
Abstract
This longitudinal study examined the long-term effects of the COVID-19 pandemic on social media use and its impact on psychiatric symptoms and well-being of 3,697 Israeli children and adolescents aged 8 to 14. Data were collected from October 2019 to June 2023, covering four school years and five measurement points prior to, throughout and post- COVID-19. Social media usage, psychiatric symptoms (depression, anxiety, somatization, and general distress), as well as subjective well-being (positive and negative emotions, and life satisfaction) were assessed. The analysis also probed the extent to which social support and extracurricular activities moderated the associations between social media use and mental health outcomes. The results of the growth mixed-effects models indicated a significant increase in social media use and psychiatric symptoms, and a significant decrease in subjective well-being over time. Greater social media use was related to more psychiatric symptoms and negative emotions, but also to more positive emotions and life satisfaction. Social support buffered the negative effects of excessive social media use on mental health, whereas extracurricular activities increased positive emotions, but also psychiatric symptoms related to social media use. These findings highlight the need for targeted interventions to regulate social media usage, given its lasting consequences on the mental health of children and adolescents in the wake of the COVID-19 pandemic.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Social media has dramatically changed how children and teens communicate with each other. Traditional playgrounds have been replaced by virtual spaces like Instagram and TikTok, where children and adolescents share their daily experiences through photos and videos, consume content, and express their opinions [1]. Despite this shift in the landscape of social interactions, the reasons for using social media platforms remain similar to traditional forms of communication in that they primarily provide a space for children and teens to interact, meet new friends, make plans, and express themselves [2].
This need for social connections was starkly reflected in the marked increase in social media use during the COVID-19 period. As conventional social spaces such as schools and parks became inaccessible, virtual spaces emerged as the primary social channels for children and adolescents. This trend persisted throughout the different waves and lockdowns of the pandemic as children and adolescents sought to maintain their ties with friends amidst clampdowns on face-to-face interactions [3].
Studies have linked the increase in social media use to reduced sleep quality [4], symptoms of depression, anxiety, psychological distress [5,6,7], and decreased happiness in adolescents [8]. Estimates indicate a prevalence rate of 15.1% for problematic social media use during the COVID-19 pandemic [9]. The global crisis aggravated the negative effects of increased social media use on mental health. Analyses suggest that the enforcement of lockdowns and social distancing measures led many adolescents to experience heightened feelings of isolation and loneliness due to their physical separation from friends, classmates, and extended family members. As a result, many turned to social media as their primary means of maintaining social connections and support-seeking during this period of social upheaval. However, the virtual nature of social media interactions often fell short of fulfilling the deep human need for in-person socialization, thus leading to increased feelings of loneliness, which also exacerbated mental health issues [10].
The COVID-19 pandemic also brought about a constant influx of distressing news updates, leading to uncertainty about the future that was amplified by misinformation circulating on social media platforms. Adolescents, who are already susceptible to heightened levels of anxiety and stress during this developmental period, were bombarded with alarming statistics, conflicting information about the virus, and divisive opinions that all contributed to heightened psychological distress [11]. The blurring of boundaries between school and personal life as a result of remote learning further exacerbated their feelings of being overwhelmed and burned out, as adolescents struggled to find a balance amidst the constant barrage of digital information and demands [12].
The pervasive nature of social media during the pandemic aggravated existing issues such as cyberbullying, online harassment, and negative social comparisons. As adolescents spent more time online, they became more vulnerable to peer pressure, attempts at social validation-seeking behaviors, and the harmful effects of cyberbullying and digital exclusion [13, 14]. Thus, social media, while initially perceived as a means of staying connected and engaged, became a double-edged sword that amplified feelings of inadequacy and disconnection.
Although studies during the pandemic focused on the relationship between social media use and mental health symptoms, there have been few longitudinal studies that trace children’s and adolescents’ social media usage patterns and their long-term mental health effects. Only a small number of studies have investigated whether increased social media use has persisted post-COVID-19, or examined its mental health consequences [15]. Subjective well-being has also attracted scant attention.
In addition, numerous factors can influence how children and adolescents use social media and the ways it affects their mental health. It is important to identify protective factors and understand how they can lead to positive outcomes for young people. The current study focused on extracurricular activities and social support, two well-researched factors that were likely to mitigate the negative consequences of social media use in children and teens during the pandemic but also post-COVID.
Extracurricular activities such as sports, arts, music, clubs, and volunteering have been linked to improved well-being and overall thriving in children and youth [16]. They provide opportunities for physical, social, and cognitive development, academic achievement, and positive social interactions with peers and adult mentors [17]. Recent studies found that team sports reduced anxiety and depression symptoms among adolescents during the pandemic compared to their non-participating peers [18, 19]. Another study showed that teens who engaged in extracurricular activities spent less than two hours on recreational screen time after school and experienced more life satisfaction, optimism, and less anxiety and depression [20].
Recent studies have also highlighted the importance of perceived social support during the COVID-19 pandemic. Children and adolescents who feel loved and valued, particularly during challenging times, and have robust social support— the perceived or actual availability of emotional, informational, or instrumental assistance from significant others —tend to have lower risks for psychological and physical illnesses [21]. Social support was linked to lower levels of depression and PTSD [22] and improved psychological well-being in adolescents [23]. Studies showed that social support from peers, including through social media played a key role in lessening mental health issues during the pandemic period [24, 25].
To address the gaps in the literature regarding the long-term impact of COVID-19 on daily social media use and mental health, this 4-year longitudinal study covering the period from September 2019 to June 2023 recruited a large sample of children and adolescents, aged 8 to 14 at baseline, who were sampled several months before the COVID-19 pandemic outbreak. Their social media usage patterns and psychiatric symptoms were examined along with indicators of well-being such as life satisfaction, and positive emotions across five points in time. The study timeline included three periods of long lockdowns, extended school closures and online learning, followed by a more stable and routine period during the 2021-23 school years. The original longitudinal study was designed pre-pandemic to measure the associations between social media use, mental health, and well-being as a function of socio-demographic and protective factors. The impact of the pandemic rapidly pointed to the value of using the 2019 data as the baseline. This prompted the extension of the study to its four-year format and the reformulation of the original hypotheses.
In the current study, the roles of extracurricular activities and social support as potential protective factors were also probed to better understand how they may buffer the impact of excessive social media use and contribute to better mental health outcomes. Based on previous studies, three hypotheses were formulated:
H1
There will be a significant increase in psychiatric symptoms (depression, anxiety, somatization, and general distress) and significant decreases in subjective well-being (lower positive emotions and life satisfaction, and more negative emotions) over the study period compared to the 2019 baseline level.
H2
There will be a significant interaction between social media daily use and time, such that increased social media use will amplify psychiatric symptoms and diminish well-being.
H3
Social support and extracurricular activities would moderate the decrease in mental health during and after the pandemic, such that children with greater social support and engagement in extracurricular activities will be less influenced by social media use in terms of a reduction in mental health and well-being. The interactions of age and gender with social media use and their mental health consequences were examined in an exploratory fashion.
Method
Participants
At baseline in 2019, the sample consisted of 3,697 children and adolescents aged 8 to 14 years (M = 11.01, SD = 1.99), with a gender distribution of 49.7% girls and 50.3% boys. To ensure representativeness, we employed a stratified random sampling approach. This consisted of defining four strata corresponding to the four main geographic regions of Israel: the North, Center, South, and the Shfela region. Then, eight schools from these different regions in Israel were selected with assistance from the Ministry of Education. Specifically, the Ministry provided a list of 5 primary and 5 secondary schools from each region that were representative of the region’s population, based on school survey data collected by the Ministry of Education. We then randomly selected one elementary and one secondary school from each region using a computer-generated random number. Special education and ultra-orthodox religious schools were excluded, since they have different curricula and student populations than mainstream schools. Within each school, we reached out to all the students in grades 3 to 9 to ask them to participate in the study. We also collected demographic information on the students. Hence, the sample was reflective of the Israeli population in terms of residence, gender, socioeconomic status, and family situation. The baseline characteristics of the participants appear in Table S1 in the online supplemental materials.
Procedure
After receiving approval from the University and municipal ethics committees, an online letter detailing the study and requesting parental consent for their children’s participation was distributed to the students’ parents. Out of the total number of students, 84% obtained written consent from their parents, rendering them eligible for inclusion. On the day of the initial assessment, all eligible students present in school were invited to participate in the study and to provide their written consent beforehand.
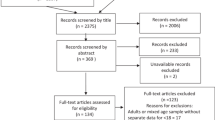
Data collection was conducted across five time points: the initial assessment took place before the COVID-19 pandemic in October 2019 (N = 3,697), followed by assessments after the first lockdown in Israel in June 2020 (N = 3,598), then after the two subsequent lockdowns in June 2021 (N = 3,364), then during the fifth pandemic wave in June 2022 (N = 3,454), and finally at the end of the school year in June 2023 (N = 3,596). In total, 97.3% of the original sample completed one or more follow-up surveys. Over the time points, 74 students left the school, 17 declined to participate, and the rest were absent from school or excluded due to incomplete data. The study participant flow diagram is presented in Fig. 1. After providing their written consent, the students received a survey link ensuring their anonymity by attributing a code number for the longitudinal follow-ups. All participants completed the questionnaires during the school day, using tablets and the Qualtrics platform. The questionnaires were consistently administered across all measurement points.

Participant flow diagram
Measures
Social Media Use [26]. The participants’ daily social media usage during typical weekdays was evaluated on a questionnaire probing their time spent on various social media platforms; i.e., “On an average weekday, how much time (in minutes/hours) do you spend on social networking, messaging sites, or Apps across platforms like YouTube, Instagram, TikTok, Facebook, Snapchat, Twitter, WhatsApp, and other social media platforms?”. The total usage time was calculated by aggregating the durations for each platform.
The Brief Symptom Inventory 18 [27] is a self-report scale composed of 18 psychiatric symptom items that are rated on a 4-point Likert scale from 0 (not at all) to 4 (very much) and refer to the previous month. The inventory covers three primary symptom subscales: Anxiety, Somatization, and Depression, and a Global Severity Index (GSI), which is the sum of the ratings of distress on each item. The scores on the BSI-18 range from 0 to 72, with higher scores reflecting more psychological distress. Example items are “Feeling weak in parts of your body” (Somatization); “Feeling hopeless about the future” (Depression), and “Feeling tense or keyed up” (Anxiety). The internal consistency reliability estimates were derived from a community sample. The alpha coefficients for Somatization, Depression, Anxiety, and GSI were 0.74, 0.84, 0.79, and 0.89, respectively, which are satisfactory. The construct validity of the BSI 18 was evaluated by correlating the Somatization, Depression, Anxiety, and GSI scores with the corresponding scores on the Symptom Check-List-90-R. The correlations were high, from 0.91 for Somatization to 0.96 for Anxiety (Depression and GSI were both 0.93 [27]. The Cronbach’s Alpha coefficients for the total scale in the current study ranged from 0.80 to 0.87 across the five measurement points.
The Brief Multidimensional Students’ Life Satisfaction Scale [28] is a self-report measure for children and adolescents that evaluates life satisfaction in different life domains. It consists of five items rated on a 7-point scale ranging from 1 (terrible) to 7 (delighted). The items are averaged to create a general life satisfaction score. The total scores range from 1 to 7, with higher scores indicating more life satisfaction. Each item measures life satisfaction in one of the following five areas: satisfaction with friendships, family life, school experience, where one lives, and oneself. Example items include “I am satisfied with my family life”, “I am satisfied with my friendships”, and “I am satisfied with myself”.
The BMSLSS was shown to be internally consistent (α = 0.75) and valid for early adolescence. It was reported to correlate well with other life satisfaction scales (r = .66 with the Multidimensional Students’ Life Satisfaction Scale - MSLSS and r = .62 with the Students’ Life Satisfaction Scale - SLSS) [28]. The scale had good internal consistency in the current study (α = 0.82 to 0.88).
The Positive and Negative Affect Schedule for Children [29] is a self-report measure designed for children and adolescents to assess levels of positive and negative affect over the previous month. It comprises 10 items composed of five positive emotions (e.g., enthusiastic, proud, excited) and five negative emotions (e.g., afraid, upset, nervous). Responses are rated on a 5-point scale ranging from 1 (very slightly or not at all) to 5 (extremely). The positive affect and negative affect scores are calculated by summing individual items. Scores range from 5 to 25. The negative affect and positive affect scales have shown high internal consistency reliability, with values of 0.82 and 0.86 respectively, for school age children. The scales have also demonstrated construct validity, by differentiating between different diagnostic groups [29]. In the current study, the alpha coefficients were 0.79 to 0.84 for the positive affect subscale and 0.77 to 0.81 for the negative affect subscale.
Perceived Social Support. Participants completed a 4-item subscale from the Multidimensional Scale of Perceived Social Support [30], which measures children’s and teens’ perceptions of their peers as providers of support. Example items include “My friends really try to help me”, and “I have friends with whom I can share my joys and sorrows”. Items are rated on a Likert scale from 1 (strongly disagree) to 5 (strongly agree) and are averaged to derive a peer support score that ranges from 1 to 5. The Cronbach’s alpha for the Friends subscale was 0.85. The construct validity of the subscale was found to be good, as it negatively related to depression symptoms (r = -.24). The Cronbach’s Alpha coefficients in this study ranged from 0.84 to 0.91.
The Extracurricular Activities Measure [31], is a 26-item questionnaire that assesses involvement in various activities, encompassing sports and physical activities, the arts and creative pursuits, academic and educational activities, leadership and youth movements, community service and volunteering, outdoor and nature activities, as well as life skills and personal development courses. Activities are rated on a scale ranging from 0 (not engaging in the activity) to 4 (engaging in the activity five or more times per week) to indicate level of involvement. The scores from these items are averaged to calculate a total score that ranges from 0 to 4. Concurrent validity analyses have demonstrated that the measure exhibits the expected associations across various constructs relevant to adolescent development including environmental support, well-being, and internalizing symptoms. The Cronbach’s Alpha coefficients in the current study ranged from 0.75 to 0.79.
Statistical analysis
The baseline measures were summarized using descriptive statistics. Missing data comprised 3.4% of the total dataset, mainly due to item nonresponses. Missing data were handled using multiple imputation with IBM SPSS V.28., a method that generates plausible values for missing values, thus creating several “complete” sets of data. We imputed 20 datasets, which was a sufficient number to obtain valid and stable estimates.
Growth mixed-effects regression models were employed to analyze the changes in psychiatric symptoms and subjective well-being measures from baseline to June 2023. Trend analyses were conducted using SPSS version 28.0. Trend analyses revealed linear changes in mental health symptoms and negative emotions, whereas positive emotions and life satisfaction demonstrated quadratic changes. For this reason, we added a quadratic term in the growth mixed-effects regression models of positive emotions and life satisfaction to capture the possible nonlinear changes in these outcome variables over time. A quadratic term allows the slope to vary depending on the value of time, which can reflect the acceleration or deceleration of the growth rate.
The growth curves, with the intercept and slope as parameters, were used to illustrate the growth patterns of the outcome variables as a linear or quadratic function of time. The intercept in the Level 1 equation represented the baseline level of the outcome variables, whereas the slope indicated changes in these variables from baseline at the five measurement points.
The level 1 models assessed the growth trajectories for the outcome measures based on Time indicating the number of school years since baseline, as well as social media use and its interaction with Time that captured within-person changes. The moderating role of social support and extracurricular activities in the relationship between social media use and mental health outcomes over time was examined through their interaction with social media use. Social media use, social support, and extracurricular activities were measured at each of the five measurement points. In the quadratic models, the linear change in outcomes was indicated by the Time factor, whereas the quadratic change over time was described by the Time2 factor at Level 1.
The level-2 models estimated the effect of age and gender on mental health outcomes, along with their interaction with social media use. Gender was represented as a dummy variable, and age at baseline was centered on the sample mean. This approach enabled us to probe how changes in social media use over time correlated with changes in mental health outcomes, while also examining how gender and age influenced this relationship. No other demographic variables emerged as significant predictors. School effects were not significant and only contributed 1- 2% of the observed variation, and were consequently excluded from the final models, as is customary [32].
Results
Descriptive statistics
The distribution of variables was assessed for normality and indicated no evidence of excessive skewness or kurtosis. The descriptive statistics and bivariate correlations of the variables at baseline are shown in Table S2 in the online supplemental materials.
Table 1 displays the mean ratings and standard deviations of the variables across the five measurement points. The participants, on average, used social media platforms for approximately 2.67 h per day (SD = 2.21) at baseline. At the beginning of the study, there were significant differences in social media use as a function of SES and family background. Middle SES children used social media less (M = 2.60, SD = 2.16, ps < 0.04) than high SES children (M = 2.79, SD = 2.30) and low SES children (M = 2.84, SD = 2.24), F(2, 3694) = 3.87, p = .02, partial η2 = 0.01. Children with married parents also used social media less (M = 2.61, SD = 2.18, ps < 0.005) than those with divorced (M = 2.89, SD = 2.26) or unmarried parents (M = 3.44, SD = 2.48), F(3, 3693) = 9.59, p < .001, partial η2 = 0.01. However, there were no significant differences in screen overuse across SES or family background groups.
Of the participants, 10.7% reported using social media for 6 h or more per day at baseline. At the end of the study, the average daily usage of social media increased to 3.14 h (SD = 2.14), and 15.5% of the participants were online for 6 h or more per day. Twelve- to 14-year-olds used social media for an average of 2.87 h per day (SD = 2.15) at baseline. By the end of the study, the average social media use of 12 to 14 year olds had risen significantly to 3.17 h per day (SD = 2.16, p < .001).
The increase in social media use in the total sample (Cohen’s d =-0.22) was accompanied by significant increases in depression, anxiety, somatization, and negative emotions, and significant decreases in social support, extracurricular activities, and life satisfaction. The effect sizes of these changes ranged from small to moderate, with the largest effects observed for negative emotions (Cohen’s d=-0.58), anxiety (Cohen’s d=-0.53), and depression (Cohen’s d=-0.49).
Among 12- to 14-year-olds, psychiatric symptoms measured by the Global Severity Index (GSI) increased significantly from the baseline (M = 16.62, SD = 11.05) to the first lockdown (M = 18.53, SD = 12.56, t = 4.43, p < .001). No significant changes were noted in subsequent measurements, with GSI scores of 18.73 (SD = 12.69, t = 0.43, p = .67) and 19.47 (SD = 15.63, t = 1.42, p = .15). By the end of the study, the average GSI had significantly increased to 22.93 (SD = 15.07, t = 13.31, p < .001; Cohen’s d=-0.48).
Longitudinal analyses of social media use and mental health
Longitudinal Growth Models were utilized to assess changes in mental health symptoms and subjective well-being over the study period as compared to the baseline assessment. The changes in social media use, mental health symptoms, and subjective well-being over the study period are presented in Fig. 2.

Trends in (a) social media usage, (b) psychiatric symptoms, (c) emotional well-being, and (d) life satisfaction across the five measurement points
Tables 2 and 3 detail the estimated fixed-effect coefficients for the regression models. The intra-class correlation coefficients (ICCs) ranged from 0.01 to 0.26, suggesting limited within-person stability in psychiatric symptoms and subjective well-being. These findings imply that year-to-year fluctuations rather than stable individual differences accounted for most of the outcome variability.
Positive coefficients for the linear slope parameter (time) were observed in the unconditional linear growth models for depression (b = 0.53, 95% CI [0.48, 0.58]), anxiety (b = 0.50, 95% CI [0.46, 0.55]), somatization (b = 0.48, 95% CI [0.44, 0.53]), and the GSI (b = 1.53, 95% CI [1.41, 1.64]), indicating a significant increase in these symptoms over the study period, and validating H1 (see Table 2). For the measures of subjective well-being, negative emotions exhibited a linear increase, (b = 0.65, 95% CI [0.62, 0.69]), whereas positive emotions (b = 0.43, 95% CI [0.40, 0.47]), and life satisfaction (b = 0.13, 95% CI [0.11, 0.14]) followed a quadratic pattern (see Table 3). There was a significant drop in positive emotions and life satisfaction from baseline to the second measurement point (after the first COVID-19 lockdown), followed by a gradual increase from the third to the fifth measurement points (see Fig. 2).
To test the second hypothesis, the impact of social media daily use and its interaction with time on psychiatric symptoms and subjective well-being was explored. A significant interaction effect was observed for social media use and time, indicating that increased social media usage was linked to increased psychiatric symptoms over time, including anxiety (b = 0.03, 95% CI [0.01, 0.06]), somatization (b = 0.06, 95% CI [0.04, 0.08]), and the GSI (b = 0.07, 95% CI [0.01, 0.12]) (see Table 2). Disconfirming the second hypothesis, higher levels of social media use were also correlated with heightened positive emotions (b = 0.24, 95% CI [0.17, 0.31]), and life satisfaction (b = 0.06, 95% CI [0.02, 0.08]) (see Table 3).
The interaction between social media use and social support displayed significant associations across all mental health indicators, including the GSI (b = -0.22, 95% CI [-0.30, -0.13]), depression (b = -0.09, 95% CI [-0.12, -0.05]), anxiety (b = -0.08, 95% CI [-0.12, -0.05]), and somatization (b = -0.04, 95% CI [-0.08, -0.01]) (see Table 2), as well as negative emotions (b = -0.07, 95% CI [-0.09, -0.04]; Table 3). This suggests a moderating effect where higher levels of social support alleviated the adverse impact of increased social media use on psychiatric symptoms and negative affect, confirming the third hypothesis.
However, the third hypothesis predicting an interaction between social media use and extracurricular activities was partially confirmed. Children and adolescents who engaged in a high number of extracurricular activities exhibited more substantial increases in positive emotions related to their social media use (b = 0.05, 95% CI [0.01, 0.09]) compared to those with lower extracurricular involvement. However, these same individuals also displayed a more pronounced rise in symptoms of general distress (b = 0.16, 95% CI [0.05, 0.27]), depression (b = 0.05, 95% CI [0.01, 0.10]), and somatization (b = 0.12, 95% CI [0.08, 0.16]) related to their social media use.
Age moderated the relationship between social media use and somatization, with steeper increases in somatization symptoms in older children and adolescents (b = 0.02, 95% CI [0.01, 0.04]). The significant social media use × gender interaction showed a more pronounced impact of social media daily use on psychiatric symptoms of depression (b = -0.12, 95% CI [-0.19, -0.06]), anxiety (b = -0.10, 95% CI [-0.17, -0.04]), somatization (b = -0.11, 95% CI [-0.17, -0.04]), and general distress (b = -0.34, 95% CI [-0.50, -0.17]), and lower life satisfaction (b = -0.02, 95% CI [-0.04, -0.01]) in girls as compared to boys.
Discussion
The result of this study showed that children and adolescents increased their social media use during and after the pandemic, both in terms of average hours and the proportion of heavy users. By the end of the study, the average daily social media usage had increased to approximately 3.14 h, and the percentage of participants online for 6 h or more had risen to 15.5%. These usage figures considerably exceed levels seen among adolescents before and during the COVID-19 period [33, 34]. This suggests that social media use may have become more habitual or addictive for young people, especially after the COVID-19 pandemic.
This study also examined whether changes in social media use over time were linked to age or to a change in social media behavior. To do so, data on older children at the outset of the study were compared to data for same-age children at the conclusion of the study. The results showed that the average daily social media use in 12–14-year-olds rose significantly from 2.87 h to 3.17 h. This suggests that the increase in usage was not simply a natural effect of aging, but an indication of changing social media habits during the study period. The effects of this change were small in terms of Cohen’s d and went from 0.14 for the 12–14 age group to 0.22 for the whole sample.
Throughout the study period, psychiatric symptoms increased significantly, and subjective well-being declined, as is evident in the reports of fewer positive emotions and more negative emotions as well as reduced life satisfaction. The observation that in 2023, at the end of the pandemic, the participants exhibited the highest levels of symptoms and the lowest level of well-being, paints a concerning picture of the pandemic’s lasting effects on the younger generation. The baseline Global Severity Index (GSI) score, which measured the intensity of psychological distress and psychiatric symptoms, was 16.20 (SD = 10.90). This score is indicative of moderate psychological distress among the students at the beginning of the study, according to the BSI Israeli norms for adolescents (M = 15.66, SD = 11.52) [35]. However, by the end of the study period, distress levels had worsened significantly, with a GSI score of 23.76 (SD = 15.56), compared to the Israeli norms [35] and previous studies that administered the Brief Symptom Inventory before the pandemic [36, 37].
The observed increase in the GSI among 12- to 14-year-olds from the baseline to the first lockdown is noteworthy. The significant rise from an average of 16.62 to 18.53 post-lockdown suggests a marked escalation in psychiatric symptoms coinciding with the onset of pandemic restrictions. This initial surge aligns with broader concerns about the mental health impacts of COVID-19 lockdowns, particularly among adolescents who are at a critical stage of social and psychological development. In addition, the significant increase in GSI scores to 22.93 by the end of the study cannot be overlooked. It underscores a gradual but persistent exacerbation of psychiatric symptoms over the course of the pandemic, which may reflect the cumulative stress and disruption experienced by adolescents during this period. The effect size (Cohen’s d =-0.48) further substantiates the substantial impact of the pandemic on adolescent mental health, beyond what might be expected from normal developmental changes. These findings necessitate a deeper exploration of long-term mental health strategies to support adolescents, as they highlight the profound and enduring effects of the pandemic on this vulnerable age group.
This mental health deterioration may have partly been caused by the closure and disruption of the education system during the COVID-19 period. The education system in Israel faced major challenges in the 2019/20 and 2020/21 school years, since schools applied a rotational system between online and hybrid learning modes depending on grade level. For instance, students in grades 5–12 spent most of their time learning online (about 75%), and only a few hours in person in small groups per week. This change in learning mode posed numerous difficulties for both students and teachers who lacked the necessary infrastructure, support, skills, or confidence to adapt to this new situation. As a result, students missed many days of in-person instruction (about 15% of the school year due to the first lockdown in 2020), and the education system did not ever operate at full capacity for any age group in the second school year in 2021 [38].
This situation contrasts with most OECD countries, where schools were fully open for about 60% of the academic year, fully closed for about 15%, and partially open for about 25% [39]. This disruption had a negative impact on student achievement, as indicated in a survey by the Israel National Authority for Measurement and Evaluation in Education, which showed that only 37% of all teachers and 40% of all parents thought that the education system had covered the curriculum during periods of distance learning [40].
Contrary to assumptions that the reopening of the economy and the education system in March 2021 in Israel would improve the mental health of children and adolescents, psychiatric symptoms continued to rise even after schools returned to full routine, and reached a peak at the last measurement point in June 2023. This suggests that the closure and disruption of the education system had long-term effects on the mental health of the younger generation. Children and adolescents in Israel also faced other sources of stress and pressure, such as political instability, the social unrest due to the ongoing Israeli-Palestinian conflict, four rounds of elections in two years, an economic crisis, a sharp decline in the income of Israeli citizens, and inflation after the pandemic [38], which peaked in 2023.
It is important to note that Israeli children presented with high levels of mental distress even before the COVID-19 pandemic. In the past decade, mental health problems among children and adolescents in Israel has increased significantly, especially in terms of anxiety-related symptoms and depression [41]. This trend has also been observed around the world, and studies over the last 10 years have linked mental health problems in preteens and teens to the impact of increased screen time and social media use on teens’ social life [42]. Social media has become a dominant feature of adolescents’ lives in Israel, with 95% of all Israeli teens aged 13 to 17 using platforms such as Instagram, Snapchat, Facebook, and YouTube. In addition, 15.3% of all Israeli adolescents were classified as problematic social media users in 2019, compared to only 4.3% in 2017 [43].
The mental health situation of Israeli children has also been undermined by the ongoing Israeli-Palestinian conflict, which exposes them to constant violence and trauma. Israeli youth present much higher levels of mental health symptoms than the global average, according to the GSI total score on the BSI [35, 44]. A study that monitored Israeli adolescents for 14 years found that they had a high rate of severe psychiatric and post-traumatic stress symptoms [45]. Thus, the COVID-19 pandemic may have added more stress to the already vulnerable mental health of Israeli preteens and teens.
The first lockdown in Israel had a negative impact on the subjective well-being of children and adolescents, since it reduced their life satisfaction and positive emotions. This could be attributed to the disruption of their normal lifestyle, such as the school closures, the suspension of extracurricular activities, and the curtailment of social interactions with friends. However, these scores improved during the subsequent measurement points, indicating a possible adaptation to the situation along with the partial resumption of routine and hybrid learning in schools. On the other hand, negative emotions showed a different pattern: they decreased after the first lockdown, which may have lifted some of the academic and social pressure on children, but increased later on as the pandemic persisted, the lockdowns repeated themselves (Israel experienced three lockdowns of more than a month each), and the challenges of coping with educational and social gaps intensified.
This study investigated how social media use affected various aspects of mental health in children and adolescents during the long-lasting pandemic. The results suggest that social media usage had both positive and negative effects on their emotional well-being. On one hand, the students who used social networks more often reported more positive emotions and life satisfaction than those who used them less often. On the other hand, the results also exposed the “dark side” of social media use, since the children and adolescents who spent more time on these platforms experienced more symptoms such as anxiety, somatization, and distress. While this study did not examine how different aspects of social media use (such as active or passive use, or the quality of interactions) related to mental health outcomes, previous research suggests some possible explanations for these associations.
Specifically, a number of studies have underscored the positive aspects of social media during the pandemic, particularly in managing anxiety and loneliness when in-person interactions were restricted [46, 47]. During lockdowns, social media played a crucial role in maintaining essential social connections. A multi-country study involving 5,114 adolescents found that over 40% increased their social media use to preserve their social ties when face-to-face interactions were not permitted [48]. Another longitudinal study showed that teens who engaged in meaningful conversations on social media experienced an increase in gratitude over time [49]. One-to-one communication and self-disclosure in mutual online friendships, as well as positive and humorous online experiences were shown to reduce feelings of stress and loneliness and increase emotional support [50]. These results suggest that social networks had a soothing effect in the sense that they served as a distraction in stressful situations and connected individuals to the outside world and positive experiences, especially when children and adolescents were isolated and confined.
However, other studies have found that digital media use during the pandemic reduced well-being. One possible explanation has to do with the overload of pandemic-related information on social media platforms, which was often negative and inaccurate, and increased feelings of worry, anxiety, and fear of missing out (FoMO), thus lowering well-being [51]. Older students, who had a better grasp of the pandemic’s severity, suffered more from the adverse effects of social media content exposure. In addition, children and adolescents used social media during the pandemic as a way to cope with boredom and negativity, as well as for entertainment, and often passively followed social media content without engaging [5]. Previous research suggests that this kind of compensatory and passive social media use results in poorer well-being [52] including greater anxiety, depression, loneliness, and low self-esteem due to body-related concerns and social comparison [53]. Further, social media use impacted healthy habits that supported mental health. For instance, greater social media use disrupted sleep patterns, leading to more screen time at night, which has been related to anxiety and irritability [54].
Thus, the present findings raise important concerns about the tradeoff between the benefits and drawbacks of social media use in children and adolescents. While these platforms may be useful coping mechanisms during stressful periods, they may also worsen mental health issues if used too much or too often. These findings underscore the notion that the impact of social media is not uniform, but is rather influenced by factors such as usage patterns, motivations, timing, and user demographics. To further elucidate these complex relationships, future research should explore specific types of social media interactions and their associated psychological impact.
The results also showed that social support was an important moderating factor in the relationship between social media use and mental health outcomes, and reduced the negative effects of high social media use on psychiatric symptoms and emotional well-being. One possible explanation is that children who have strong social support have more positive experiences both online and offline. They have higher self-esteem, enjoy more popularity, and have a greater sense of belonging to their social groups. They also face less rejection, Fear of Missing Out, and social comparison, all of which have been linked to increased mental health problems as a result of social media use in previous work [55]. In addition, these children have more positive social interactions on social media [56], which may enhance their social skills and relationships.
The emotional effects of social media use were more complex for those who participated in extracurricular activities. On the positive side, children and adolescents who were involved in extracurricular activities exhibited greater well-being and mental health during the pandemic and beyond, and social media provided extra benefits for these children and adolescents by enhancing their positive emotions. It is possible that social media allowed them to express themselves, connect with others, or cope with stress, in addition to their extracurricular experiences. On the negative side, however, this group also showed more signs of general distress and somatization after using social media. This suggests that they were more susceptible to the harmful consequences of overusing social media.
Contrary to expectations, these children and teens did not reduce their social media use despite their involvement in extracurricular activities. It is possible that for children and adolescents who are highly engaged in extracurricular activities, the time spent on social media could disrupt their routines or take away from their limited free time, potentially causing distress or exacerbating existing feelings of being overwhelmed. Social media could also expose them to constant comparison with others, which could increase their stress or anxiety, especially if they feel inadequate or pressured by their extracurricular activities.
The influence of social media use on mental health symptoms was moderated by age and gender. Specifically, older children and adolescents showed a more significant increase in somatization symptoms with increased social media use. In addition, girls experienced a more substantial relationships of daily social media use with psychiatric symptoms and reported lower life satisfaction than boys. These findings are consistent with previous research indicating an increase in the negative effects of social media as children enter adolescence [57], and a more pronounced impact on girls [58]. This suggests that both age and gender are crucial factors in determining the psychological effects of social media use.
Limitations
This study has several limitations. First, the assessment of social media use in this study relied on retrospective data collection where the participants were asked to recall past activities, rather than tracking participants’ activities through contemporaneous time-diary studies, which are considered the gold standard in time-use research. Fortunately, comparisons between survey responses and experience sampling in the same individuals indicate consistent estimates, particularly for regularly occurring activities [59]. In addition, reliance on self-reported measures for well-being and mental health introduces limitations such as social desirability and recall and other biases.
Moreover, while the BSI Israeli norms for adolescents provide a valuable framework for our study, they may not fully capture the subtle variations across different adolescent age groups. Established over two decades ago, these norms might not entirely reflect the complex psychological landscape faced by today’s youth. The societal, technological, and environmental shifts that have occurred since then suggest that a reevaluation of these norms could be beneficial. Our study underscores the importance of revisiting and updating these norms to more accurately depict the multifaceted nature of adolescent mental health today.
Additionally, this study solely measured the frequency, not the quality, of social media use. Evaluating the quality of social media engagement in terms of factors such as the social comparisons, addiction, active versus passive engagement, and types of usage might yield different associations with well-being and symptoms. Moreover, while the study focused on the two potential protective factors of extracurricular activities and social support other factors including personality traits, coping strategies, family cohesion, adaptability, parent-child relationships, and technology use patterns could act as significant moderators for psychiatric symptoms linked to the pandemic.
Conclusion
The increased use of digital media observed after the pandemic is suggestive of the emergence of new behavioral norms for social media use among children and adolescents. This emphasizes the need for interventions that not only encourage positive usage but also mitigate its adverse effects on mental health. Such interventions could include educating young people about the pros and cons of social media use, providing them with strategies to manage their online time and activities, and encouraging them to seek professional help when needed.
The importance of protective factors such as social support and extracurricular activities as highlighted in this study underscores the profound interconnectedness between children’s and adolescents’ mental health and their daily habits and social environments. Investing efforts in nurturing supportive relationships, thus has immense potential value in providing crucial support to young people. Further, promoting consistent extracurricular activities offers structure, stability, and offline social interactions, all of which play pivotal roles in children and adolescents’ mental health. However, children who are very busy with extracurricular activities were more negatively affected by the excessive use of social media. Future work should explore how to achieve a balance for these children, to enable them to thrive both in the social space in reality and in the virtual space.
The considerable mental health decline among post-pandemic children and teenagers necessitates urgent attention. Addressing this requires multifaceted approaches, mitigating increased social media impact and fortifying diminishing social support. Strategies involving parents, educators, and mental health practitioners are crucial to nurturing and rebuilding these support structures. Implementing systematic screening protocols for early mental health detection and tailored interventions is imperative. Collaborative efforts among professionals are essential to equilibrating digital engagement and mental well-being in the younger generation to foster resilience in the aftermath of the pandemic.
Data availability
The data is available upon request. Requests to access the dataset should be directed to ashoshani@runi.ac.il.
References
Reid Chassiakos YL, Radesky J, Christakis D, Moreno MA, Cross C, Hill D, Swanson WS (2016) Children and adolescents and digital media. Pediatrics 138(5):e20162593. https://doi.org/10.1542/peds.2016-2593
Spies Shapiro LA, Margolin G (2014) Growing up wired: Social networking sites and adolescent psychosocial development. Clin Child Fam Psychol Rev 17:1–18. https://doi.org/10.1007/s10567-013-0135-1
Salzano G, Passanisi S, Pira F, Sorrenti L, La Monica G, Pajno GB, Lombardo F (2021) Quarantine due to the COVID-19 pandemic from the perspective of adolescents: the crucial role of technology. Ital J Pediatr 47(1):1–5. https://doi.org/10.1186/s13052-021-00997-7
Bérard M, Manneville F, Minary L, Ligier F, Bitar S, Agrinier N (2023) Mediating effect of sleep in the association between social media use and mental health among French adolescents during the COVID-19 sanitary crisis. Sleep Med 112:223–231. https://doi.org/10.1016/j.sleep.2023.10.020
Marciano L, Ostroumova M, Schulz PJ, Camerini AL (2022) Digital media use and adolescents’ mental health during the COVID-19 pandemic: a systematic review and meta-analysis. Front Public Health 9:793868. https://doi.org/10.3389/fpubh.2021.793868
Keles B, McCrae N, Grealish A (2020) A systematic review: the influence of social media on depression, anxiety and psychological distress in adolescents. Int J Adolesc Youth 25(1):79–93. https://doi.org/10.1080/02673843.2019.1590851
Ma L, Evans B, Kleppang AL, Hagquist C (2021) The association between screen time and reported depressive symptoms among adolescents in Sweden. Fam Pract 38(6):773–779. https://doi.org/10.1093/fampra/cmab029
Sikorska IM, Lipp N, Wróbel P, Wyra M (2021) Adolescent mental health and activities in the period of social isolation caused by the COVID-19 pandemic. Adv Psychiatry Neurol 30(2):79–95. https://doi.org/10.5114/ppn.2021.108472
Alimoradi Z, Lotfi A, Lin CY, Griffiths MD, Pakpour AH (2022) Estimation of behavioral addiction prevalence during COVID-19 pandemic: a systematic review and meta-analysis. Curr Addict Rep 9(4):486–517. https://doi.org/10.1007/s40429-022-00435-6
Hudimova A (2021) Adolescents’ involvement in social media: before and during COVID-19 pandemic. Int J Innov Technol Soc Sci 24(1):29. https://doi.org/10.31435/rsglobal_ijitss/30032021/7370
Depoux A, Martin S, Karafillakis E, Preet R, Wilder-Smith A, Larson H (2020) The pandemic of social media panic travels faster than the COVID-19 outbreak. J Travel Med 27(3):taaa031. https://doi.org/10.1093/jtm/taaa031
Scott SR, Rivera KM, Rushing E, Manczak EM, Rozek CS, Doom JR (2021) I hate this: a qualitative analysis of adolescents’ self-reported challenges during the COVID-19 pandemic. J Adolesc Health 68(2):262–269. https://doi.org/10.1016/j.jadohealth.2020.11.010
Patchin JW (2021) Bullying during the COVID-19 pandemic. Cyberbullying Res Cent. https://cyberbullying.org/bullying-during-the-covid-19-pandemic
Amran MS, Jamaluddin KA (2022) Adolescent screen time associated with risk factor of fear of missing out during pandemic Covid-19. Cyberpsychol Behav Soc Netw 25(6):398–403. https://doi.org/10.1089/cyber.2021.0308
Bozzola E, Spina G, Agostiniani R, Barni S, Russo R, Scarpato E, Di Mauro AO, Di Stefano AV, Caruso C, Corsello G, Staiano A (2022) The Use of Social Media in Children and adolescents: scoping review on the potential risks. Int J Environ Res Public Health 19(16):9960. https://doi.org/10.3390/ijerph19169960
Badura P, Geckova AM, Sigmundova D, van Dijk JP, Reijneveld SA (2015) When children play, they feel better: organized activity participation and health in adolescents. BMC Public Health 15:1–8. https://doi.org/10.1186/s12889-015-2427-5
Schaefer DR, Simpkins SD, Ettekal AV (2018) Can extracurricular activities reduce adolescent race/ethnic friendship segregation? In: Alwin DF, Felmlee DH, Kreager DA (eds) Social networks and the life course: integrating the development of human lives and social relational networks. Springer, New York, pp 315–339
Chi G, Wang L (2022) The association of sports participation with depressive symptoms and anxiety disorder in adolescents. Front Public Health 10:860994. https://doi.org/10.3389/fpubh.2022.860994
LaForge-MacKenzie K, Tombeau Cost K, Tsujimoto KC, Crosbie J, Charach A, Anagnostou E, Korczak DJ (2022) Participating in extracurricular activities and school sports during the COVID-19 pandemic: associations with child and youth mental health. Front Sports Act Living 4:936041. https://doi.org/10.3389/fspor.2022.936041
Oberle E, Ji XR, Kerai S, Guhn M, Schonert-Reichl KA, Gadermann AM (2020) Screen time and extracurricular activities as risk and protective factors for mental health in adolescence: a population-level study. Prev Med 141:106291. https://doi.org/10.1016/j.ypmed.2020.106291
Yang X, Yang X, Kumar P, Cao B, Ma X, Li T (2020) Social support and clinical improvement in COVID-19 positive patients in China. Nurs Outlook 68(6):830–837. https://doi.org/10.1016/j.outlook.2020.08.008
Liu CH, Zhang E, Wong GTF, Hyun S (2020) Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: clinical implications for US young adult mental health. Psychiatry Res 290:113172. https://doi.org/10.1016/j.psychres.2020.113172
Kurudirek F, Arıkan D, Ekici S (2022) Relationship between adolescents’ perceptions of social support and their psychological well-being during COVID-19 pandemic: a case study from Turkey. Child Youth Serv Rev 137:106491. https://doi.org/10.1016/j.childyouth.2022.106491
Wang X (2021) The motivations and uses of mainstream and social media during the COVID-19 pandemic in China: a structural equation modeling approach. Comput Hum Behav Rep 4:100098. https://doi.org/10.1016/j.chbr.2021.100098
Zhu S, Zhuang Y, Ip P (2021) Impacts on children and adolescents’ lifestyle, social support and their association with negative impacts of the COVID-19 pandemic. Int J Environ Res Public Health 18(9):4780. https://doi.org/10.3390/ijerph18094780
Levenson JC, Shensa A, Sidani JE, Colditz JB, Primack BA (2016) The association between social media use and sleep disturbance among young adults. Prev Med 85:36–41. https://doi.org/10.1016/j.ypmed.2016.01.001
Derogatis LR (2001) Brief symptom inventory 18. Johns Hopkins University, Baltimore
Seligson JL, Huebner ES, Valois RF (2003) Preliminary validation of the brief multidimensional students’ life satisfaction scale (BMSLSS). Soc Indic Res 61:121–145. https://doi.org/10.1023/A:1021326822957
Ebesutani C, Regan J, Smith A, Reise S, Higa-McMillan C, Chorpita BF (2012) The 10-Item positive and negative affect schedule for children, child and parent shortened versions. J Psychopathol Behav Assess 34(2):191–203. https://doi.org/10.1007/s10862-011-9273-2
Zimet GD, Dahlem NW, Zimet SG, Farley GK (1988) The multidimensional scale of perceived social support. J Pers Assess 52(1):30–41. https://doi.org/10.1207/s15327752jpa5201_2
Risco CM, Collado AD, Reynolds EK, Lejuez CW, MacPherson L (2016) Evaluation of the Environmental supports scale with a community sample of adolescents. Prev Sci 17(4):493–502. https://doi.org/10.1007/s11121-016-0637-4
Raudenbush SW, Bryk AS (2002) Hierarchical Linear Models: Applications and Data Analysis Methods, Second Edition. Newbury Park, CA
Anderson M, Jiang J (2018) Teens, social media & technology 2018. Pew Res Cent 31:1673–1689
Rideout V, Robb MB (2021) The role of media during the pandemic: connection, creativity, and learning for tweens and teens. Common Sense, San Francisco, CA
Canetti L, Shalev AY, De-Nour AK (1994) Israeli adolescents’ norms of the brief Symptom Inventory (BSI). Isr J Psychiatry Relat Sc 31(1):13–18
Slone M, Shechner T (2009) Psychiatric consequences for Israeli adolescents of protracted political violence: 1998–2004. J Child Psychol Psychiatry 50(3):280–289. https://doi.org/10.1111/j.1469-7610.2008.01940.x
Kor A, Shoshani A (2023) Moderating the impact of the COVID-19 pandemic on children’s and adolescents’ substance use, digital media use, and mental health: a randomized positive psychology addiction prevention program. Addict Behav 141:107660. https://doi.org/10.1016/j.addbeh.2023.107660
Bank of Israel (2020) The long-term impact of the disruption of studies during the COVID-19 period on students in Israel. BOI Publishing. Accessed 3 March 2024
UNICEF (2021) COVID-19 and school closures: One year of education disruption. https://data.unicef.org/wp-content/uploads/2021/03/COVID19-and-school-closures-report.pdf Accessed 3 March 2024
The National Authority for Measurement and Evaluation in Education (2021) Remote teaching and learning: Lessons from the lockdown period due to the COVID-19 pandemichttps://meyda.education.gov.il/files/Rama/Remote_learning_Teachers_Survey_extended_version.pdf Accessed 3 March 2024
Berman T (2019) The state of Young Children in Israel- 2019. The Israel National Council for the Child, Jerusalem
Twenge JM, Martin GN, Campbell WK (2018) Decreases in psychological well-being among American adolescents after 2012 and links to screen time during the rise of smartphone technology. Emotion 18(6):765–780. https://doi.org/10.1037/emo0000403
Walsh SD, Sela T, De Looze M, Craig W, Cosma A, Harel-Fisch Y et al (2020) Clusters of contemporary risk and their relationship to mental well-being among 15-year-old adolescents across 37 countries. J Adolesc Health 66(6):S40–S49. https://doi.org/10.1016/j.jadohealth.2020.03.010
Slone M, Shoshani A (2022) Effects of war and armed conflict on adolescents’ psychopathology and well-being: measuring political life events among youth. Terror Polit Violence 34(8):1797–1809. https://doi.org/10.1080/09546553.2020.1787314
Slone M, Shoshani A (2014) Psychiatric effects of protracted conflict and political life events exposure among adolescents in Israel: 1998–2011. J Trauma Stress 27(3):353–360. https://doi.org/10.1002/jts.21918
Cauberghe V, Van Wesenbeeck I, De Jans S, Hudders L, Ponnet K (2021) How adolescents use social media to cope with feelings of loneliness and anxiety during COVID-19 lockdown. Cyberpsychol Behav Soc Netw 24:250–257. https://doi.org/10.1089/cyber.2020.047842
Orben A (2020) Teenagers, screens and social media: a narrative review of reviews and key studies. Soc Psychiatry Psychiatr Epidemiol 55:407–414. https://doi.org/10.1007/s00127-019-01825-443
Kerekes N, Bador K, Sfendla A, Belaatar M, Mzadi AE, Jovic V et al (2021) Changes in adolescents’ psychosocial functioning and well-being as a consequence of long-term covid-19 restrictions. Int J Environ Res Public Health 18:8755. https://doi.org/10.3390/ijerph1816875544
Maheux AJ, Nesi J, Galla BM, Roberts SR, Choukas-Bradley S (2021) # Grateful: longitudinal associations between adolescents’ social media use and gratitude during the COVID-19 pandemic. J Res Adolesc 31:734–747. https://doi.org/10.1111/jora.12650
Rosen AO, Holmes AL, Balluerka N, Hidalgo MD, Gorostiaga A, Gómez-Benito J, Huedo-Medina TB (2022) Is social media a new type of social support? Social media use in Spain during the COVID-19 pandemic: a mixed methods study. Int J Environ Res Public Health 19:3952. https://doi.org/10.3390/ijerph19073952
Liu H, Liu W, Yoganathan V, Osburg V-S (2021) COVID-19 information overload and generation Z’s social media discontinuance intention during the pandemic lockdown. Technol Forecast Soc Change 166:120600. https://doi.org/10.1016/j.techfore.2021.120600
Hudimova A, Popovych I, Baidyk V, Buriak O, Kechyk O (2021) The impact of social media on young web users’ psychological well-being during the COVID-19 pandemic progression. Amazonia Investiga 10:50–61. https://doi.org/10.34069/AI/2021.39.03.5
Vall-Roqué H, Andrés A, Saldaña C (2021) The impact of COVID-19 lockdown on social network sites use, body image disturbances and self-esteem among adolescent and young women. Prog Neuropsychopharmacol Biol Psychiatry 110:110293. https://doi.org/10.1016/j.pnpbp.2021.110293
Li SH, Beames JR, Newby JM, Maston K, Christensen H, Werner-Seidler A (2021) The impact of COVID-19 on the lives and mental health of Australian adolescents. Eur Child Adolesc Psychiatry 31(9):1465–1477. https://doi.org/10.1007/s00787-021-01790-x
Dou F, Li Q, Li X, Li Q, Wang M (2021) Impact of perceived social support on fear of missing of out (FoMO): a moderated mediation model. Curr Psychol 42:63–72. https://doi.org/10.1007/s12144-021-01404-4
Benvenuti M, Panesi S, Giovagnoli S, Selleri P, Mazzoni E (2023) Teens online: how perceived social support influences the use of the internet during adolescence. Eur J Psychol Educ 1–22. https://doi.org/10.1007/s10212-023-00705-5
Panchal U, Salazar de Pablo G, Franco M, Moreno C, Parellada M, Arango C, Fusar-Poli P (2023) The impact of COVID-19 lockdown on child and adolescent mental health: systematic review. Eur Child Adolesc Psychiatry 32(7):1151–1177. https://doi.org/10.1007/s00787-021-01856-w
Twenge JM, Martin GN (2020) Gender differences in associations between digital media use and psychological well-being: evidence from three large datasets. J Adolesc 79:91–102. https://doi.org/10.1016/j.adolescence.2019.12.018
Sonnenberg B, Riediger M, Wrzus C, Wagner GG (2012) Measuring Time use in surveys—how valid are Time use questions in surveys. Concordance of survey and experience sampling measures. SSRN Electron J 41:1037–1052
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
A.S.: Conceptualization, Methodology, Supervision, Formal analysis, Writing. A.K.: Project administration, Investigation, Writing. S.B.: Project administration, Investigation.
Corresponding author
Ethics declarations
Competing interests
The authors have no competing interests to declare that are relevant to the content of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Shoshani, A., Kor, A. & Bar, S. The impact of social media use on psychiatric symptoms and well-being of children and adolescents in the Post-COVID-19 era: a four-year longitudinal study. Eur Child Adolesc Psychiatry (2024). https://doi.org/10.1007/s00787-024-02454-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00787-024-02454-2