
Abstract
Mental disorders account for a large and increasing health burden worldwide, as shown in the Global Burden of Diseases (GBD) Study 2010. Unpacking how this burden in children and adolescents varies with sex, geographical regions, and ethnicities and how it has changed in the last 3 decades are important to improve the existing public health policies and prevention strategies. The study was conducted using GBD 2019 database. The burden of children and adolescents’ (< 20 years old) mental disorders was displayed as prevalence, incidence, disability-adjusted life-years (DALYs), years of life lost, and years lived with disability globally between 1990 and 2019. The number of DALYs in children and adolescents diagnosed with mental disorders was 21.5 million (95% CI: 15.2–29.6 million) in 2019. From 1990 to 2019, the age-standardized rates of DALYs of mental disorders increased from 803.8 per 100,000 (95% CI: 567.7–1104.3 per 100,000) to 833.2 per 100,000 (95% CI: 589.0–1146.1 per 100,000) population. Over the past 30 years, there had been a huge increase in the number of individuals suffering from anxiety disorders, major depressive disorders, and conduct disorders including an alarming increase in the rate of eating disorders such as 24.3% in bulimia nervosa and 17.0% in anorexia nervosa. Globally, 8.8% of children and adolescents have been diagnosed with varieties of mental illnesses, accounting for a heavy disease burden on public health. Besides, the worldwide increasing rates of anxiety disorders, major depressive disorders, and eating disorders have brought considerable challenges to public health undertakings, for which further prevention and treatment countermeasures are urgently needed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mental disorders are usually associated with higher incidences of chronic physical abnormalities [1,2,3,4] and early mortality than normal aging-associated death [5]. Between 1990 and 2019, the reported mental disorders DALYs increased from 80.8 million to 125.3 million, and the percentage contributed by mental disorders increased from 3.1 to 4.9% [6]. In 2009, the WHO initiated World Mental Health (WMH) Survey reported that the inter-quartile range of 25th–75th percentiles of lifetime mental disorders’ (combining substance disorders, behavioral deficits, and abrupt mood changes) was 18.1–36.1% [7]. The global burden of disease (GBD) study also reported that mental and substance use disorders were the fifth leading disorder category of global disability-adjusted life-years (DALYs) in 2010 [8]. A cumulative review study has shown that on average, 1 out of 5 respondents (17.6%, 95% confidence interval (CI): 16.3–18.9%) was identified as meeting the full criteria for any of the frequently diagnosed mental illnesses during the 12-month pre-assessment period, while 29.2% (25.9–32.6%) of respondents were accounted for experiencing the symptoms of any type of common mental disorder at some point of their lifetimes [9]. The 2009 WMH results suggest that mental disorders may commonly occur with or without any comorbidity, and often the symptoms are manifested at an early age of onset, leading to significantly adverse socio-economic burden [10]. Unfortunately, only a small percentage of these patients with mental disorders receive treatment in clinical settings in most countries, and even fewer of these patients may have the opportunity to receive high-quality treatments [11].
Over the past decades, the prevalence of childhood disability coupled with impaired mental health and retarded neurodevelopmental conditions has drastically increased. Halfon et al. have reported that mental health disorders are the leading cause of physical disabilities in children and adolescents aged under 18 years in the United States [12]. Moreover, emerging studies showed that, in the Americas and Europe, mental disorders ranked second among the most common causes of DALYs in children aged 5–14 years in 2015 [13]. A retrospective meta-analysis including 41 studies conducted in 27 countries has revealed that the worldwide-pooled prevalence of mental disorders is approximately 13.4% in children and adolescents [14]. Notably, juvenile and adolescent-associated mental disorders are often neglected and remain undiagnosed in many countries. In recent years, the focus of global health care has been dramatically shifted toward improving the early diagnosis and treatment opportunities for childhood mental illnesses, thereby reducing the early-life mortality rates.
During the past 3 decades, the world has experienced several ups and downs, like wars, low fertility rates, economic growth, improvement of medical settings, and notable environmental changes. Given that the prevalence of most mental disorders varies greatly based on the subject’s age, sex and ethnicity, their burden is expected to be reduced in recent years with rapid technological advancements in diagnostic tools and medical intervention strategies. Due to the lack of statistically significant global data, the current study exploits the GBD 2019 database to update the previous investigations on mental health disorders data in children and adolescents covering the period 1990–2019. Here, we represented the prevalence, incidence, and their burden as absolute numbers and rates attributable to all kinds of mental disorders in general, and age, sex, year, and the subject’s geographical location for the period 1990–2019 to provide the updated information for better health care decision making and policy implementation.
Methods
Case definition and categorization
Mental disorders are divided into 12 major categories in GBD studies, such as schizophrenia, major depressive disorder, dysthymia, bipolar disorder, anxiety disorders, anorexia nervosa, bulimia nervosa, autism spectrum disorders, attention-deficit/hyperactivity disorder, conduct disorder, idiopathic intellectual disability, and other mental disorders. In the GBD study, cases were selected based on the diagnostic criteria of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM) or International Classification of Diseases (ICD). Different versions of DSM (DSM-III, DSM-III-R, DSM-IV, DSM-IV-TR, and DSM-V) and ICD (ICD-9 and ICD-10) were employed for this study [15].
Data sources
Data were obtained from the Global Health Data Exchange GBD Results Tool (http://ghdx.healthdata.org/gbd-results-tool). The GBD 2019 was created by GBD collaborators to provide a systematic assessment of the burden of 369 diseases and injuries, including the aforementioned 12 mental disorders, from January 1st 1990, to December 31st 2019 [16]. The general methodology of GBD 2019 and its main changes compared with previous years have been described in the previous publication [17]. Briefly, the GBD 2019 study used data from national censuses, demographic surveys, disease surveillance point systems, causes of death registration report information systems, and systematically reviewed published literature on the incidence and prevalence of various diseases. As not all disorders from all countries were assessed, the GBD 2019 study used DisModMR 2.1, a Bayesian metaregression tool, as the primary estimation method to ensure consistency between the incidence, prevalence, and mortality rates for each diseased condition.
The GBD 2019 study estimated the burden of diseases, injuries, and risk factors for 204 countries, territories, and selected subnational locations. The GBD 2019 data resources allowed us to query all causes, risks, impairments, and injuries by nature, measure of deaths, years of life lost (YLLs), years lived with disability (YLDs), DALYs, prevalence, incidence, and so on during the period of 1990–2019 for all measures—by metrics of number, rate, percent and years; by genders; by all GBD age groups and by locations of GBD super regions, regions, countries, selected subnational units, and custom regions (WHO regions, World Bank Income Levels, and more). YLL is defined as the measure of premature death within a group of people. YLLs are calculated by starting with the highest achievable life expectancy in a given year for a given age group, then subtracting the age at which a person in that age group dies. YLD measures the amount of time people lose to diseases and injuries that degrade health but do not cause death. It is calculated by multiplying a disability’s severity by the time it lasts. DALY defines as years of healthy life lost, the sum of years lost due to YLLs and YLDs.
Statistical analysis
This study was designed based on the GBD database to analyze the global burden of mental illness, measuring disease burden data of children and adolescents less than 20 years old. First, the prevalence, incidence, DALYs, YLLs, and YLDs of 12 mental disorders in children and adolescents worldwide in 1990 and 2019 were analyzed and compared. Further, the burden of 12 psychiatric disorders was assessed for different developmental ages and different gender. The influence of economic-geographical factors, regions, and countries on the overall burden of mental illnesses among children and adolescents were also studied.
In this study, children and adolescents (< 20 years) were divided into 5 GBD age groups (0 to ≤ 4 years, 5 to ≤ 9 years, 10 to ≤ 14 years, and 15 to ≤ 19 years). We analyzed the different development levels affecting the burden of mental disorders by socio-demographic index (SDI). SDI is a compound measure of income, average years of schooling, and fertility for each GBD location, and the year which is used as a measure of socio-demographic development. The GBD 2019 database divides the world into five categories according to the SDI index: low-SDI countries, low-middle SDI countries, middle-SDI countries, high-middle SDI countries, and high-SDI countries. This study further refined the distribution of disease burden by geographical regions. Regions included in this study were: the high-income Asia Pacific, high-income North America, Western Europe, Australasia, Andean Latin America, Tropical Latin America, Central Latin America, Southern Latin America, Caribbean, Central Europe, Eastern Europe, Central Asia, North Africa, and Middle East, South Asia, Southeast Asia, East Asia, Oceania, Western sub-Saharan Africa, Eastern sub-Saharan Africa, Central sub-Saharan Africa, and Southern sub-Saharan Africa.
Results
The prevalence, incidence, DALYs, YLDs, and YLLs of child and adolescent mental disorders in 2019 and 1990
In 2019, the global prevalence of mental disorders was 8830.79 per 100,000 (7685.15–10,043.49 per 100,000; 95% CI) population, including people aged 0–19 years (Table 1). In this age group, the prevalence of mental disorders was the seventh highest among 22 grade 3 causes in GBD 2019 database, much higher than digestive disease, and about twice the prevalence of chronic respiratory disease. Within the subtypes of various mental disorders, anxiety disorder accounted for the highest prevalence, followed by idiopathic developmental intellectual disability, and attention-deficit/hyperactivity disorder. In 1990, total prevalence of mental disorders was 8950.73 per 100,000 (7753.72–10,208.97 per 100,000; 95% CI) children and adolescent populations. However, from 1990 to 2019, the total mental disorders’ prevalence decreased slightly by 1.3% (119.94 per 100,000). In these years, the highest prevalence among different forms of mental disorders changed from idiopathic developmental intellectual disability to anxiety disorders. In the last 3 decades, the most significant increases in the prevalence of mental disorder subtypes were observed for conduct disorder (118.34 per 100,000, an increase of 8.2% from 1990), depression disorder (89.05 per 100,000, an increase of 10.9% from 1990), and anxiety disorder (35.10 per 100,000, an increase of 1.6% from 1990), while the most significant decreases were accounted for idiopathic developmental intellectual disability and attention-deficit/hyperactivity disorder. Depressive disorders consist of major depressive disorder and dysthymia. The increase in depressive disorders might be mainly due to the increase in major depressive disorder, which was increased by 64.28 per 100,000(an increase of 10.2% from 1990).
The incidence of mental disorders was 2764.18 per 100,000 (2342.78–3276.32 per 100,000) in people aged 0–19 years in 2019. In this age group, the incidence of mental disorders was the tenth highest among 22 grade 3 causes in GBD 2019 database, about three times as many as chronic respiratory disease, and about twice the prevalence of digestive disease. Within the mental disorder subtypes, major depressive disorder (1157.01 per 100,000) accounted for the highest incidence, followed by conduct disorder (542.22 per 100,000) and anxiety disorders (531.58 per 100,000). Comparing with 1990, the total incidence of mental disorders grew by 6.8% (174.85 per 100,000). The top three most significant absolute increases in incidence were observed for major depressive disorder (92.67 per 100,000, an increase of 8.7% from 1990), eating disorders (40.18 per 100,000, an increase of 22.9% from 1990), and conduct disorder (33.26 per 100,000, an increase of 6.5% from 1990), and the most significant decreases were noted for attention-deficit/hyperactivity disorder (12.86 per 100,000, a decrease of 7.3% from 1990) and autism spectrum disorders (3.11 per 100,000, a decrease of 11.7% from 1990). Eating disorders consist of anorexia nervosa and bulimia nervosa. The increase in eating disorders might be mainly due to the increase in bulimia nervosa symptoms, which increased by 36.57 per 100,000 (an increase of 23.5% from 1990).
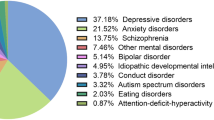
In 2019, mental disorders were responsible for 21.5 million YLDs (15.2–29.6 million) globally in people aged 0–19 years, and within different types of mental disorders, anxiety disorders (5.7 million) accounted for most YLDs, followed by conduct disorder (4.9 million) and major depressive disorder (3.8 million). From 1990 to 2019, the highest YLDs among various types of mental disorders had no obvious change. In the 3 decades of change, the top increases were in cases of conduct disorder (0.9 million) and major depressive disorder (0.8 million), and the only decrease was found for idiopathic developmental intellectual disability.
In children and adolescents, eating disorders were the only mental disorders associated with mortality. The numbers of YLLs attributable to anorexia nervosa and bulimia nervosa were 1674.95 (1376.86–2594.17) and 245.69 (122.14–683.76), respectively, in 2019. Thus, mental disorders were responsible for 1920.64 YLLs (1523.08–3008.28) in people aged 0–19 years. From 1990 to 2019, mental disorders’ YLLs were grown up from 1570.50 to 1920.64 (an increase of 22.3%).
Given that DALYs are the sum of YLLs and YLDs, in this study, DALYs for mental disorders were YLDs for the mental disorders plus YLLs for the eating disorders. In 2019, mental disorders were responsible for 21.5 million DALYs (15.2–29.6 million) in people aged 0–19 years, while the data from 1990 indicated the occurrence of 18.3 million DALYs (12.9–25.1 million) in this population. The total age-standardized rate of DALYs was 833.2 per 100,000 (589.0–1146.1 per 100,000) population in 2019 and 803.8 per 100,000 (567.7–1104.3 per 100,000) population in 1990. Within the mental disorder categories, the highest age-standardized rate of DALYs was documented for anxiety disorders (222.2 per 100,000; 95% CI: 140.1–329.0 per 100,000), followed by conduct disorder (147.0 per 100,000; 95% CI: 88.7–234.0 per 100,000) and major depressive disorder (188.9 per 100,000; 95% CI: 106.1–295.5 per 100,000). From 1990 to 2019, the variation of DALYs’ number was consistent with that of YLDs. When calculating the rate of increase for each disease, the fastest rate of increase for mental disorders was 24.3% for bulimia nervosa and 17.0% for anorexia nervosa.
Taking gender into account, mental disorders led to 10.5 million (95% CI: 7.5–14.4 million) DALYs in female individuals, accounting for 48.8% of the total disease burden (Table 2), while mental disorders led to 11.0 million (95% CI: 7.7–15.1 million) DALYs in male individuals, accounting for 50.2% of the total disease burden in 2019. Boys and men (aged < 20 years) had a greater proportion of burden than girls and women with equivalent age. The gender-associated age-standardized rates of DALYs were varied from 838.9 per 100,000 (95% CI: 596.8–1153.7 per 100,000) of the girls and women to 827.7 per 100,000 (95% CI: 581.1–1138.0 per 100,000) of the boys and men. Moreover, this difference was especially vivid in the case of autism spectrum disorders, for which the age-standardized rate of DALYs in boys and men was 3 times more than that of the girls and women. It is important to note that among children and adolescents, the age-standardized rates of DALYs for eating disorders in females were twice higher than in males. The mental health-related diseases with the highest age-standardized rates of DALYs included anxiety disorder (274.22 per 100,000; 95% CI: 174.11–403.75 per 100,000), major depressive disorder (189.86 per 100,000; 95% CI: 114.66–301.55 per 100,000) and conduct disorder (133.75 per 100,000; 95% CI: 72.57–219.74 per 100,000) in female children and adolescents, while the highest age-standardized rates of DALYs in male children and adolescents were conduct disorder (240.74 per 100,000; 95% CI: 139.66–375.85 per 100,000), anxiety disorder (173.28 per 100,000; 95% CI: 109.43–260.42 per 100,000) and major depressive disorder (106.70 per 100,000; 95% CI: 64.10–170.76 per 100,000). From 1990 to 2019, the age-standardized rates for DALYs among female minors also exhibited 4.1% increase as shown numerically from 805.94 (95% CI: 577.45–1104.58 per 100,000) to 838.92 per 100,000 (95% CI: 596.79–1153.71 per 100,000) population. Likewise, over the 30-year period, the age-standardized rates of DALYs among male adolescents also increased from 801.67 (95% CI: 566.06–1102.43 per 100,000) to 827.74 per 100,000 (95% CI: 581.05–1138.01 per 100,000) population, resulting in an increase of 3.3%.
Mental disease burden of children and adolescents in different age groups
The burden of mental disorders was reflected in all age groups. In the GBD database, not all diseases were analyzed from birth. The mental disorders DALYs in children and adolescents of different age group (aged < 20 years) are shown in Fig. 1. The number of DALYs was found to vary along with the age of the child, from 1.0 million of the youngest children (0 to < 5 years) to 10.0 million in the oldest (15 < 20 years) population. Most mental disorders associated with DALYs were found to increase with aging in childhood and adolescence. However, the exceptions were observed in the number of highest DALYs for conduct disorder and attention-deficit/hyperactivity disorder that occurred in the age range of 10–14 years, followed by a gradual decline. Moreover, DALYs for autism spectrum disorders and idiopathic developmental intellectual disability exhibited a slight decrease with respect to aging. The burden associated with the less common but chronic disorders, such as schizophrenia and bipolar disorder, and so on, also showed a rapid increase. Among young children and adolescents, the most significant increases were documented for anxiety disorders and major depressive disorder.

The mental disorders DALYs in children and adolescents of different age group (aged < 20 years) in 2019
From 1990 to 2019, the change of disease proportion in children and adolescents (< 20 years) was ranged according to the descending order as bulimia nervosa (20.0%), anorexia nervosa (12.8%), and idiopathic developmental intellectual disability (–16.7%), as shown in Fig. 2. Likewise, for the children aged below 5 years, the change of disease proportion was ranged from the largest to the smallest occurrence as major depressive disorder (17.7%), dysthymia (14.4%) and idiopathic developmental intellectual disability (–13.1%), and that for the children aged 5–9 years was bulimia nervosa (22.8%), major depressive disorder (19.7%), and idiopathic developmental intellectual disability (–13.4%). The changes in disease proportion in children aged 10–14 years were ranged from the highest to the lowest incidence as bulimia nervosa (16.1%), major depressive disorder (11.0%), and idiopathic developmental intellectual disability (–11.7%), while that for the children aged 15–19 years was ranged from the highest to the lowest occurrence as bulimia nervosa (17.0%), anorexia nervosa (10.6%), and attention-deficit/hyperactivity disorder (–13.8%).

DALYs proportions (%) for mental disorders in each age group across childhood and adolescents in 2019 and 1990
Mental disease DALYs rate in different socio-demographic indexes (SDI)
As shown in Fig. 3, in 2019, anxiety disorders, conduct disorder, and major depressive disorder had the highest proportion of total disease burden across all regions. For most of the diseases, the DALYs rates were increased with the SDI index, except for idiopathic developmental intellectual disability. Idiopathic developmental intellectual disability exhibited the greatest regional variation. The proportion of age-standardized rates of DALYs attributable to idiopathic developmental intellectual disability was more than 4.4 times higher in low-SDI countries (105.4 per 100,000) than it was in high-SDI countries (19.5 per 100,000). Bulimia nervosa DALYs exhibited a variation of more than 4.1 times between the SDI regions, while it was more than 3.0 times in case of anorexia nervosa DALYs. By contrast, conduct disorder, dysthymia, and schizophrenia were stable in terms of their age-standardized rates of DALYs (less than or equal to 0.5 times variation between regions). The DALYs rates of children and adolescents with 12 mental disorders in different SDI regions in 1990 and 2019 are depicted in Supplementary Table 1.

The age-standardized rates of DALYs attributable to mental disorders as a proportion of all disease burden by SDI region in 2019 and 1990
From 1990 to 2019, the most significant DALYs rate increase was reflected in case of bulimia nervosa, and the most significant DALYs rate decrease was observed in idiopathic developmental intellectual disability in low-SDI countries (28–16%), low-middle SDI countries (55–25%), middle-SDI countries (46–22%) and high-middle SDI countries (35–19%). However, for the high-SDI countries (35–22%), the most significant DALYs rate increase was found in major depressive disorder and the most significant DALYs rate decrease was reported in idiopathic developmental intellectual disability.
Mental disease DALYs rate in a different region
Among the GBD regions, the highest rate of DALYs for mental disorders was found in Australia, both in 2019 (1364.0 per 100,000; 95% CI: 967.2–1889.4 per 100,000) and 1990 (1370.3 per 100,000; 95% CI: 963.6–1877.6 per 100,000), as shown in Fig. 4. The next highest-ranking regions included Western Europe (1,301.1 per 100,000; 95% CI: 915.8–1768.3 per 100,000), North Africa and Middle East together (1077.5 per 100,000; 95% CI: 770.6–1483.4 per 100,000) in 1990, and Western Europe (1258.0 per 100,000; 95% CI: 878.9–1725.0 per 100,000) and high-income North America (1242.2 per 100,000; 95% CI: 892.7–1697.0 per 100,000) in 2019. The GBD 2019 database classifies 204 countries into 21 regions. DALYs rates of children and Adolescents with 12 mental disorders in 204 countries in 2019 are shown in the supplementary Table 2 as supplementary file. The region-specific lowest DALYs rates for mental disorders in 1990 were found in Central Asia (643.4 per 100,000; 95% CI: 451.8–895.0 per 100,000), Western Sub-Saharan Africa (666.8 per 100,000; 95% CI: 468.7–921.8 per 100,000) and South Asia (709.6 per 100,000; 95% CI: 487.8–980.0 per 100,000), which were gradually shifted towards Central Asia (642.0 per 100,000; 95% CI: 446.8–895.7 per 100,000), Eastern Europe (701.4 per 100,000; 95% CI: 491.1–972.6 per 100,000) and East Asia (703.3 per 100,000; 95% CI: 495.8–964.5 per 100,000) in 2019. The most significant changes in these 3 decades were found in high-income North America (24.7%), Tropical Latin America (17.2%) and Central Latin America (12.2%).

The age-standardized rates of DALYs attributable to mental disorders as a proportion of all disease burden by 21 GBD regions
In both 1990 and 2019, major depressive disorder, anxiety disorders, and conduct disorder had the highest age-standardized rates of DALYs across all regions, except for South Asia, in which idiopathic developmental intellectual disability, conduct disorder, and anxiety disorders presented the highest age-standardized rates of DALYs. In most of the regions, there had been significant increases. There were also some geographical regions where age-standardized rates of DALYs for multiple mental disorders were significantly reduced (such as high-income Asia Pacific, Western Europe, Australia, Central Europe, Eastern Europe, and East Asia). The three disorders with the greatest regional variations were accounted for depressive disorders, eating disorders, and idiopathic developmental intellectual disability. There was a large increase in depressive disorders’ age-standardized rates of DALYs in most of these regions (e.g., high-income North America, Tropical Latin America, and Central Latin America, 2–55%), and a small decrease in some countries (e.g., East Asia, Eastern Europe and Central Europe, 1–26%) was also observed. Notably, for eating disorders, growth rates of DALYs were increased in almost all regions (4–62%), especially in South Asia (62%), East Asia (47%), and Southeast Asia (42%) except for 1% decrease in Eastern Europe. In a special case, idiopathic developmental intellectual disability exhibited a rapid decline (5–56%) in almost all countries and regions except Australia, the Caribbean, and Central Saudi Arabia, where increases were recorded as 16%, 4%, and 7%, respectively.
Mental disease DALYs rate in a different country
As Fig. 5 demonstrates, in 2019, the age-standardized rates of DALYs for mental disorders were greatly varied among the countries for which data were available (data not available is grayed out on the map), ranging from 606.6 per 100,000 (95% CI: 421.8–842.7 per 100,000) population in Mongolia, being the lowest, to 1558.8 per 100,000 (95% CI: 1074.0–2151.1 per 100,000) population in Portugal, as the highest. DALYs rates of children and adolescents with mental disorders in 204 countries are presented in the supplementary Table 2. Among these countries or regions, the top ten ranking regions were Portugal, Spain, New Zealand, Greece, Syrian Arab Republic, Ireland, Australia, Andorra, San Marino, and Netherlands, in descending order. While the top 10 countries with the lowest rates were Mongolia, Kazakhstan, Vietnam, Turkmenistan, Uzbekistan, Kyrgyzstan, Bangladesh, Mali, Tajikistan, and Azerbaijan, in descending order. Countries with relatively high age-standardized rates of DALYs were mainly high-income countries, mainly located in Australasia, Western Europe, North Africa, and Middle East. Countries with relatively low age-standardized rates of DALYs were mainly low-SDI countries, distributed in Central Asia, Southeast Asia, South Asia, and Western sub-Saharan Africa. However, despite clear trends in burden proportions, many of these differences between the countries were within wide ranges of uncertainty resulting from the lack of epidemiological data for many of these countries and territories.

The differences of age-standardized rates of DALYs in child and adolescent mental disorders at the 204 country or territorial level in 2019
Discussion
This study was the first of its kind that displayed the prevalence and burden of mental disorders other than substance abuse. The comprehensive and standardized statistical approach of the GBD 2019 database made it possible to compare the global disease burden across time and regions [18]. To the best of our knowledge, no population-based studies have comprehensively described the concurrent relationship between the socio-economic conditions in different geographical areas or countries and the mental illness burden among children and adolescents in recent years.
In this study, the results showed that in the past 3 decades, the total burden of mental disease was increased rapidly, but the rate of increase was not consistent between different age groups, different genders, different diseases, and different locations. The GBD 2019 results for 1990 and 2019 exhibited the increase rate of the total burden of mental disorders by 14.9%, from 18.3 million (95% CI: 12.9–25.1 million) in 1990 to 21.5 million (95% CI: 15.2–29.6 million) DALYs in 2019. Further growth of the mental disease burden conveyed in our report was consistent with the previous study reported by Whiteford et al. in 2010, indicating that the burden of mental and substance use disorders increased by 37.6% between 1990 and 2010 in all ages, which for most disorders was driven by population growth and aging (of which substance use disorders alone accounted for about 20.5% DALYs) [8]. Similar to the findings of a study of adolescent mental disorders in 27 countries in the Eastern Mediterranean [19], our study revealed that anxiety disorders, conduct disorders, and depressive disorders accounted for a large proportion of illnesses. Anxiety disorders were found to be the most prevalent class of mental disorders in youth aged < 20 years in our research, as consistent with the estimated lifetime prevalence of any anxiety disorder averaging approximately 16% across WHO surveys reported by Kessler et al. [10].
The present study revealed that the proportion and magnitude of growth in the disease burden were gender-related. Notably, gender differences in autism spectrum disorders and eating disorders were 2–3 times or more in adolescents. The highlights of our study were in agreement with the previously published research results by Wang et al., revealing that the crude rates of prevalence and the DALY rates of eating disorders were higher for females than that for males in all age groups. The highest crude rates of prevalence and DALY rates were observed among those aged 15–39 years for eating disorders and anorexia nervosa and among those aged 15–44 years for bulimia nervosa [20]. The reasons are multifactorial and might be related to the psychological characteristics of these age groups. Women are more likely to suffer from negative body talk, including appearance related teasing and pressure from siblings [21], have lower body satisfaction, and are more likely to have irregular frequency of certain foods [22], all these can be triggers for eating disorders. In addition, some studies have found that women are more prone to self-depression. It is reported that women are more selflessness and eating disorders than men, and self-repression is a more closely linked to eating disorders in women than in men [23]. This finding was consistent with previous prevalence studies and eating disorder statistics, partly explaining sex differences in eating disorders.
We observed that the disease burden of most subtypes of mental disorders was significantly increased with aging and observed a sharply increasing rate in anorexia bulimia versus a decreasing rate in idiopathic developmental intellectual disability at different age groups. Chinese researchers have revealed the prevalence trend of eating disorders in 2009, reporting the high prevalence in adolescence [24]. Similarly, it has been reported that at 4 years of age, the prevalence of intellectual disability was 4.5%, and the idiopathic intellectual disability accounts for 12.6% [25]. Stress, nutrition, parental care, and cognitive stimulation are some of the critical factors that can mediate the impact on brain structure and cognitive function, as memory, executive function, and language [26]. It is worth mentioning that, compared with other mental disorders, the prevalence and burden of eating disorders were smaller, but in these recent years, the rapidly increasing rate of eating disorders is alarming, in cases of both anorexia nervosa and bulimia nervosa, especially for anorexia nervosa. Disease characteristics revealed that it had serious negative effects, which could be the most significant cause of death among mental disorders in addition to suicide and chronic disease accidents [27, 28].
Further analyses of the relationships between the diseases, socio-demographic and geographical factors showed that diseases in high-SDI countries and high-income countries presented more significant characteristics of disease onset and burden, while in low-income countries and low-SDI countries, developmental disorders were significantly higher than those in other countries and regions. In terms of the distribution of various diseases, this study found that anxiety disorders, major depressive disorder, and conduct disorder were among the most common diseases in all SDI countries and regions. When the burden of disease was analyzed by country, the countries with the highest disease burden were Portugal, Spain, and New Zealand. These countries have reportedly high economic income and social demographic index, which again confirms our statistical data. Studies have also shown that most of the children affected by ID are from low-income families whose parents have a low educational level. This might be due to the effect of poverty on child development and educational outcomes [29, 30]. There have also been studies that have found a relationship between disease burden and race, suggesting that the racial/ethnic disparities in attention-deficit/hyperactivity disorder diagnosis may occur by kindergarten and continue until at least the end of eighth grade. In these studies, African Americans, Hispanics, and children of other races/ethnicities were 69%, 50%, and 46% lower in populations, respectively, than that for whites. In addition, these studies have also included the factors related to the increased risk of an attention-deficit/hyperactivity disorder diagnosis in children raised in an English-speaking household [31]. To sum up, the reasons for the different burden of mental disorders in different countries and regions are multifaceted and interactive. It includes economic level, educational level, ethnic and local psychiatric development, capacity of local medical units to diagnose disease, epidemiological data defined by specialists or primary care physicians, and level of concern and commitment to disease [32, 33]. For example, the dramatic reform of psychiatry and the development of biomedical psychiatry in Spain, as well as the establishment of the international medical union, led to widespread screening and high diagnostic rates for mental disorders in high-income Spain [34]. In addition, cultural differences between countries, with some customs and religious beliefs that regard mental illness as taboo or stigma, make disease reporting and help-seeking rare [35]. Therefore, the epidemiological data in these areas are limited and uncertainly, and it should be noted that the interpretation of database estimates in these areas needs to be cautious.
During this research, the large population-based sample and high-quality nationwide registered data were strengths of our study. Nevertheless, there are limitations in our study. First, there is bias in many ways. The original study of partial regional or national data was biased, with either higher or lower levels depending on the heterogeneity of the disease. The GBD data used in this study were obtained through the integration of a large number of epidemiological survey data and the smoothing of the blank data through rigorous statistical methods. The absence of raw data for many countries means that country and regional differences were made up of both true differences in burden and differences arising from uncertainty in the estimates because of a scarcity of data. It is expected that the database would include more high-quality epidemiological studies from around the world with standardized disease assessment methods, filling in the gaps of data for many diseases in some areas. Second, we studied a broad spectrum of mental illnesses and the associated factors, but we could not clearly explain the causal relationship of the conclusions, and the specific and practical effects of these factors on diseases could not be effectively observed using the secondary analyses of cross-sectional data and observations from the trends in data change. Therefore, we were careful in drawing conclusions about the total burden of disease. Finally, there are further limitations, such as the study did not analyze and exclude the condition of comorbidities of mental disorders. We hope that the database will be able to further differentiate between these large segments of the population since having one mental disorder can be easily combined with other mental disorders [36, 37]. Information about the children diagnosed with mental disorders most likely to come from the parents’ and pediatric professors’ observations, while many children have impaired functioning although they do not meet the diagnostic criteria for a specific mental disorder, which may lead to ignorance or exaggeration of some disease symptoms. It is necessary to notice that a mental health concern of the patient, family, or childcare and/or school personnel may trigger a preliminary psychosocial assessment. Therefore, it is suggested that fully structured interviews and blinded clinician re-interviews are preferred when gathering data in large epidemiological research [7]. As many subtypes of diseases have not been included in the GBD 2019, so the prevalence and burden of diseases could be either overweighed or underweighted, which could lead to the inaccuracy of our observations.
Taken together, we have summarized the burden of 12 classes of mental disorders globally in children and adolescents between 1990 and 2019 to describe the burden accumulation of mental disorders (e.g., anxiety disorders, major depressive disorder, and conduct disorders) over time and a high growth rate in eating disorders and also explore demographic and geographic correlations of mental disorders. Interventions aimed at the primary prevention of chronic physical diseases should optimally be integrated into the treatment of all mental disorders in primary and secondary care from early time points in the disorder course. Ameliorating mental disorders could have implications for improving life span, improvements in health span, reducing health care usage, and the financial costs associated with treating these physical diseases. Global attention should be focused on the relative burden associated with disease morbidity rather than mortality alone. The move to incorporate the effects of disease morbidity has been key in emphasizing the importance of mental disorders. An international effort to improve the mental health of populations around the world is now underway. New policies, financing, and implementation can put established best practices and numerous research findings from around the country into action.
Abbreviations
- The GBD study:
-
The Global Burden of Diseases study
- WMH Survey:
-
World Mental Health Survey
- DSM:
-
The American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders
- ICD:
-
International Classification of Diseases
- YLLs:
-
Years of life lost
- YLDs:
-
Years lived with disability
- DALYs:
-
Disability-adjusted life-years
- SDI:
-
Socio-demographic index
- UI:
-
Uncertainty interval
References
Lawrence D, Kisely S, Pais J (2010) The epidemiology of excess mortality in people with mental illness. Can J Psychiatr 55:752–760
Scott KM, Lim C, Al-Hamzawi A, Alonso J, Bruffaerts R, Caldas-de-Almeida JM, Florescu S, de Girolamo G, Hu C, de Jonge P, Kawakami N, Medina-Mora ME, Moskalewicz J, Navarro-Mateu F, O’Neill S, Piazza M, Posada-Villa J, Torres Y, Kessler RC (2016) Association of mental disorders with subsequent chronic physical conditions: world mental health surveys from 17 countries. JAMA Psychiat 73:150–158
Wahlbeck K, Westman J, Nordentoft M, Gissler M, Laursen TM (2011) Outcomes of Nordic mental health systems: life expectancy of patients with mental disorders. Br J Psychiatr 199:453–458
Scott KM, de Jonge P, Alonso J, Viana MC, Liu Z, O’Neill S, Aguilar-Gaxiola S, Bruffaerts R, Caldas-de-Almeida JM, Stein DJ, de Girolamo G, Florescu SE, Hu C, Taib NI, Lepine JP, Levinson D, Matschinger H, Medina-Mora ME, Piazza M, Posada-Villa JA, Uda H, Wojtyniak BJ, Lim CC, Kessler RC (2013) Associations between DSM-IV mental disorders and subsequent heart disease onset: beyond depression. Int J Cardiol 168:5293–5299
Cunningham R, Sarfati D, Peterson D, Stanley J, Collings S (2014) Premature mortality in adults using New Zealand psychiatric services. N Z Med J 127:31–41
Collaborators GBDMD (2022) Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatr 9:137–150
Kessler RC, Aguilar-Gaxiola S, Alonso J, Chatterji S, Lee S, Ustun TB (2009) The WHO World Mental Health (WMH) Surveys. Psychiatrie (Stuttg) 6:5–9
Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, Charlson FJ, Norman RE, Flaxman AD, Johns N, Burstein R, Murray CJ, Vos T (2013) Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet 382:1575–1586
Steel Z, Marnane C, Iranpour C, Chey T, Jackson JW, Patel V, Silove D (2014) The global prevalence of common mental disorders: a systematic review and meta-analysis 1980–2013. Int J Epidemiol 43:476–493
Kessler RC, Aguilar-Gaxiola S, Alonso J, Chatterji S, Lee S, Ormel J, Ustun TB, Wang PS (2009) The global burden of mental disorders: an update from the WHO World Mental Health (WMH) surveys. Epidemiol Psichiatr Soc 18:23–33
Wang PS, Aguilar-Gaxiola S, Alonso J, Angermeyer MC, Borges G, Bromet EJ, Bruffaerts R, de Girolamo G, de Graaf R, Gureje O, Haro JM, Karam EG, Kessler RC, Kovess V, Lane MC, Lee S, Levinson D, Ono Y, Petukhova M, Posada-Villa J, Seedat S, Wells JE (2007) Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet 370:841–850
Houtrow AJ, Larson K, Olson LM, Newacheck PW, Halfon N (2014) Changing trends of childhood disability, 2001–2011. Pediatrics 134:530–538
Baranne ML, Falissard B (2018) Global burden of mental disorders among children aged 5–14 years. Child Adolesc Psychiatr Ment Health 12:19
Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA (2015) Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatr 56:345–365
Association WDCAP (2013) American psychiatric association Diagnostic and Statistical Manual of Mental Disorders (DSM-V). Am Psychiatric Assoc. https://doi.org/10.1176/appi.books.9780890425596
Diseases GBD, Injuries C (2020) Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396:1204–1222
Collaborators GBDV (2020) Five insights from the Global Burden of Disease Study 2019. Lancet 396:1135–1159
Xu T, Wang B, Liu H, Wang H, Yin P, Dong W, Li J, Wang YX, Yusufu M, Briant P, Reinig N, Ashbaugh C, Adelson J, Vos T, Bourne R, Wang N, Zhou M (2020) Prevalence and causes of vision loss in China from 1990 to 2019: findings from the Global Burden of Disease Study 2019. Lancet Public Health 5:e682–e691
Collaborators GBDEMRAH (2018) Adolescent health in the Eastern Mediterranean Region: findings from the global burden of disease 2015 study. Int J Public Health 63:79–96
Wu J, Liu J, Li S, Ma H, Wang Y (2020) Trends in the prevalence and disability-adjusted life years of eating disorders from 1990 to 2017: results from the Global Burden of Disease Study 2017. Epidemiol Psychiatr Sci 29:e191
Johnson EL, Salafia EHB (2022) Mediating effects of intimacy between body talk and girls’ body dissatisfaction: the forgotten sibling relationship. J Youth Adolesc 51:1230–1240
Purkiewicz A, Kamelska-Sadowska AM, Ciborska J, Mikulska J, Pietrzak-Fiecko R (2021) Risk factors for eating disorders and perception of body in young adults associated with sex. Nutrients 13(8):2819
Bachner-Melman R, Watermann Y, Lev-Ari L, Zohar AH (2022) Associations of self-repression with disordered eating and symptoms of other psychopathologies for men and women. J Eat Disord 10:41
Jackson T, Chen H (2008) Predicting changes in eating disorder symptoms among Chinese adolescents: a 9 month prospective study. J Psychosom Res 64:87–95
Karam SM, Barros AJ, Matijasevich A, Dos Santos IS, Anselmi L, Barros F, Leistner-Segal S, Felix TM, Riegel M, Maluf SW, Giugliani R, Black MM (2016) Intellectual disability in a birth cohort: prevalence, etiology, and determinants at the age of 4 years. Public Health Genomics 19:290–297
Hillemeier MM, Morgan PL, Farkas G, Maczuga SA (2011) Perinatal and socioeconomic risk factors for variable and persistent cognitive delay at 24 and 48 months of age in a national sample. Matern Child Health J 15:1001–1010
Arcelus J, Mitchell AJ, Wales J, Nielsen S (2011) Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch Gen Psychiatr 68:724–731
Johnson JG, Cohen P, Kasen S, Brook JS (2002) Eating disorders during adolescence and the risk for physical and mental disorders during early adulthood. Arch Gen Psychiatr 59:545–552
Bergen DC (2008) Effects of poverty on cognitive function: a hidden neurologic epidemic. Neurology 71:447–451
Engle PL, Black MM (2008) The effect of poverty on child development and educational outcomes. Ann N Y Acad Sci 1136:243–256
Morgan PL, Staff J, Hillemeier MM, Farkas G, Maczuga S (2013) Racial and ethnic disparities in ADHD diagnosis from kindergarten to eighth grade. Pediatrics 132:85–93
Alonso J, Liu Z, Evans-Lacko S, Sadikova E, Sampson N, Chatterji S, Abdulmalik J, Aguilar-Gaxiola S, Al-Hamzawi A, Andrade LH, Bruffaerts R, Cardoso G, Cia A, Florescu S, de Girolamo G, Gureje O, Haro JM, He Y, de Jonge P, Karam EG, Kawakami N, Kovess-Masfety V, Lee S, Levinson D, Medina-Mora ME, Navarro-Mateu F, Pennell BE, Piazza M, Posada-Villa J, Ten Have M, Zarkov Z, Kessler RC, Thornicroft G, Collaborators WHOWMHS (2018) Treatment gap for anxiety disorders is global: Results of the World Mental Health Surveys in 21 countries. Depress Anxiety 35:195–208
Perez MI, Limon DL, Candelari AE, Cepeda SL, Ramirez AC, Guzick AG, Kook M, La Buissonniere AV, Schneider SC, Goodman WK, Storch EA (2022) Obsessive-compulsive disorder misdiagnosis among MENTAL HEALTHCARE PROVIDERS in Latin America. J Obsessive Compuls Relat Disord 32:100693
Baca E, Lazaro J, Hernandez-Clemente JC (2010) Historical perspectives of the role of Spain and Portugal in today’s status of psychiatry and mental health in Latin America. Int Rev Psychiatr 22:311–316
Schnyder N, Panczak R, Groth N, Schultze-Lutter F (2017) Association between mental health-related stigma and active help-seeking: systematic review and meta-analysis. Br J Psychiatr 210:261–268
McGrath JJ, Lim CCW, Plana-Ripoll O, Holtz Y, Agerbo E, Momen NC, Mortensen PB, Pedersen CB, Abdulmalik J, Aguilar-Gaxiola S, Al-Hamzawi A, Alonso J, Bromet EJ, Bruffaerts R, Bunting B, de Almeida JMC, de Girolamo G, De Vries YA, Florescu S, Gureje O, Haro JM, Harris MG, Hu C, Karam EG, Kawakami N, Kiejna A, Kovess-Masfety V, Lee S, Mneimneh Z, Navarro-Mateu F, Orozco R, Posada-Villa J, Roest AM, Saha S, Scott KM, Stagnaro JC, Stein DJ, Torres Y, Viana MC, Ziv Y, Kessler RC, de Jonge P (2020) Comorbidity within mental disorders: a comprehensive analysis based on 145 990 survey respondents from 27 countries. Epidemiol Psychiatr Sci 29:e153
Plana-Ripoll O, Musliner KL, Dalsgaard S, Momen NC, Weye N, Christensen MK, Agerbo E, Iburg KM, Laursen TM, Mortensen PB, Pedersen CB, Petersen LV, Santomauro DF, Vilhjalmsson BJ, Whiteford HA, McGrath JJ (2020) Nature and prevalence of combinations of mental disorders and their association with excess mortality in a population-based cohort study. World Psychiatr 19:339–349
Acknowledgements
We highly appreciate the work by the GBD 2019 collaborators.
Funding
This work was supported by a National Natural Science Foundation of China (NSFC) grant (Grant No: 82000754) to Dr. He Xue, a Youth Backbone Support Program of China Medical University (QGZD2018013) to Dr. He Xue, and a Jilin health talent grant (Grant No: JLSWSRCZX2021-037) to Dr. Piao Jianmin. The funders played no role in study design, data collection and analysis, the decision to publish, or preparation of the manuscript. The corresponding author had full access to all the data and had final responsibility for the decision to submit for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The authors declare that no competing interests exist.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Piao, J., Huang, Y., Han, C. et al. Alarming changes in the global burden of mental disorders in children and adolescents from 1990 to 2019: a systematic analysis for the Global Burden of Disease study. Eur Child Adolesc Psychiatry 31, 1827–1845 (2022). https://doi.org/10.1007/s00787-022-02040-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-022-02040-4