration, many patients and clinicians have or will have multi-ethnical and multi-cultural backgrounds [2]. Moreover, since results pertaining to esthetic preferences of the assessed populations are not necessarily generalizable to other populations [15], the knowledge of esthetic preferences of each culture and ethnicity is of importance to clinicians worldwide [2].
The soft tissue and its components like lip position and facial convexity play an important role in esthetics (and therefore in orthodontic diagnosis and treatment planning) [2, 7, 11, 16]. To achieve proper esthetics, it is necessary to first define facial harmony and beauty [2]. Soft tissue profile esthetics can be determined differently by clinicians and laypersons; therefore, the assessment of esthetic factors from the perspective of laypersons as well as clinicians including orthodontics and maxillofacial surgeon is necessary [2, 17, 18]. These psychophysical assessments can be obtained by showing the judges (clinicians or laypeople) different representations of the profile such as photogrammetric profile silhouettes, drawings, caricatures, cephalographs, real photographs, or touched-up photographs, also by using a technique, namely perceptometrics, which allows computerized manipulation of facial profile’s features within a defined range [19,20,21,22]. This technique can be used to create controlled photogrammetric changes in profiles for evaluation of esthetic acceptability preferences of laypeople or clinicians.
Despite the importance of esthetics, the literature on factors affecting the attractiveness of soft tissue profile is relatively few, quite controversial, and mostly limited by small samples [2, 4, 6, 7, 19,20,21,22,23,24,25]. Of these, few studies have compared the esthetic perception of individuals of different backgrounds [2]; comparison of the esthetic perception of orthodontists with that of other professions is quite rare and in some cases non-existent (such as orthodontists versus maxillofacial surgeons). The objective of this study was to compare for the first time the esthetic preferences of orthodontists, maxillofacial surgeons, and laypeople to a range of lip positions and profile convexities in photographs of subjects created using the perceptometrics method. Also, it was assessed for the first time that whether changing the direction of the subjects’ profiles (from the standard direction to the horizontally flipped one) can affect the esthetic judgment of the viewer.
The null hypotheses comprised the lack of differences between esthetic perceptions of judges (1) among different education backgrounds, (2) between male and female judges, (3) while looking at male versus female profiles, and (4) while looking at the right side of test faces versus looking at their left sides; they also included (5) the absence of differences between the optimum esthetic measurements observed in this study with the corresponding norms.
Materials and methods
This clinical trial included 3456 esthetic evaluations (6 sets of 9 images each, rated by 64 judges) for lip prominence and 3456 assessments for facial convexity angles. To begin, 6 images (3 women, 3 men) were randomly selected from an orthodontic photography archive of about 3000 patients attending a private orthodontic office, according to the following inclusion criteria: the patients had to be aged between 18 and 35 years old, be of Iranian decent, without any craniofacial syndromes and disorders, and having a normal profile convexity and lip prominence. The Ricketts E-line (a line connecting the soft tissue pogonion to the tip of the nose) was used to measure the lip prominence. The normal distance from this line should be 1 mm and 0 for the upper and lower lips, respectively. Facial profile convexity was assessed according to the Legan-Burstone analysis, in which the angle between the lines “glabella-subnasale and subnasale-pogonion” should be 12° [26,27,28]. The photograph had to be in natural head position and of proper image quality (not blurred and completely showing all facial features). Written signed consents were obtained from the included subjects. The protocol ethics were approved by the university’s ethics committee in accordance with the Helsinki declaration (registered as GP95210).
Photogrammetric stimuli
In order to modify the lip prominence and profile convexity using the perceptometrics method, an image editing program (Photoshop 2017, Adobe, USA) was used by a graphic designer and an orthodontist. Two series of 9 images each were created for each subject; on them, the parameters “lip prominence and profile convexity” were manipulated. Lip prominence was modified with increments of 1 mm, according to Table 1. Facial convexity angle was modified by increments of 2° through moving the mandible, chin, and lower lip (Table 2).
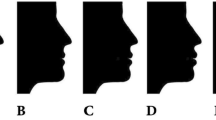
Among the 6 sets of convexity series (a total of 54 images), image sets of three patients (27 images) were selected randomly and flipped horizontally (mirrored right to left, Fig. 1). The same was done for lip prominence series as well (Fig. 2).

Series of images with modifications in the profile convexity (the eyes were not masked in the experiment)

Series of images with modifications in the lip positions (the eyes were not masked in the experiment)
Esthetic evaluation of profiles
These images were evaluated esthetically by judges who were contacted directly and asked to participate. The inclusion criteria for the judges were being Iranian, being consent to participate, knowing their right to leave the study at their will, and belonging to one of the following three groups: (A) laypeople—35 individuals including 21 women and 14 men, without any educations in fields relevant to facial esthetics completed the survey. Among them, 8 had high school diploma degrees or lower, 15 had bachelor of science, 8 had master of sciences, and 4 had PhDs or higher. (B) Orthodontists—of the 20 orthodontists who originally agreed to participate, 19 (6 women and 13 men) agreed to participate and finished the survey. (C) Oral and maxillofacial surgeons—of the 20 surgeons who agreed to participate, 10 (1 woman and 9 men) completed the survey. Overall, 64 judges (28 females and 36 males) were included. The age ranges of laypeople, orthodontists, and surgeons were respectively about “20–65,” “30–55,” and “30–55” years old.
The images were shown to the judges using an online system. Each set of 9 images was presented as a series of horizontally attached images, in which all images were sorted from right to left or vice versa (Figs. 1 and 2). All image sets were presented within the same webpage survey, and the judges could freely scroll down or up to see whichever set they desired to evaluate, for how many times they wanted. The judge could zoom in or out of the webpage. There was no limitation on the time of assessment. The order of the sets on the webpage was randomly selected, but it was fixed and not changing randomly in each browsing session.
The judges were asked to select the range of images considered by them to be esthetically acceptable (i.e., the zone of acceptability, ZA) and discard the unattractive images. The ZA had four parameters: the minimum and maximum ends, size, and midpoint. For instance, a judge could select the range between the images 2 and 6 as acceptable (i.e., the ZA). In this case, the ZA span would be 5 images wide. The minimum and maximum ends of the ZA would be the images 2 and 6, respectively. And the median (midpoint, midrange) of the ZA would be the image 4; this point would indicate the most esthetic measurement within the ZA, because the midrange has the longest distance from the unacceptable zones on both sides. The ZA size selected by each judge could be between 1 and 9 images wide.
Statistical analysis
The numbers of test profiles and judges were determined based on previous literature; the number of judges was supposed to be the same for all groups initially (i.e., 20 per group), but many surgeons who had agreed to participate originally refused later to complete the survey due to time limitations. The number of laypeople (who were more available) was later augmented to keep the number of judges as 60, as predetermined originally. It eventually reached 64 judges.
A Cronbach alpha was used to assess the internal consistency of the minimum and maximum ends of the selected ZA across the 6 image sets of convexity angles or the 6 sets of lip prominences (males and females combined). The internal consistencies for the minimum and maximum profile convexities were 77.1% and 72.1%, respectively (p < 0.001). For the minimum and maximum lip prominences, the internal consistencies were 81.8% and 74.3%, respectively (p < 0.001).
The midranges (medians) of the acceptability ranges (i.e., ZAs) were determined as the optimum esthetic value. Characteristics of the acceptable ranges (ZAs) were summarized for facial convexity and the lower lip. Since both the upper and lower lips had been edited to the exact same amount, the same lower lip ZA values minus 1 mm equaled the upper lip values (according to the Ricketts norm definitions, the lower and upper lips are respectively 0 and 1 mm behind the Ricketts E-line).
The mean midranges were compared with the normal values, using a one-sample t test. Esthetic parameters were compared between the profiles of men versus women, using a paired t test. The correlations between ZA parameters of male and female test subjects were estimated using a Pearson correlation coefficient. A one-way analysis of variance (ANOVA) followed by a Tukey post hoc test was used to compare the opinions of judges. An independent sample t test was used to compare the esthetic preferences of male versus female judges, to compare the genders of test subjects, and to compare profile directions (subjects with left vs. right sides of faces visible). A multivariable mixed effects linear model was used to simultaneously assess the effects of the judge groups, judge sexes, test subject sexes, and the direction of the face of the test subjects on the ZA parameters. The software used was SPSS 25 (IBM, Armonk, NY, USA). The level of significance was set at 0.05.
Results
Comparisons between the ZAs of male and female profiles
Detailed descriptive statistics and 95% confidence intervals (CIs) for the whole sample are presented in Tables 3 and 4.
Profile convexity
Mean acceptable convexities ranged from 8.40° to 14.09° for profiles of male subjects, while they ranged between 7.93° and 14.14° for preferable female profiles. The paired t test showed insignificant differences between most of the ZA parameters of female profiles versus male profiles; the mean of the minimum of the ZA was about 0.5° greater in males compared to females (p = 0.127), while the mean of the maximum end of the range was almost similar in both genders (p = 0.871). The mean size of the ZA was greater in women (p = 0.039); the mean of the midrange of the ZA was about 0.3° greater in men, but it was not significant (p = 0.356, Table 3).
The one-sample t test showed that mean profile convexity midranges of men and women were significantly lower than the norm (p ≤ 0.003).
The Pearson correlation coefficient showed significant correlations between male and female profile convexities in terms of the minimums of ZA (r = 0.339, p < 0.001), maximums of ZA (r = 0.199, p = 0.006), range spans (r = 0.458, p < 0.001), and midranges (r = 0.203, p = 0.005).
Lip prominence
Mean acceptable lower lip limits in male profiles ranged between 0.88 mm posterior to the Ricketts line and 1.75 mm anterior to the Ricketts line (the values for the upper lips would be the same values minus 1 mm). In female profiles, the mean ZA ranged between 1.44 mm posterior to the Ricketts line and 1.30 mm anterior to that line (the upper lip values being 1 mm posterior to these values). The mean of the minimum limit of the ZA was significantly more protruded in males compared to females (p = 0.0001, paired t test); similarly, the mean of the maximum end of the ZA was more advanced in males (p = 0.0013). The mean ZA was slightly wider in females than males, but it was not significant (p = 0.261). The mean of the midrange of the lower lip ZA was 0.43 mm anterior to the Ricketts line in men while it was almost touching the Ricketts line (0.07 mm posterior to it) in women (p = 0.0002, Table 4). Of course, the mean of the median acceptable upper lip positions (midrange) would be posterior to the Ricketts line in both genders. Mean lower lip prominence midranges of men (p = 0.0003) but not women (p = 0.454) were significantly greater than the norm (p ≤ 0.003).
There were significant correlations between male and female lip prominences in terms of the minimums of ZA (r = 0.323, p < 0.001), maximums of ZA (r = 0.186, p = 0.010), range spans (r = 0.336, p < 0.001), and midranges (r = 0.250, p < 0.001).
Comparisons between the esthetic preferences of orthodontists, surgeons, and laypeople
Profile convexity
The comparison of the scores given to profile convexities by orthodontists, surgeons, and laypeople (Table 5) revealed significant differences in esthetic preferences of these groups, only in the case of the mean ZA of convexities of male profiles (in which surgeons had the narrowest range [4.5°] while orthodontists had the widest range [6.9°]). The Tukey test showed significant differences between orthodontists with surgeons or laypeople (both p values ≤ 0.002) but not between surgeons and laypeople (p = 0.329). The maximum end of the ZA for male profiles was marginally significant among the three groups of judges (p = 0.068, Table 5).
Considering the opinions of the referees towards the esthetics of women profile convexities, the maximum end of the ZA differed significantly among the three groups of judges (p = 0.025). The only significant post hoc comparison was between orthodontists and surgeons (p = 0.021); the other two post hoc comparisons were insignificant (p > 0.2). Also, there was a significant difference among the three groups of judges in terms of the ranges of acceptability (again surgeons having the narrowest zone (average = 4.5°) and orthodontists having the broadest zone (7.7°), p < 0.001, Table 5). The Tukey test indicated significant differences between orthodontists with surgeons or laypeople (both p values ≤ 0.001); however, the difference between surgeons and laypeople was insignificant (p = 0.111).
All the groups’ mean midranges were lower than the norm; these comparisons reached the level of significance for all groups (all p values ≤ 0.019) except the subgroup of laypeople judging male profiles (p = 0.255).
Lip prominence
The comparison of the preferable lip prominences among the three groups of referees showed some significant differences (Table 6). In the case of male profiles, the sizes of the zones of acceptability differed among the judges (orthodontists having the broadest zones [3.0 mm] and surgeons having the narrowest zones [2.1 mm], p = 0.011). According to the Tukey, the only significant post hoc comparison was between orthodontists and surgeons (p = 0.008), while the other two comparisons were insignificant (p > 0.140).
Regarding female lip prominences, the three groups of judges had different opinions in the case of minimum acceptable limit (p = 0.005 [orthodontists tolerating the most retruded lips and surgeons accepting the least retruded ones]), sizes of ZAs (p = 0.023, orthodontists accepting wider ranges of changes and surgeons preferring the narrowest range), and midranges of ZAs (p = 0.034, surgeons having a mean midrange of about 0.4 mm and 1.4 mm posterior to the Ricketts line for the lower and upper lips, respectively; while orthodontists having a mean midrange of about 0.3 mm anterior to that line for the lower lip and 0.7 mm posterior to the Ricketts line for the upper lip).
The Tukey test was used to follow up on the significant ANOVA results; comparing the minimum limits of three judge groups showed a significant difference between orthodontists and surgeons (p = 0.006). The differences between orthodontists and laypeople (p = 0.058) and between surgeons and laypeople (p = 0.253) were not significant. The size of the ZA was significantly greater in orthodontists compared to surgeons (Tukey p = 0.017), but was not significantly different between orthodontists and laypeople (p = 0.558) or between surgeons and laypersons (p = 0.076). The midrange scores were significantly different between orthodontists and surgeons (p = 0.052), but were not significantly different between orthodontists and laypeople (p = 0.086) or between surgeons and laypeople (p = 0.664).
Mean ZA midranges of surgeons did not differ significantly from the norm (both p values > 0.190, one-sample t test). Orthodontists’ mean midrange for assessment of men profiles was significantly greater than the norm (p = 0.005), while their mean midrange for women profiles was significantly smaller than the norm (p = 0.001). For laypeople, mean midrange of women esthetic lip range did not differ from the norm (p = 0.851); however, their midrange of men lip position was significantly greater than the norm (p = 0.018).
Comparisons between the opinions of male versus female judges
The independent sample t test showed that the esthetic preferences of male referees did not differ significantly from those of female judges, in terms of any of the parameters assessed either in male subjects or in female subjects (all p values > 0.1, Tables 7 and 8).
Differences between the acceptable ranges of right-looking versus left-looking faces
Profile convexity
The independent sample t test showed that the perception by judges of subjects with right or left sides of faces visible differed: compared to left-looking faces, subjects’ right-looking faces had greater minimum acceptable convexities (marginally significant), greater maximum acceptable convexities, broader acceptable convexity ranges, and greater acceptable convexity midpoints (indicating more convex profiles being determined as esthetic in right-looking faces, Table 9).
Lip prominence
The judges’ esthetic perception of the subjects’ lip prominence did not differ significantly based on the direction of subjects’ faces (all p values > 0.1, Table 9).
Mixed-model multivariable analysis
A mixed-effects linear model was used to assess the effects of the factors “judges’ professions and sexes together with subjects’ sexes and face sides” on the convexity and lip ZA parameters. The results confirmed the role of subjects’ face direction in differences of esthetic facial convexity perceived by judges. They also showed significant effects of subjects’ gender on the judges’ esthetic perception of some parameters pertaining to lip positions and profile convexities (Table 10). Since initial models showed no significant interactions between the effects of subject’ and judges’ genders, this interaction was removed from the final model.
Discussion
Some researchers have shown that dental professionals and laypeople similarly rate profiles’ esthetics [8, 29, 30]. According to certain authors, the higher experience and education of orthodontists and specialists compared to laypersons may not necessarily matter when it comes to a generally attractive profile [14]. The findings of this study indicated that all the groups assessed preferred lips slightly anterior to the ideal Ricketts norm in men but not in women (for which, orthodontists preferred retruded lips while surgeons preferred slightly protruded lips and finally laypeople found the Ricketts norm more attractive). All tended to prefer profiles slightly less convex than Legan-Burstone norm for men. For women, laypersons and surgeons preferred profiles as convex as Legan-Burstone norm, while orthodontists preferred profiles mildly more concave than this particular norm. Compared to surgeons who had rather narrower ranges of esthetic tolerances, orthodontists found a broader range of lip prominences and profile convexities as acceptable. Our results were in contrast to some findings of Sodagar and Borujeni [2] who compared the opinions of orthodontists, dental students, and orthodontic patients regarding the profile silhouettes of men and women. They concluded that all groups preferred the mean profile for men and profiles but with mildly retruded lips for women, while orthodontic patients approved a broader range for men and favored retruded lips for women; all groups disliked profiles with greatly protruded lips [2]. Similarly, Ioi et al. [22] assessed favorable anteroposterior position of lips in Japanese and concluded that orthodontists and dental students favored profiles with mildly retruded lips; the extent of favorable retrusion was greater for women, according to dental students; in their study, the most protrusive lips were the least favored ones. Whether greater for men or women probably depended on the overall effect of facial attractiveness. In another study, Ioi et al. [21] compared the opinions of Korean with Japanese dental students on acceptability of lip prominence, observing that both Korean and Japanese students favored slightly more retruded lips for both males and especially females. Their findings were in contrast to the present study in terms of males but agreed with our results in terms of female lips. Also, our findings were consistent with the results of Arpino et al. [31] who found that orthodontists had understandably a wider range for acceptability than surgeons, probably because orthodontic treatment is spread over several years while surgery is immediate with shorter time for changes to be observed. Miner et al. [20] (who surveyed the perception of young patients and their mothers towards the profile convexity and lip prominence of a series of digitally created images) asserted that mothers preferred more protrusive mandibles, while children preferred more prominent mandibles and original upper lips. McKoy-White et al. [19] studied perception of orthodontists and women and found that white orthodontists favored flatter profiles than did the African-American women, and that African-American women favored fuller profiles compared to African-American orthodontists. Magnitudes of the ZA were not significantly different between these groups.
The current study showed for the first time that the side of the test subject’s face can affect the perception of beauty by the judges; when the test subjects looked to the right and their right side of faces were visible, raters tended to regard a broader range of facial convexities as esthetically acceptable. On the other hand, judges looking at the left side of test faces would become more accurate; the judges also tended to prefer less convex profiles when the test subjects looked to the left and their left side of faces were displayed. All orthodontic studies to date have evaluated the standard cephalometric/photographic direction of test subjects’ faces used in clinics and textbooks, when assessing their profile attractiveness. Therefore, further comparisons and discussions are not possible. Still, the increased accuracy when looking at leftward profiles might be explained by the left-lateralized attention of human due to the visuospatial dominance of the right brain hemisphere [32, 33]. Future studies should also assess this newly found important factor in terms of other profile parameters. If face sidedness was found to matter for many parameters, it can have important clinical and research implications and should be taken into account in future practice.
Controversy exists over findings regarding esthetic lip positions probably because of the multifactorial nature of the notion of beauty being affected by numerous factors such as ethnicity, culture, and gender of test subjects and referees [1,2,3,4,5,6,7,8,9,10]. A proper parameter for assessing the lips’ esthetics is Ricketts E-plane [4, 7, 24, 34]. According to some authors, the lips should be posterior to the E-plane [6, 24, 35]. Even so, full lips together with small noses can be desirable [3,4,5, 7, 24, 25, 35,36,37]. In women, freshness and youth are implied by more convex profiles and fuller lips and therefore these would be preferable [4, 5, 24]. Such profiles may also be preferred for men, because of the influence of fashion magazines or other media [5, 37]; however, some studies suggest that in males, flatter profiles with retruded lips are preferred [4, 24, 25, 34, 38].
This study was limited by some factors. The concept of beauty is subjective and cannot be easily generalized from one population to another [3,4,5,6,7, 23, 24, 37, 38] although according to some authors, it can be universal [39]. However, if the ethnicity and culture could affect the generalizability, this would remain a limitation of all other studies; this would also be less important than before, now that many populations are mixtures of different ethnocultural groups. Another point is that patients usually know their own full faces as seen in the mirror, but orthodontists and surgeons base their diagnosis and treatment mostly on profiles [40, 41]. It was better to have some of the judges repeat their rating after some time, in order to be able to assess intrarater agreements. Still, the internal consistencies of the test image sets calculated based on the inter-rater scores of male + female test profiles were acceptable. An additional limitation of the study was the sample size of judges and subjects which should have been predetermined based on pilot studies and power calculations. Still, this was probably the largest sample in the literature and sufficed to provide numerous significant results. Furthermore, the lack of randomization of image sets within the survey webpage as well as the lack of standardizing the assessment time might reduce the reliability. As well, the screens on which the judges selected the acceptable images were not standardized. These however could improve the generalizability of the results, since not all clinicians or patients use the same screen resolution and brightness or the same evaluation times to assess facial esthetics. Another point is other facial features except the study variables, such as forehead contour and hairstyle that might affect esthetics. However, in this study, esthetic comparisons were not made between different test subjects who had different clothing or facial features. Comparisons were done within each test subject (across 9 similar images of that subject), who had the same appearances with the only changing variable being the one digitally edited by the authors. Therefore, other facial or clothing features would not bias the intra-individual esthetic evaluations. Such studies have been conducted before as well [19,20,21,22]. Some other studies had used silhouettes in order to ensure that facial features would not bias the judgment of facial profile [2]; on the other hand, silhouettes might disallow gender recognition and may not relate to clinical conditions where clinicians or patients assess patients’ pre- and post-treatment profile photographs and not their silhouettes; besides, we used different subjects in order to reduce the biasing effects of facial features. In this study, we designed series of controlled modifications in order to standardize the photogrammetric stimuli within each set as the independent variables. Although this was needed for the sake of reliability, it was not easily generalizable to clinical conditions, where the lip position or facial convexity might not usually change in isolation. It can be argued that for reliable assessment of face sides, each face should have been mirrored. However, we believe that mirroring only half of faces could yield reliable results if selected randomly and analyzed properly. Our multivariable analyses confirmed that the sidedness of face does matter, controlling for other variables. Finally, the number of males was considerably greater than females among orthodontists and surgeons, due to relative unavailability of female practitioners in these specialties. This can limit the reliability of those statistical comparisons performed between male and female judges within each of these two profession groups. Nevertheless, it was not our intention to compare the opinions of male and female judges separately within each of these profession groups. Instead, we assessed if there were significant differences between esthetic judgements of males and females, regardless of judges’ profession, in the whole sample (which was rather balanced in terms of sex, i.e., n = 28 female and 36 male judges; Tables 7 and 8). Afterwards, we conducted more advanced statistics to evaluate the role of judges’ sex on their judgment, controlling for their profession (Table 10). Both of these analyses confirmed that despite the large samples of esthetic evaluations done by males and females (and the proper powers resulted), esthetic preferences of males and females were close to each other (all p values > 0.1 and most of them > 0.5, Tables 7, 8, and 10). Furthermore, we did not limit ourselves to hypothesis testing; we provided effect size measures as well which demonstrated the closeness of esthetic perceptions of male judges to those of female judges.
This study had some advantages. Its sample size and its number of null hypotheses were unique to the literature. Most importantly, it is the first study ever suggesting that the direction of faces of patients on profile photographs might affect the esthetic preferences of a practitioner. This means that perhaps assessing exclusively profiles of the right side of the face is not the best practice. If further studies report that many other esthetic parameters are as well affected by laterality, perhaps current esthetic assessments in which the patient looks only to the right should be reconsidered.
Conclusions
Within the limitations of this study, it was concluded that Iranian orthodontists, maxillofacial surgeons, and laypeople unanimously preferred lips slightly anterior to the Ricketts norm in men, with test women, surgeons, laypeople, and orthodontists preferring slightly protruded lips, normal lips, and retruded lips, respectively. All groups preferred profiles slightly less convex than the Legan-Burstone norm for men and women. Orthodontists had the broadest zones of acceptability, while surgeons had the narrowest zones; laypeople had ZAs between these two other groups.
Male and female judges rated profiles similarly for every parameter of facial convexity and lip prominence.
Female test subjects may have a wider zone of acceptability compared to males, in terms of facial convexity. The esthetic optimum points (ZA midpoints) for convexity angles of both men and women were less convex than the norm. For lip prominence, esthetic male subjects have protruded lower and higher limits of the ZA than do females, as well as more protruded midpoints. An esthetic lower lip would be more protruded than the norm in men, but would be similar to the norm in women.
Interestingly, it was shown for the first time in the whole literature that the side of the test face also influences the perception of beauty: when the test subjects’ profiles look to the left (and their left side of face is visible), judges may prefer less convex profiles compared to when the right side of the face is visible. Also judges’ esthetic tolerance reduces and their accuracy increases (i.e., the convexity ZA narrows down) when looking at the left side of the test face. Future studies of these preliminary observations are warranted.
References
Massad JJ (1999) A perspective on dental beauty. Dent Today 18:46–49
Sodagar A, Borujeni DG (2013) Evaluation of anteroposterior lip positions in the most-favored iranian facial profiles using silhouette. J Dent (Tehran, Iran) 10:393–404
Berneburg M, Dietz K, Niederle C, Goz G (2010) Changes in esthetic standards since 1940. Am J Orthod Dentofac Orthop 137(450):e1–e9 discussion −1
Matoula S, Pancherz H (2006) Skeletofacial morphology of attractive and nonattractive faces. Angle Orthod 76:204–210
Nguyen DD, Turley PK (1998) Changes in the Caucasian male facial profile as depicted in fashion magazines during the twentieth century. Am J Orthod Dentofac Orthop 114:208–217
Nomura M, Motegi E, Hatch JP, Gakunga PT, Ng'ang'a PM, Rugh JD et al (2009) Esthetic preferences of European American, Hispanic American, Japanese, and African judges for soft-tissue profiles. Am J Orthod Dentofac Orthop 135:S87–S95
Khosravanifard B, Rakhshan V, Raeesi E (2013) Factors influencing attractiveness of soft tissue profile. Oral Surg Oral Med Oral Pathol Oral Radiol 115:29–37
Cox NH, van der Linden FPGM (1971) Facial harmony. Am J Orthod 60:175–183
Cross JF, Cross J (1971) Age, sex, race, and the perception of facial beauty. Dev Psychol 5:433–439
Martin JG (1964) Racial ethnocentrism and judgment of beauty. J Soc Psychol 63:59–63
Hickman L, Firestone AR, Beck FM, Speer S (2010) Eye fixations when viewing faces. J Am Dent Assoc 141:40–46
Giddon DB (1995) Orthodontic applications of psychological and perceptual studies of facial esthetics. Semin Orthod 1:82–93
Shimomura T, Ioi H, Nakata S, Counts AL (2011) Evaluation of well-balanced lip position by Japanese orthodontic patients. Am J Orthod Dentofac Orthop 139:e291–e2e7
Schlosser JB, Preston CB, Lampasso J (2005) The effects of computer-aided anteroposterior maxillary incisor movement on ratings of facial attractiveness. Am J Orthod Dentofac Orthop 127:17–24
Celebi AA, Tan E, Gelgor IE, Colak T, Ayyildiz E (2013) Comparison of soft tissue cephalometric norms between Turkish and European-American adults. Sci World J 2013:806203
Hassebrauck M (1998) The visual process method: a new method to study physical attractiveness. Evol Hum Behav 19:111–123
Sukhia RH, Khan M, Fida M, Shaikh A, Azam SI (2011) Esthetic preferences for facial soft tissue profiles. Int J Orthod Milwaukee 22:17–23
Naini FB, Donaldson ANA, McDonald F, Cobourne MT (2012) Assessing the influence of chin prominence on perceived attractiveness in the orthognathic patient, clinician and layperson. Int J Oral Maxillofac Surg 41:839–846
McKoy-White J, Evans CA, Viana G, Anderson NK, Giddon DB (2006) Facial profile preferences of black women before and after orthodontic treatment. Am J Orthod Dentofac Orthop 129:17–23
Miner RM, Anderson NK, Evans CA, Giddon DB (2007) The perception of children’s computer-imaged facial profiles by patients, mothers and clinicians. Angle Orthod 77:1034–1039
Ioi H, Shimomura T, Nakata S, Nakasima A, Counts AL (2008) Comparison of anteroposterior lip positions of the most-favored facial profiles of Korean and Japanese people. Am J Orthod Dentofac Orthop 134:490–495
Ioi H, Nakata S, Nakasima A, Counts AL (2005) Anteroposterior lip positions of the most-favored Japanese facial profiles. Am J Orthod Dentofac Orthop 128:206–211
Mantzikos T (1998) Esthetic soft tissue profile preferences among the Japanese population. Am J Orthod Dentofac Orthop 114:1–7
Ghorbanyjavadpour F, Rakhshan V (2019) Factors associated with the beauty of soft-tissue profile. Am J Orthod Dentofacial Orthop 155:832–843
Erbay EF, Caniklioglu CM (2002) Soft tissue profile in Anatolian Turkish adults: part II. Comparison of different soft tissue analyses in the evaluation of beauty. Am J Orthod Dentofac Orthop 121:65–72
Ricketts RM (1957) Planning treatment on the basis of the facial pattern and an estimate of its growth. Angle Orthod 27:14–37
Legan HL, Burstone CJ (1980) Soft tissue cephalometric analysis for orthognathic surgery. J Oral Surg 38:744–751
Jacobson A, Jacobson RL (2007) Radiographic cephalometry: from basics to 3-D imaging, 2nd edn. Quintessence, Hanover Park, IL
Spyropoulos MN, Halazonetis DJ (2001) Significance of the soft tissue profile on facial esthetics. Am J Orthod Dentofac Orthop 119:464–471
Romani KL, Agahi F, Nanda R, Zernik JH (1993) Evaluation of horizontal and vertical differences in facial profiles by orthodontists and lay people. Angle Orthod 63:175–182
Arpino VJ, Giddon DB, BeGole EA, Evans CA (1998) Presurgical profile preferences of patients and clinicians. Am J Orthod Dentofac Orthop 114:631–637
Nicholls ME, Loftus A, Mayer K, Mattingley JB (2007) Things that go bump in the right: the effect of unimanual activity on rightward collisions. Neuropsychologia 45:1122–1126
Pisella L, Alahyane N, Blangero A, Thery F, Blanc S, Pelisson D (2011) Right-hemispheric dominance for visual remapping in humans. Philos Trans R Soc Lond Ser B Biol Sci 366:572–585
Czarnecki ST, Nanda RS, Currier GF (1993) Perceptions of a balanced facial profile. Am J Orthod Dentofac Orthop 104:180–187
Lew KK, Ho KK, Keng SB, Ho KH (1992) Soft-tissue cephalometric norms in Chinese adults with esthetic facial profiles. J Oral Maxillofac Surg 50:1184–1189 discussion 9-90
Peck H, Peck S (1970) A concept of facial esthetics. Angle Orthod 40:284–318
Sforza C, Laino A, D'Alessio R, Grandi G, Tartaglia GM, Ferrario VF (2008) Soft-tissue facial characteristics of attractive and normal adolescent boys and girls. Angle Orthod 78:799–807
Turkkahraman H, Gokalp H (2004) Facial profile preferences among various layers of Turkish population. Angle Orthod 74:640–647
Jones D, Hill K (1993) Criteria of facial attractiveness in five populations. Hum Nat 4:271–296
Hemmatpour S, Kadkhodaei Oliadarani F, Hasani A, Rakhshan V (2016) Frontal-view nasolabial soft tissue alterations after bimaxillary orthognathic surgery in class III patients. J Orofac Orthop 77:400–408
Hershon LE, Giddon DB (1980) Determinants of facial profile self-perception. Am J Orthod 78:279–295
Acknowledgments
The authors express their sincere gratitude to Prof. Donald B. Giddon for his in-depth review of the methods, statistics, and article as well as his extensive contributions and edit to the text.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
All procedures were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments.
Informed consent
Informed consent was obtained from orthodontic patients.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mousavi, S.M., Saeidi Ghorani, P., Deilamani, A. et al. Effects of laterality on esthetic preferences of orthodontists, maxillofacial surgeons, and laypeople regarding the lip position and facial convexity: a psychometric clinical trial. Oral Maxillofac Surg 23, 439–451 (2019). https://doi.org/10.1007/s10006-019-00795-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10006-019-00795-w