
Abstract
There is great cultural diversity across Europe. This is reflected in the organisation of child and adolescent mental health (CAMH) services and the training of the respective professionals in different countries in Europe. Patients and their parents will want a high quality, knowledgeable, and skillful service from child and adolescent psychiatrists (CAPs) wherever they see them in Europe. A European comparison of training programs allows all stakeholders in different European countries to assess the diversity and to initiate discussions as to the introduction of improvements within national training programs. Major issues to be addressed in comparing child and adolescent psychiatric training programs across Europe include: (1) formal organisation and content of training programs and the relationship to adult psychiatry and paediatrics; (2) flexibility of training, given different trainee interests and that many trainees will have young families; (3) quality of governance of training systems; (4) access to research; and (5) networking. The Child and Adolescent Psychiatry—Study of Training in Europe (CAP-State) is a survey of training for child and adolescent psychiatrists (CAPs) across European countries. It aims to revisit and extend the survey carried out in 2006 by Karabekiroglu and colleagues. The current article is embedded in a special issue of European Child + Adolescent Psychiatry attempting to for the first time address training in CAP at the European and global levels. Structured information was sought from each of 38 European and neighboring countries (subsequently loosely referred to as Europe) and obtained from 31. The information was provided by a senior trainee or recently qualified specialist and their information was checked and supplemented by information from a senior child and adolescent psychiatry trainer. Results showed that there is a very wide range of provision of training in child and adolescent psychiatry in different countries in Europe. There remains very substantial diversity in training across Europe and in the degree to which it is subject to national oversight and governance. Some possible reasons for this variation are discussed and some recommendations made.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
CAPs are the only medical specialists specifically trained to diagnose and treat mental disorders of childhood and adolescence. They bring a fully biopsychosocial synthesis of perspectives to the service of their child and adolescent patients and their families after they have had an appropriate training in child development and child mental health difficulties and illness. Thorough training is of paramount importance.
Are undergraduate medical students exposed to CAP? Many doctors make their career choices at this stage, so this is important for recruitment. In Europe, CAP is regarded as a specialty in its own right or as a sub-specialty of another major medical specialty, usually adult psychiatry. The status of CAPs in each country as separate medical specialists may affect how they are seen by other medical specialists and by stakeholders such as hospital administrators and politicians.
How are candidates selected to train as CAPs? Once selected, how are they trained as CAPs across Europe and is there substantial variation? Do the different patterns of training lead to specialists who are able to provide a breadth and standard of service in their own countries? Can they meet the standards required in other countries in Europe to be appointed in competitive interviews? What are their employment prospects if they select CAP as a career? To begin to answer these questions, there has to be a much clearer idea of what happens in CAP training in the countries of Europe and whether this is changing over time.
Training CAPs in Europe has become a hot topic in recent years. There is increasing awareness of the challenges in training faced by trainees and trainers. There is also growing awareness of different systems of training, and inter-country collaboration. This work is led by organisations such as European Union of Medical Specialists Section for Child and Adolescent Psychiatry (UEMS-CAP), International Association of Child and Adolescent Psychiatry and Allied Disciplines (IACAPAP), European Federation of Psychiatric Trainees (EFPT), and European Society for Child and Adolescent Psychiatry (ESCAP), which support training for trainees at the international level. This study takes place against the backdrop of an increase in free movement of workers, trainees and professionals in the EU. There is an increasing realisation of the importance of the framework within which teaching occurs, its governance, and the need to support trainers, none of which have been adequately researched to date.
The nomenclature used in the endeavour to raise knowledge and skills can be confusing. Training requirements for medical specialties are set nationally in Europe as each nation designates its specialists. Training standards can be agreed by any competent body. Usually, they are set by specialist organisations nationally. International organisations such as the UEMS can only lead to guidelines for training, as each state decides its own requirements. Confusingly, UEMS produces and refers to “education training requirements” (ETR) for each medical specialty. In reality, these are guidelines, as they cannot be enforced.
There has been increasing effort to understand training differences, to drive up training standards and to harmonise training requirements through persuasion of nation states. While this is not a new endeavour, it has evidently become a more pressing issue. Several groups have looked at the current state of European training [1,2,3,4,5]. Associated with these, there have been initiatives to agree training standards across Europe and encourage a contemporary, relevant training. For example, the UEMS-CAP Section has representatives from all the European Union countries. It has supported training by developing a curriculum framework, i.e., guidelines for topics and skills to be covered within which national curricula can be set. It has also provided a model log book [6]. This also supports trainees in advocating for the realisation of these standards, a project in which the EFPT has been active. MindEd has developed online training resources with substantial material appropriate for trainees [7]. IACAPAP has developed an evidence-based textbook [8], readily available internationally. Several international groups have advocated improving training standards and the use of competencies 7–10]. Others have focused on key clinical areas providing guidelines for practice and training in specific areas [11,12,13,14].
Aims of this study
Given the rapid changes in CAP services and training in Europe and the advent of new UEMS-CAP training requirements in 2014 [15], this study aims to provide an updated and enlarged 10 year follow-up of the previous research on CAP training in Europe, completed in 2006 [16]. We report on changes over the last 10 years. We explore a broader and deeper understanding of the complex issues highlighted in the 2012 paper [10] by the EFPT through exploring trainers’ situations, training institutions, and build on work surveying trainees regarding training initiatives and needs [10, 17].
As the UEMS-CAP curriculum framework [15] has been agreed by senior CAPs appointed as representatives across Europe and ratified by UEMS in 2014, this offers a template against which to understand the findings in this study.
The value that each country places on its future health may well be reflected in its spending on some groups of more vulnerable citizens including its children and young people. There is a considerable and increasing interest in and awareness of the importance of child mental health in Europe, e.g., [18]. There is some realisation of its economic costs if not adequately addressed. This study also offers an opportunity to examine the variability of investment in child mental health across Europe.
Materials and methods
The CAP-STATE project was initiated by the ESCAP Research Academy. One motive was the formation of a research network among the attendees of the 2015 meeting of the Academy in Madrid. Three international core group members (Barrett, Hergüner, and Klasen) coordinated the design and data collection. A trainee or recently qualified child psychiatry specialist from each ESCAP member state in attendance participated. Where there was no attendee from a European country that had participated in earlier studies, see Table 1, these were recruited through ESCAP member organisations. They were asked to collect the data on CAP training for their country. Co-authors provided data in a representative capacity (they were instructed to check national curricula and consult with residents and trainers from various university and peripheral training schemes to collect reliable data on CAP training throughout their country). This strategy has been used in the previous surveys. They were required to cross-check information with a senior colleague familiar with national training standards (such as the university chair of child and adolescent psychiatry, a regional or national training director) who would co-sign the final data submitted. The respondent and the supervising respondent were aware of the need to check final responses for accuracy. Where a representative stated that there were significant variations within their country, they were asked to describe these.
National data collectors were provided with a web link to the survey. Several reminder emails were sent to participants. Following completion of the data collection questionnaires, the core group members reviewed all responses and provided support regarding queries. Final opportunities to review all data were provided to participants in January 2016 prior to data analysis. An additional opportunity to check data for accuracy as applying to the data collection window (June 2015–January 2016) was given to all participants after the initial analysis of the data and again during the write up stage. Each co-author was responsible for the accuracy of the data reported for their own country. Changes that had taken place subsequent to the survey window were not included. Some clarification of answers was undertaken subsequently, but the data all related to this collection period. During the analysis, outlying data in relation to the length of training was checked with the submitting nation’s co-author. Its accuracy was confirmed, and the data were included.
Participants
The invited participants in this study were 31 national societies in ESCAP, six countries which are not in ESCAP, but participated in the 2006 survey, and one country that provided a representative, but is not yet part of ESCAP (Macedonia) [19]. Thus, a total of 38 countries were asked to participate in CAP-STATE: Albania, Austria, Belarus, Belgium, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Israel, Italy, Latvia, Lithuania, Macedonia, Netherlands, Norway, Poland, Portugal, Romania, Russia, Serbia Slovakia, Slovenia, Spain, Sweden, Switzerland, Turkey, Ukraine, and UK.
Data from five countries (Finland, Hungary, Iceland, Russia, and Slovakia) could not be included in the analysis, as there were no responses to the survey. The information from Spain and Cyprus has been excluded from most of the analysis, because there was no separate specialty or sub-specialty of CAP recognised at the time of the survey in Spain, despite ongoing efforts to achieve this and Cyprus had no CAP specialist training scheme on the island. Some basic information was provided, and where this represented the current situation at the time of the survey rather than future plans, this was included.
Respondents were trainees (21, 58%), early career CAPs (9, 25% within 3 years of completion of training) or were more senior consultants (6, 17%). All recorded their supervising consultant, i.e., the person with whom they cross-checked the answers for their country. One respondent was a clinical psychologist (Macedonia) who verified her input with the head of department of CAP.
Tool: the survey questionnaire
Following review of recent publications, an online survey tool exploring key areas was developed by the core team using encryption and a designated weblink. It was initially piloted amongst some participant countries. The survey questionnaire included both quantitative and qualitative aspects regarding the training of CAPs, the training centres and the trainers in each country. During the pilot phase, all co-authors reviewed the survey tool to ensure that they fully understood the questions and provided feedback regarding the survey. Following this pilot, a revised questionnaire was circulated to all participant country representatives. The final questionnaire consisted of 69 items (available as supplementary material).
Items were for the most part categorical data (e.g., is a logbook utilized? yes/no/recommended) and in some instances continuous (e.g., what is the required length of training in months?). Qualitative questions enabled participants to give a more detailed description of certain aspects of their training and add to the topics covered in quantitative questions (e.g., “Please describe how psychotherapy training is organised in your country”).
The survey covered the following subject areas:
- 1.
country information regarding numbers of child and adolescent psychiatry specialists and population of each country;
- 2.
undergraduate exposure to CAP;
- 3.
separate specialty vs. sub-specialty;
- 4.
initial recruitment to CAP and duration of training,
- (a)
recruitment and selection,
- (b)
training duration,
- (c)
part-time training.
- (a)
- 5.
training composition,
- (a)
components of training,
- (b)
theoretical knowledge,
- (c)
practical skills,
- (d)
research,
- (e)
international exposure/ conference opportunities,
- (f)
supervision,
- (g)
assessment,
- (h)
skills to practice child and adolescent psychiatry.
- (a)
- 6.
training centres: organisation and oversight,
- (a)
requirements of supervisors,
- (b)
appointing training centres,
- (c)
facilities for trainees,
- (d)
trainee supervision ratios,
- (e)
monitoring of schemes,
- (f)
perceived variation within countries,
- (a)
- 7.
Employment prospects following training.
Gross domestic product (GDP) was taken from the International Monetary fund data for 2017 [20].
Analysis and data presentation
Data were captured and stored using industry standard encryption technology. Statistical analysis was descriptive using SPSS for Windows, version 17.0 and SPSS 24.0 (SPSS Inc., Chicago, Illinois, USA). All percentages are rounded to the nearest whole number. Pearson correlation was used for continuous variables; univariate analysis of variance was used as appropriate.
To examine the overall level of provision of CAP specialists in relation to the wealth of countries across Europe, univariate analysis of variance was employed using SPSS. To account for varying child populations as a proportion of the whole country’s population, the provision was primarily related to the population under age 18, information provided for each country by the respondent to the survey.
Results
Full or nearly complete data sets were received from 31 countries.
- 1.
Country information numbers of CAPs, population size, and GDP
There was considerable variability in the number of specialist CAPs in the 31/31 countries for which we had this data, ranging from 10 to 2502. Relating these to the population aged < 18 years, there was a very wide range from 2648 (Switzerland) to 78,950 (Bosnia and Herzegovina) per child and adolescent psychiatrist with a median value of 15,867 (Table 1).
The number of CAPs was calculated for each country’s Gross Domestic Product per size of the non-adult (< 18 years) population. For the 31 countries, where an estimate of the number of CAPs was available, univariate analysis showed that GPD per child under 18 predicted the number of CAP specialists in the country. (F = 7.37, p = 0.017). This relationship also held when GDP was related to the total population (F = 11.8, p = 0.006).
Table 1 Number of child and adolescent psychiatrists in European and neighboring countries in relationship to population size (including the underage population) and gross domestic product (International Monetary Fund) - 2.
Undergraduate exposure to child and adolescent psychiatry
For 23/31 countries (74%), there was a formal requirement to teach CAP at undergraduate medical school; a further seven countries recommended this nationally, but it was not a requirement of medical schools. Only 11/31 required clinical exposure of the undergraduate medical students to CAP, with another nine countries recommending this. Electives with increased exposure to CAP were offered in 17/31 (55%) of the countries.
- 3.
Speciality vs. sub speciality
24 (73%) of 33 responding countries recognise CAP as a separate specialty in medicine. In a further eight countries, it is recognised as a sub-specialty of psychiatry including Bosnia Herzegovina, where CAP is either a distinct specialty or a sub-specialty depending on the region. In one country (Spain), CAP was not recognised as either a separate specialty or as a sub-specialty of psychiatry when this survey was carried out (see “Materials and methods”).
- 4.
Recruitment and selection, training duration, and flexible training in child and adolescent psychiatry.
- (a)
Recruitment and selection
After basic medical qualification, the stage of entry to postgraduate training in CAP varied (Table 2). So did the criteria used to assess the candidates for CAP specialist training and whether the entry was organised to a national standard, a regional standard or at the level of individual training centres.
Table 2 Selection to train as CAPs - (b)
Training duration and location
There were significant variations in the length of required training after basic medical training to qualification as a specialist in CAP, whether any adult psychiatry training was a necessary part of training, and the obligatory time in this or other fields such as paediatrics (Fig. 1).
Fig. 1 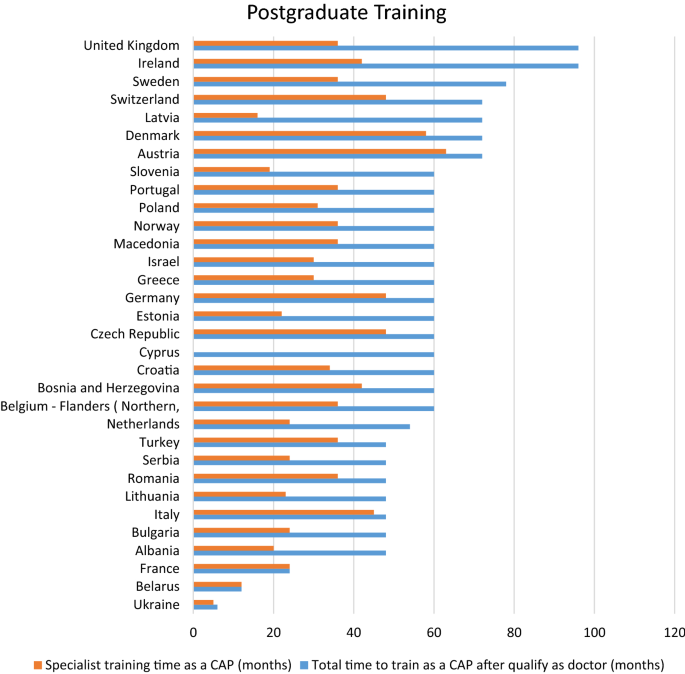
Length of postgraduate medical training
The minimum mean time postbasic medical qualification including training in psychiatry, paediatrics, or other fields to achieve a CAP specialist role was 4.7 years. The shortest and longest overall training times were found in Ukraine (6 months from qualification to specialist status) and in Ireland and the UK (8 years). The mean training time in CAP itself among the countries surveyed was 33 months (range 5–63 months) with the shortest trainings in Ukraine (5 months) and Bosnia Herzegovina (12 months) and the longest in Austria and Denmark (63 and 58 months, respectively). Both the length of post-qualifying training time to be a specialist CAPs (F = 9.3, p = 0.005) and of the specialist training time in CAP itself (F = 12.8, p = 0.001) were related to the GDP per child under the age of 18 years.
- (c)
Part-time training
Part-time training was definitely possible in 7/30 (23%) countries; it was not possible in 19 (63%) countries and could be achieved with difficulties in the remaining 4 (13%) countries.
With regard to appointable applications, the 25 countries that gave clear responses split more or less evenly into three groups of those with (a) too few training places; (b) more training places available than applicants; and (c) a balance between number of appointable applications and places. The perceived balance of training posts to demand for training did not vary significantly with the number of under 18 years in the population on univariate analysis (F = 0.474, p = 0.498)
- (a)
- 5.
Training composition
- (a)
Components of training
Many countries mandate the time spent in some CAP practice settings and in adult psychiatry. For example, 94% of countries require outpatient CAP experience. The time required varied widely between 4 months and 30 months (mean 16.4 months, SD 8.4) among the 19 countries that specified a minimum time in outpatient settings. Nearly, all countries required inpatient experience; among the 23 countries that specified a minimum time for this experience, the length varied widely (1–60 months, mean 14.6 months SD 12.4). 29 countries specified a period of training in adult psychiatry. The range was between 1 month and 36 months (mean 13.2 months SD 9.6).
- (b)
Theoretical knowledge
Of the topics suggested in the UEMS-CAP curriculum framework, there was broad coverage of knowledge for core clinical topics such as diagnosis, epidemiology and aetiology, pharmacotherapy, and the psychotherapies (Table 3). For 7 out of 21 areas of the curriculum framework, more than 80% of countries provided theoretical teaching “usually or always”. For four areas of the curriculum framework, the teaching reached this level in 50–80% of countries, while in seven areas, it fell below 50%.
Table 3 Topics taught by percentage of countries (based on valid responses from 31 countries) - (c)
Skills in practice for child and adolescent psychiatrists
The range of practical skills training focused on clinical skills including interviewing (diagnostic and treatments) and pharmacological skills (Table 4). Management, leadership, and teaching skills were much more sparsely taught (around one-third of the 31 countries). Trainees were required to observe senior colleagues’ clinical practice in 11 countries (36%); it was specifically recommended in 16 (52%) and not required in the remaining four countries (13%).
Table 4 Practical skills training 28 countries reported data on training for any of the psychotherapies. 12 required practical training in individual psychotherapy with children and seven recommended it (68% combining the categories). The type of individual psychotherapy was not specified. 27 countries reported training on systemic therapy. Six countries required this training and a further five countries recommended it; this represented a combined percentage of 41% of those reporting figures. With regard to supervision of psychotherapy, four countries required supervision if the trainee undertook psychotherapy even though it was not required for the training. On the other hand, seven countries did not require supervision of psychotherapies, even though they were required or recommended for the training.
In 94% of respondent countries, trainees can initiate medication during their training.
- (d)
Research
Of the 31 countries reporting, 14 (45%) required the trainee to undertake a research project; a further nine countries (29%) recommended this, while eight countries (26%) had no research specified element in the training.
- (e)
Opportunities for international conferences and electives
In 72% of the countries surveyed, trainees could attend international conferences in employer’s paid time with funding. 27% could not attend such meetings, for lack of study leave and/or funding. International experience could be provided by 21% of countries with ease, while 71% of countries had difficulty offering this.
- (f)
Supervision
All trainees received some clinical supervision (Table 5). This was regulated in most countries, but the amount of formal and informal clinical supervision varied widely across Europe (see Table 4). Several countries appear to offer infrequent supervision only.
Table 5 Clinical supervision - (g)
Assessments of trainees
A variety of approaches are used across Europe to assess trainee progress formally (Table 6). Written examinations during or at the end of training were undertaken in 12 (39%) of the 31 countries responding. Oral summative examinations were required in 23 countries (74%). Six countries (31%) required trainees to take written, oral and clinical examinations, while seven countries relied on structured assessments of trainees’ practice during of training. The nature, timing, and content of these oral and written examinations was quite variable. Equally, there was considerable variation in whether they were organised locally, regionally, or nationally. Four countries recommend or require the use of Objective Structured Clinical Examinations (OSCEs), 24 countries use case discussions as part of a summative assessment, while nine countries recommend or require the use of review of video material (29%).
Table 6 Assessments of training 19 countries (61%) have a system to provide feedback to a trainee who is struggling with the training, while 13 countries (42%) have a formal process to support a trainee in difficulties with the training. Respondents were also asked to provide written information on the feedback process for struggling trainees. The nature of review, support, and action was depicted as very variable between training schemes and between countries ranging from additional supervision through having to repeat a year of training, to being counselled out of training.
On successful completion of specialist, training 22 countries (71%) maintain a national specialist register, for which the trainee is eligible.
- (a)
- 6.
Training centres: organisation and oversight
- (a)
Requirements for supervisors
Trainers have various measures applied in the different countries across Europe to assess their ability to supervise trainees (Table 7).
Table 7 Requirements of trainers - (b)
Trainees supervised
The survey requested information on the number of trainees supervised by each training supervisor. Of the 28 countries that provided information, 15 (48%) set the number of trainees for each supervisor which usually ranged between 1:1 and 1:3, the latter in a few countries. One country reported a ratio of one supervisor to nine trainees.
- (c)
Facilities for trainees
Most countries (21/31) required the trainee to have the use of a computer with internet access, seven countries recommend, this but three countries (10%) are silent about the need of this for trainees. Virtually, all countries require or recommend access to a library in the training institution (18 of 31 countries and 12 countries—58% and 39%, respectively). Twenty countries (65%) require trainees to have facilities to carry out a physical examination. However, six countries (19%) neither require nor recommend this.
- (d)
Appointing, funding, and monitoring of training schemes
In most countries, the training is paid for by public authorities, but in 10% (3/31) of the countries, some or all trainees have to pay a substantial part or the full cost of the theoretical teaching they receive (other aspects related to organisation and oversight of training centres, see Table 8).
Table 8 Appointing, funding, and monitoring of training schemes - (e)
Perceived variation in training within countries
Correspondents and their senior reference colleagues were asked to agree on the degree of variation in the training experience in different centres within their country. 13 countries (42%) regarded training as consistent across their country, though two of these countries only had a single training scheme; 16 countries (52%) described considerable variation in the application of national and European guidelines. The remaining two countries perceived there to be a high variation with little or no use of national guidelines in training.
- (a)
- 7.
Employment following training
25 countries (81% of trainees) report that most trainees in their country find a paid post at the end of training, while six countries (19%) found it difficult for newly qualified trainees to find specialist work once trained.

Discussion
An interest in understanding the provision of medical training across Europe is fairly recent. It has been given impetus by the creation of the European Union. There has also been a recognition of the need for high standards of clinical practice. The increased mobility of professional people in the modern world including specialties across medicine has focussed interest in this topic. Other influences have probably included increased scientific contact internationally, at a personal level, through collaboration and joint publications. The issues are captured in the statutes [21] of the Union Européenne Des Médecins Spécialistes, an organisation created in 1958 to “Promote the interests of each medical specialty; define European Medical Standards in each medical specialty and to promote the highest standard of training at the European level.” UEMS-CAP and ESCAP both work with these aims in mind for Child and Adolescent Psychiatry in Europe. It needs to be pointed out that little scientific data are available on what constitutes good training. However, there is some convergence from unconnected training systems in different parts of the world, e.g., the curricula in the United Kingdom, Sweden, Australia, and New Zealand.
The current study represents an update and expansion of the first significant survey of the education of CAPs undertaken by ESCAP in 2006. It develops further questions raised by the international trainees’ organisation (EFPT) in their study dated 2012 [10]. It attempts to look in greater detail at recruitment of trainees and the composition and delivery of training. It examines trainee experiences on the ground, the supports for trainers and training institutions and it aims to identify key challenges. Overall, the variability of training throughout Europe is substantial, particularly in comparison with, for instance, Australia (Rao et al., current issue), China (Zhang et al., current issue), India (Sagar et al., current issue), and the USA (Hunt et al., current issue). Whereas this reflects the national diversity inherent to Europe, we deem it important to foster close consideration of differences in training and suggest that they need considerable justification, where they differ across Europe. Such efforts would be likely to raise the standards experienced by patients and their families; furthermore, clinical and research efforts would profit and render Europe more competitive in a globalized world. Last but not least, this would foster cross-national training programs [22].
Clearly, this study shows that the number of CAPs on the ground varies widely from country to country. For example, the country ratios of the total number of CAPs per population number of minors (≤ 18 years) varied widely from one per 2648 in Switzerland to one for 78,950 in Bosnia and Herzegovina (Table 1). Overall, these differences are poorly understood. We assume that they likely impact on service provision to young people and their families. Factors such as funding, the nature of care provided, the availability of alternative service pathways (e.g., paediatricians, psychologists, social workers trained in mental health care provision, etc.) and socio-political commitments to the welfare of children are beyond the scope of this study, but likely to be important. A future survey, which does not focus on training, should attempt to provide an overview of national mental health services for children and adolescents to better enable cross-country comparisons and to provide a contextual framework for national assessment of the ratios of the number of CAPs per capita. Our data only allow a comparison for the field of CAP, which has historically evolved in different ways between countries and even within regions of a particular country. We assume that these historically different roots contribute to the observed variation of the ratios; we think it unlikely that they provide a full explanation of the variation. It is perhaps encouraging that the GDP per child under 18 predicted the number of CAP specialists in the country; this may hide under-provision in some countries. This topic should be further explored in future studies.
The number of adult psychiatrists per 100,000 inhabitants varies from 30 per 100,000 in Switzerland and 26 in Finland to 3 in Albania and 1 in Turkey according to an article focusing on training in adult psychiatry [23]. Despite adult psychiatry being the largest medical specialty in Europe, the authors similar to our own conclusions state that “by no means yet are there common standards nor requirements for training and certification that are recognised and implemented in all countries across Europe. The reasons are diverse, but cultural and political insights and influences account for these differences”. The authors stress the need to particularly promote training in psychotherapy within adult psychiatry across Europe. It is beyond the scope of this article to assess if the variation across Europe in CAP training is similar to or exceeds that in other medical specialties. A comparison with adult psychiatry would appear of particular interest to assess if the differences across Europe parallel those observed for CAP.
Undergraduate exposure and recruitment into CAP
Recruitment into CAP remains an issue. Many physicians understand the importance of exposure to a particular discipline within medicine during undergraduate medical training. It tends to influence later career choice/specialisation. Experience in CAP at medical school is variable across Europe. Only about a third of the countries in the study required exposure of medical students to clinical practice. This is likely to have an impact on later recruitment relative to other specialties, where experience is a universal requirement.
There are high levels of child mental health impairment in society, running currently at ten to somewhat over 20% [24, 25]. Therefore, we need to clearly promote knowledge of mental health disorders/issues in childhood and adolescence among all medical students. In this context, the availability of structures and personnel to achieve this goal within medical faculties is crucial. Though not specifically examined, the limited exposure of medical students to CAP might suggest that the teaching resources to achieve this are not in place. Organising elective opportunities for medical students should be further encouraged; comparisons of the availability and type of these opportunities between countries may help generate ideas for achieving this.
There were wide differences in national organisation of selection, specification of criteria for selection and the application of the respective criteria. These are likely to lead to different groups of young doctors being selected to train in different countries across Europe. With regard to selection, the 25 countries that gave clear responses split more or less evenly into groups with too few training places/those with too many and with unfilled places/countries, where the perceived number of appointable applications and places was balanced. Several countries referred to there being unfilled training opportunities and too few specialists in CAP for the population. This suggests that the specialty is not attracting enough applicants in a number of countries across Europe. This might reflect overall problems of the respective national health care systems, a relatively low status of the field of child and adolescent psychiatry in medicine, to features of the training itself or other influences.
Duration and composition of training
This survey points to a wide variation between countries in the length of training to become a specialist in Child and Adolescent Psychiatry. UEMS-CAP recommends a minimum of 36 months specialist training within CAP. Economic reasons (GDP per person aged < 18) were associated both with the time for full post-qualifying training and even more strongly with the time spent in specialist CAP. It must be questionable whether adequate specialist training can be safely achieved in 6–12 months. Countries with the longest specialist training in CAP may wish to consider whether the additional time is well spent. Some competencies might be met in a different way, possibly as continuing professional development during a specialist career. On the other hand, it does take time to develop and integrate the range of skills that an independent CAP specialist needs. The UEMS-CAP European Training Requirements (ETR—i.e., the Europe-wide guidelines to nationally mandated bodies), agreed by nationally appointed senior CAP educational representatives from across Europe are clear that “normally training in child and adolescent psychiatry will take a minimum of 3 years of work with children and young people. If training is proposed to take less time, then this must be robustly and evidentially justified in terms of the role of the consultant independent practitioner” [15].
The European Commission recognises Child and Adolescent Psychiatry as a separate specialism within medicine, separate from Adult Psychiatry and its sub-specialties [26]. This change in status was subsequent to the survey published by Karabakiroglu et al. in 2006 when two-thirds of 34 countries recognised Child and Adolescent Psychiatry as a separate specialism. Despite the legal change in 2005, the proportion recognising the specialty has not changed much in the past decade. For a number of countries, it has continued to be recognised as a sub-specialty of psychiatry. Only one country still did not recognise it as either a specialty (Spain) or sub-specialty.
It is also striking that only a fifth of countries require prior adult psychiatry experience before a trainee can specialise as a CAPs. There is an increasing understanding of the roots of adult mental health difficulties in children and youth. CAP trainees need to recognise adult psychopathology for two reasons; the parents of their patients may have difficulties. In addition, we know that much of adult mental illness begins in childhood and adolescence [27]. We, on the contrary, suggest that adult psychiatrists should gain significant experience in training of CAP. Their patients’ children are at greater risk of mental health difficulties; an adult psychiatrist can encourage their patients to establish a contact to a CAP. Accordingly, an adult psychiatrist should have received some training as to normal and abnormal behaviour of children and adolescents, all the more because mentally ill parents may be experiencing stress related to their childrens` behaviour. An understanding of neuropsychiatric developmental disorders is increasingly recognised as important for all trainees.
Where it is possible, we also see the value of other experience, such as in paediatrics to improve the skills of CAPs in the physical care of their patients. Numerous psycho-somatic conditions come to the attention of both specialties. Such experience helps to foster communication and mutual understanding between child and adolescent psychiatrists and paediatricians. We found considerable variation between countries about whether experiences in other specialties allied to CAP (such as paediatrics and paediatric neurology) are required or desirable in training. To some extent, this will be influenced by the scope of allied medical specialties but the extent and the reasons for this variation warrant careful re-examination in each country.
Within child and adolescent psychiatry training, the balance between inpatient and outpatient experience also varies widely between countries across Europe. This may reflect the historical availability of services, but it may not represent an optimal approach to training future specialists. In well-developed, integrated services, the substantial majority of practice occurs in outpatient child psychiatry settings. It is appropriate that trainees gain significant experience of inpatient child and adolescent psychiatry. It is not appropriate that the majority of their training takes place in such settings.
Composition of training and curricula in practice
There remains huge variability around duration and composition of training. In particular, logbooks and demonstration of competency is not a requirement in all countries, examination systems are highly variable. Most but not all countries now have a national curriculum for training CAPs. There are too many neglected areas of the curriculum currently. It is also surprising that direct observation of seniors at work and by seniors directly viewing the skills development of trainees are not yet used routinely across Europe among training methods.
Perhaps, now, in the 21st century, each country should consider developing a national CAP curriculum. In some countries, there may be an argument to vary this by region on the basis of very real cultural differences. In such cases, we would argue that each region should carefully consider the variations and should bring their training into line with the European level agreed curriculum framework [6, 15]. A competency-based curriculum provides the trainee with the scope of what is to be learned, the trainer and training organisation a clear guide to what they have to teach and develop the trainee’s skills. Finally, and most importantly, it guides the public on what knowledge and skills that they can expect of a CAPs. It seems that there is still considerable scope for increasing harmonisation of national curricula to the UEMS-CAP curriculum framework [15], whose use should help to develop national curricula and contribute to harmonisation of standards in training across Europe.
There are also real risks of harmonisation of training to some countries, in that their doctors may wish to travel to other parts of Europe or elsewhere in pursuit of higher income and/or a different lifestyle. This creates a very real cost for the nation that has trained the specialist and difficulties staffing their own services. Perhaps, other means of retaining specialists could be used other than making the training incompatible with practice elsewhere and possibly of a lower standard. For example, there might be a requirement to practice in the home country for a period or face repaying the costs of the training that the young specialist has received. Many countries struggle to provide sufficient CAPs for their needs. Some respond by accepting a poorer level of service provision.
There are several areas within the UEMS-CAP curriculum framework, where only a minority of countries provides teaching of theory. Three that seem particularly important are leadership and management training, teaching others, and research theory. Both theoretical teaching and skill-based teaching appear deficient in more than half the countries surveyed that are training future specialists. Most CAPs are likely to take on leadership or management roles during their career and it would be wise to introduce them to training in this area early in their careers. Similarly, CAP trainees are likely to have teaching roles. They may teach and support future psychiatry trainees or teach other professions. Much is now known about adult learning and teaching skills. These are taught in fewer than 25% of European countries. Because many countries in Europe have difficulties in recruiting CAPs into research, it would seem important to include research theory into the curricula.
Teaching of practical skills
This survey has provided a more detailed picture of skills teaching than the 2006 Karabekiroglu survey [16]. For clinical skills, the coverage of the UEMS-CAP curriculum framework [15] across European countries is mostly acceptable. However, when it comes to other skills such as teaching about management skills, leadership and the knowledge, and skills to teach adult learners, the teaching is much less comprehensive. This should be improved across many European countries. These authors recognise that teaching these skills can be difficult given the sensitive nature of significant parts of managerial work and thus limited opportunity to shadow those in management positions. More thought and creativity can provide good management training to equip a specialist to be effective in the systems in which they will practice. It is also perplexing that teaching skills are not widely taught. This is difficult to achieve without adequate support and necessary resourcing of trainers and training centres. There are limited numbers of CAPs in many European countries; a specialist is likely to have to support a range of professional disciplines in a variety of settings to work with this young population.
Research training is not universal, perhaps surprisingly. To support evidence-based practice and understand the role of research in clinical and academic practice, as a profession, we must consider whether research skills (its strengths and its limitations, and appraisal of same) should be a mandatory part of training. We believe that this would support trainees to support their patients and their parents with judicious evidence-based approaches based on reliable information, where it is available, rather than on the basis of historical precedent. An early exposure to research training may help to boost the number of young CAPs willing to actively participate in research. Furthermore, the substantial national differences in research output [28] might be reduced. For these reasons, there are many references to the importance of understanding research in the UEMS-CAP Curriculum Framework, e.g., “The doctor will have the knowledge, skills and experience to analyse and appraise the research literature in child mental health and will undertake a piece of work to demonstrate this to an academic standard” [6].
Supervision, international exposure, and supporting trainees on the ground
It is encouraging that over 70% of countries now require formal supervision at least weekly. However, some countries still rely on informal arrangements. Given the importance of supervision for clinical development and helping trainees to think about their training and careers, the remaining countries should be encouraged to put in place formal supervision arrangements, so that trainees do get at least an hour weekly of supervision from a qualified CAPs. This time should be devoted to the needs of the trainee(s); it should be provided in addition to indirect training such as during rounds [15], p 7. This study has not further explored links with burnout and training, though this area merits further exploration—lack of supervision has been associated with trainee-reported burnout [29].
It is still quite difficult for trainees to gain international experience. This is probably a missed opportunity and short-term electives abroad would be likely to enhance training if the language difficulties can be surmounted. The ESCAP Research Academy [30] tries to bridge countries by providing young investigators throughout Europe and beyond with an opportunity to follow-up on cutting edge science and to form a network among the attendees (this article provides an example the potential of such networks to perform cross-country comparisons with respect to CAP). The EFPT Exchange Program offers around 65 vacancies across 16 countries in all major fields of clinical psychiatry, including child and adolescent psychiatry [31].
Many countries still do not offer the opportunity to train part time/in a flexible way. This is important, especially as CAP tends to have more women as specialists. Current training requirements may interfere with a couple’s ability to start or manage a young family. Unfortunately, the UEMS-CAP current training requirements are silent on this matter [15].
Assessment
The assessment of trainees during their training again showed considerable variability. Just over half of countries mandate that their trainees’ clinical casework is assessed; when countries that recommend this are included in the analysis, the proportion rises. There were still several countries, where this did not occur.
There has been an increase in the use of examinations as the route or a component of recruitment (35–45% of countries) to child and adolescent psychiatry training. The use of an exit examination on completion of training has not changed much, but this survey indicates that the majority of these assessments are by oral examination alone, data that were not sought in 2006 [16]. There is some question as to whether this situation is adequate, given some limitations of the oral examination approach [32]. There may be better ways to assess clinical competence. Viewed from the perspective of parents and patients, this patchy provision of assessment across Europe seems unsatisfactory. Would parents and families want or expect all trainees to be assessed to similar clinical standards across their country or even across Europe?
Training centre oversight, organisation, and thoughts about support
Overall, the majority of European countries identified much variation within countries in the delivery of training between training centres. This suggests that there is at least considerable flexibility in the national oversight of training schemes and in their governance. It may reflect an insufficient level of national oversight. It is likely that CAP will be subject to similar levels of oversight or the lack of it as may exist in other branches of medical specialist training in a particular country. Where this true, it could have wider implications for the organisation of medical specialist training in countries across Europe.
It is striking that 35% of the European countries surveyed still have no monitoring system covering the courses and organisation of the providers of specialist training in child and adolescent psychiatry. In each country, there is a different balance between the regulatory authorities for medical postgraduate training, the universities, and clinical systems. Perhaps, this contributes to the inconsistencies highlighted with respect to assessment systems. It also likely affects various different organisational arrangements of training systems in the different countries across Europe. There is a perception that there is considerable variation in training between centres within countries as well as between countries. Again, this is likely to reflect the variability in levels and types of monitoring of the training schemes. It would be useful to try to identify structures that result in improved quality of training [33].
In the light of the differences found in training across Europe, it would appear desirable to develop an online curriculum accessible to CAPs in training throughout Europe. Lectures available online would help to improve knowledge and practice throughout Europe.
Are variations justifiable on the basis of cultural and societal differences?
The UEMS-CAP Curriculum Framework [6] page 5 clearly states that CAP training should aim for a high level of skill in “5) The doctors will take into account issues of culture and diversity as they affect individual children, adolescents and families in the particular society in which they live”. A question arises as to whether this justifies some of the wide variation in extent and style of training currently seen in Europe. To these authors, this seems questionable. Can it be justified that most of training in some countries still takes place in inpatient services? It could be argued that this is where child psychiatry is provided in these countries, so that it is culturally appropriate. UEMS-CAP training requirements state “An ongoing caseload of 25–35 cases is normally appropriate during training with an annual number of assessments of about 75 cases as a guideline. In inpatient settings, the caseload will be lower. Trainees should aim to see at least ten cases of each common disorder and five cases of each of the less common disorders during their training”. It is unlikely that these required levels of experience can properly be achieved with trainings provided largely in inpatient settings.
Strengths and limitations
Strengths of the CAP-STATE study include that it is a follow-up of countries that participated in the original study 10 years prior to this study, the consistency with previously reported results and the breadth of the data set. It has recognised the difference between stated curricula and training in practice due to its foundation on data provided by trainees. In contrast to the previous work, it has included wider issues such as trainers and their qualifications, standards required of training institutions, and national supports such as the availability of a curriculum. It provides a toolbox to support practical outcomes. Practicalities such as the availability of part-time training, resourcing of supervision etc., are explored. Last but not least the financial support of training is explored. This study has begun to search correlational patterns between factors related to CAP organisation of care on one hand and CAP training on the other hand.
Limitations to the study include that the data were collected by one trainee or recently qualified specialist working with a senior trainer in each country. As co-authors and data collectors, they received instructions to collect information throughout their country and to check with national curricula and other published information. There was, however, no prescribed methodology on how data collection per country should be performed and the methods used to obtain accurate data in each country might differ to a certain extent. The questionnaire was in English, so that there is a possibility that there will have been language misunderstandings. Attempts to minimize bias included having a senior trainer as well as a trainee or early career psychiatrist sign the submitted survey for accuracy of information. This is similar to approaches taken in the previous studies.
The number of countries that submitted valid returns for the CAP-STATE survey was slightly reduced from those of Karabekiroglu 2006 [16]. The method of data collection varied in that the junior colleague in each country was not necessarily the EFPT Child and Adolescent Psychiatry representative, nor was the senior colleague the UEMS-CAP representative, but the principle of using a relatively junior and a relatively senior person from each country was used.
Recommendations
We recommend that:
- 1.
CAPs should work towards recognition of CAP as a specialty in its own right. This does not mean that we recommend training CAPs in isolation from linked professions, particularly adult psychiatry and paediatrics.
- 2.
There should be an agreed national curriculum in all European countries for which the UEMS-CAP framework should serve as a template. This will require negotiation and sensitivity, where there is regional variation. If the focus is kept on patient and family needs, we think that it is achievable and represents a worth-while pursuit.
- 3.
It would represent a step forward to introduce online training programs that were developed within a European collaboration between CAPs trainers; such an endeavour would likely have the ‘side effect’ of reducing the substantial diversity in Europe and at the same time form a more coherent European field of CAP.
- 4.
Part-time training must become readily available to maximise the number of good, high-quality specialists in the field.
- 5.
Supervision should be weekly, provided on 1:1 basis and become an integral part of training.
- 6.
Supervision of psychotherapeutic skills, of whatever style of intervention should be available. This is not only a training issue, but also concerns patient safety.
- 7.
Exchange of training ideas across Europe among trainers and trainees should be fostered, e.g., building on current initiatives of UEMS-CAP and the EPFT exchange program).
- 8.
Research training is essential, not to produce more CAP researchers, although that too is needed, but to ensure that all practitioners are research literate and can interpret new research, as it is published and change their practice if required. CAP will never become an evidence-based undertaking without this.
- 9.
Future research:
- (a)
Should assess if the countries that provide clinical exposure to undergraduates better attract physicians to the field of CAP.
- (b)
Comparison of the CAP-State results with those in adult psychiatry and potentially other medical fields.
- (c)
Identification of best practices for training in CAP by promotion of cross-country studies.
- (d)
Should further explore correlations between the organisation of care in Child and Adolescent Psychiatry and the training of CAPs, e.g., in recruitment, variation in training and its organisation, etc.
- (a)
Change history
19 January 2020
The original article has been corrected.
19 January 2020
The original article has been corrected.
References
Brittlebank A et al (2016) Training in psychiatry throughout Europe. Eur Arch Psychiatry Clin Neurosci 266(2):155–164
Hill P, Rothenberger A (2005) Can we—and should we—have a Neuropsychiatry for Children and Adolescents? Eur Child Adolesc Psychiatry 14(8):466–470
Remschmidt H, Engeland HV (eds) (1999) Child and adolescent psychiatry in Europe: historical development, current situation, future perspectives. Springer, Darmstadt
Remschmidt H, Belfer M (2005) Mental health care for children and adolescents worldwide: a review. World Psychiatry 4(3):147–153
Rothenberger A (2001) The training logbook of UEMS section/board on child and adolescent psychiatry (CAPP) progress concerning European harmonization. Eur Child Adolesc Psychiatry 10(3):211–213
UEMS-CAP, Jacobs B (2014) European Training Logbook for Child and Adolescent Psychiatry (UEMS). http://www.uemscap.eu/uploads/45/UEMS_Logbook_final__-_12-01-2014_-_no_password-pdf. Accessed 1 Nov 2019
MindEd (2019) MindEd: A free educational resource on children and young people’s mental health. www.minded.org.uk. Accessed 1 Nov 2019
IACAPAP (2019) IACAPAP textbook of child and adolescent mental health. http://iacapap.org/iacapap-textbook-of-child-and-adolescent-mental-health. Accessed 1 Nov 2019
Mayer S et al (2014) European Psychiatric Association (EPA) guidance on post-graduate psychiatric training in Europe. Eur Psychiatry 29(2):101–106
Simmons M et al (2012) Trainee experiences of Child and Adolescent Psychiatry (CAP) training in Europe: 2010–2011 survey of the European Federation of Psychiatric Trainees (EFPT) CAP working group. Eur Child Adolesc Psychiatry 21(8):433–442
Tsiantis J, Piha J, Deboutte D (2007) UEMS child and adolescent psychiatry psychotherapy training guidelines. Int Psychiatry 2007(cited 41);24. www.uemscap.eu/uploads/13/Guidelines_on_Psychotherapy_2009-pdf. Accessed 4 Nov 2019
Roessner V et al (2011) European clinical guidelines for Tourette syndrome and other tic disorders. Part II: pharmacological treatment. Eur Child Adolescent Psychiatry 20(4):173–196 (Erratum appears in Eur Child Adolesc Psychiatry. 2011;20(7):377)
Taylor E et al (2004) European clinical guidelines for hyperkinetic disorder—first upgrade. Eur Child Adolesc Psychiatry 13(Suppl 1):I7–I30
Sollner W et al (2007) European guidelines for training in consultation-liaison psychiatry and psychosomatics: report of the EACLPP Workgroup on Training in Consultation-Liaison Psychiatry and Psychosomatics. J Psychosom Res 62(4):501–509
UEMS-CAP, Jacobs B (2014) Training requirements for the specialty of child and adolescent psychiatry. http://www.uemscap.eu/uploads/44/Training-Requirement-for-Child-adolescent-Psychiatry-approved_by_UEMS_Council_April_2014-pdf. Accessed 1 Nov 2019
Karabekiroglu K et al (2006) Child and adolescent psychiatry training in Europe: differences and challenges in harmonization. Eur Child Adolesc Psychiatry 15(8):467–475
Barrett EP et al (2011) P01–265—Child and adolescent psychiatry training in Europe: views of trainee representatives for 2009–2010 to the European federation of psychiatric trainees. Eur Psychiatry 26(Supplement 1):266
(2018) Accounts, C.o.P., Mental Health Services for Children and Young People, in House of Commons Committee of Public Accounts. House of Commons, UK Parliament. https://www.parliament.uk/business/committees/committees-a-z/commons-select/public-accounts-committee/inquiries/parliament-2017/inquiry12/. Accessed 4 Nov 2019
(2018) Psychiatry, E.S.f.C.a.A. ESCAP Member States. ESCAP member States. https://www.escap.eu/index/escap-members/. Accessed 2 Aug 2019
(2017) World Economic Outlook Database. International Monetary Fund
UEMS (2015) UEMS Statutes (revised). https://www.uems.eu/__data/assets/pdf_file/0003/25257/UEMS-2015-13-en-amend-04-15-STATUTES-UEMS.pdf. Accessed 4 Nov 2019
Hebebrand J et al (2019) EUREXIT? High time to consider the merits of European collaboration in child and adolescent psychiatry. Eur Child Adolesc Psychiatry 28(6):731–734
Brittlebank A et al (2016) Training in psychiatry throughout Europe. Eur Arch Clin Neurosci 266(2):155–164
Vizard T et al (2017) Mental health of children and young people in England. https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2017/2017. Accessed 4 Nov 2019
Ravens-Sieberer U et al (2007) Mental health of children and adolescents in Germany. Results from the BELLA study within the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 50(5–6): 871–878
Directive 2005/36/EC of The European Parliament and of the Council (2005) Official Journal of The European Union 39.9.2005 1.255/99, T.E.P.a. Council, Editor. 7th September 2005. p. 1.255/99
Kessler R et al (2005) Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry 62(6):593–602
Albayrak Ö et al (2012) Bibliometric assessment of publication output of child and adolescent psychiatric/psychological affiliations between 2005 and 2010 based on the databases PubMed and Scopus. Eur Child Adolesc Psychiatry 21:327–337
Jovanović N et al (2016) Burnout syndrome among psychiatric trainees in 22 countries: risk increased by long working hours, lack of supervision, and psychiatry not being first career choice. Eur Psychiatry 32:34–41
Hebebrand J (2017) ESCAP Research Academy. https://www.escap.eu/index/the-urgent-need-to-interact/. Accessed 2 Aug 2019
(2018) Trainees, E.F.o.P. http://www.sfbup.se/wp-content/uploads/2018/11/Guidelines-of-the-EFPT-Exchange-Programme.pdf. Accessed 4 Nov 2019
Hodges B (2019) Assessment of competence of trainees in psychiatry. Department of Psychiatry and the Wilson Centre for Research in Education
Jovanović N et al (2019) Depression and suicidality among psychiatric residents—results from a multi-country study. J Affect Disord 249:192–198
Acknowledgements
The following contributed country data: Annemie Baelemans, Salma Baidusi Natoor, Stepanka Beranova, Ariel Como, Saliha Kılınç, Jasna Klara Lipovšek, Viktorija Palubeckiene, Sara Emilie Poulsen, Natalia Sergeeva.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
This article is part of the focused issue ‘The European and Global Perspective on Training in Child and Adolescent Psychiatry’.
Henrikje Klasen: Sadly Dr. Rikje Klasen who was deeply involved in the design and implementation of this paper died part way through the preparation. She is greatly missed.
Henrikje Klasen: Deceased.
The original version of this article was revised due to incorrect thirteenth name of the author.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Barrett, E., Jacobs, B., Klasen, H. et al. The child and adolescent psychiatry: study of training in Europe (CAP-STATE). Eur Child Adolesc Psychiatry 29, 11–27 (2020). https://doi.org/10.1007/s00787-019-01416-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-019-01416-3