
Abstract
Objectives
The aim of this in vitro study was to assess the dentinal tubule penetration of three different sealers, AH Plus, BC Sealer and a novel tricalcium silicate sealer (NTS).
Materials and methods
Ninety-six human maxillary central incisors were divided into three experimental groups (n = 32) and were filled with gutta-percha using a single-cone technique in conjunction with one of the three sealers: AH Plus, BC Sealer or NTS. The roots in each group were cross-sectioned at 1 and 5 mm from the root apex, and the surfaces were examined under confocal laser scanning microscopy (CLSM). The sealer penetration depths were measured at their maximum depths and at four circumferential depths (12, 3, 6 and 9 o’clock) and were evaluated using ImageJ software (ImageJ, NIH).
Results
The maximum and mean penetration depths were significantly higher at 5 mm compared to 1 mm from the apex in the AH Plus (p < 0.001), BC Sealer (p < 0.001) and NTS groups (p < 0.001). No significant difference was observed between the groups at 1 mm for both parameters. The maximum and mean penetration depths were significantly lower at 5 mm for AH Plus compared with the other two groups (p = 0.012).
Conclusions
Within the study limitations, the BC Sealer and NTS demonstrated better tubule penetration results than the AH Plus sealer.
Clinical relevance
Although no study has confirmed a relationship between the penetration depth of root canal sealers and the prevention of apical periodontitis, dentinal tubule sealer penetration may improve obturation quality.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The aim of a root canal filling is to prevent reinfection of the disinfected canal. This is achieved primarily by providing an adequate seal against any possible bacterial ingress and their related toxins using gutta-percha (GP) in combination with root canal sealers [1, 2]. Root canal sealers are used to fill the space between the gutta-percha cones and the dentinal wall. Different root canal sealers have been used in endodontic therapy. AH Plus (Dentsply DeTrey, Konstanz, Germany), a widely used epoxy resin–based sealer, possesses positive manipulation characteristics and high physical properties [3]. It has been tested and is considered the gold standard for use as a control material in most studies on sealers [4,5,6,7,8]. Newly developed calcium silicate-based sealers are reportedly comparable to resin-based sealers, such as AH Plus, in terms of sealing ability [9]. These sealers generate bioactivity on the material surface. In addition, calcium silicate-based sealers demonstrate low cytotoxicity and high biocompatibility, and they can induce an osteogenic response [10]. EndoSequence BC Sealer (Brasseler USA, Savannah, GA, USA), a calcium silicate-based sealer, is a single-component sealer that is cytocompatible [11] and sets in vivo when water diffuses into the sealer. Its penetration into the dentinal tubules forms a physical barrier, improves retention of the root filling and entombs residual bacteria [12, 13]. The farther a sealer can penetrate into the tubules, the greater its antibacterial effect, if present, is [14]. Physical and chemical properties, such as wettability and flow ability, are important parameters that may have an impact on a sealer’s dentin tubule penetration depth [6]. A new experimental novel tricalcium silicate (NTS)-based sealer composed of tricalcium silicate, tantalum and calcium oxide has been recently developed [15]. It is considered to be minimally cytotoxic [16]. NTS is composed of tricalcium silicate, which also includes calcium carbonate in the formulation. The calcium carbonate is added as a filler and acts as a nucleating agent, providing more reaction sites for cement hydration [15]. Among a variety of obturation techniques, the single-cone obturation technique is generally recommended with calcium silicate-based sealers for several reasons. In fact, calcium silicate-based sealers do not shrink compared with other types of sealers [17]; the application of heat may affect their properties [18], and finally, they have been claimed to create bonds along the sealer/gutta-percha interface [19]. Although a number of tricalcium silicate-based sealers have been recently developed, none fulfils the necessary criteria of stability and interaction with dentin, and to the best of our knowledge, no study to date has compared the tubule penetration of these three different sealers.
The purpose of this study was to investigate tubule penetration of AH Plus, BC Sealer and NTS under CLSM. The null hypothesis tested was that there were no significant differences in the maximum depth penetration or in the mean depths of sealer penetration among the three experimental groups.
Materials and methods
A total of 96 extracted human maxillary central incisors with fully formed apices were anonymously collected from several dental offices and stored in distilled water. Teeth were obtained from patients varying in age from 50 to 60 years old. The study was approved by the ethics committee of Saint Joseph University, Beirut, Lebanon (USJ-2016-61). Digital periapical radiographs (SOPIX2, Acteon, France) were taken from the mesiodistal and buccolingual directions to confirm the presence of a single canal. The crowns of the teeth were removed, and the root was cut to a 16-mm length. A standard access preparation was performed for each tooth. The working length was established with a no.10 K-file (Dentsply Maillefer, Ballaigues, Switzerland). The file was introduced into the canal until it was visible at the apical foramen, and its length was measured. The working length (WL) was determined by subtracting 0.5 mm from this length. Root canals were instrumented to a size no. 15 K file (Dentsply Maillefer), followed by ProTaper (Dentsply Maillefer, Ballaigues, Switzerland) rotary instrumentation to a size of F4 (40/06). The hand piece was used with an electric engine (X-smart, Densply Maillefer, Ballaigues, Switzerland) at 250 rpm.
During instrumentation, the root canals were copiously irrigated with 10 mL 5.25% NaOCl. After instrumentation, the canals were irrigated with 10 mL 17% EDTA, followed by 3 mL 5.25% NaOCl for 3 min and then a final flush with 10 mL deionised water. All root canals were irrigated using 30-gauge irrigation needles (Max-I-Probe; Dentsply Maillefer) and dried with paper points. The specimens were randomly distributed into the following three groups, according to the sealer type: group AH Plus (n = 32), group BC Sealer (n = 32) and group NTS (n = 32).
Root canal obturation
Each sealer was prepared according to each manufacturer’s directions. To perform analysis under CLSM, the sealers were labelled with rhodamine B (Sigma-Aldrich, St. Louis, MO, USA) to an approximate concentration of 0.1% to provide fluorescence and allow confocal laser microscopy assessment. The single cone technique was used for obturation. All root canal sealers were placed into the canal 1-mm short of the working length, using a size 30 Lentulo spiral (Dentsply Maillefer, Ballaigues, Switzerland). The Lentulo was used in small pecking motions within the canal for at least 5 s. A single gutta-percha cone (ProTaper Universal F4, Dentsply Maillefer) was then lightly coated with the sealer and placed in the root canal to the WL. The cone was cut at the level of the orifice and slightly condensed with a plugger. The coronal opening was filled with a temporary filling material (Cavit, 3 M; ESPE, St. Paul, MN), and the specimens were stored at 100% humidity and 37 °C for 2 weeks to completely set.
Root sectioning and root surface preparation
After 2 weeks, the teeth were inserted centrally and vertically in orthodontic resin (Dentsply Caulk, Milford, DE, USA). The samples were stored in a humidity chamber at room temperature until the end of the study (6–7 weeks). The root canals were cross-sectioned perpendicular to their long axes using a diamond disk (Buehler, Lake Bluff, IL, USA) with a slow speed (25,000 rpm) hand-piece 1 mm and 5 mm from the root apex. The specimens were then mounted onto glass slides, and the coronal surface were polished using sand papers number 500, 700 and 1200 under continuous water to eliminate the debris product coming from the cutting procedure. The sample thickness submitted to confocal laser microscopy was 2 mm.
Confocal laser scanning microscopy analysis of the roots
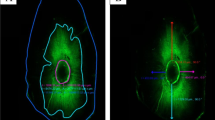
Specimens were examined with a Zeiss confocal laser scanning microscope (Zeiss, LSM 780, Germany) at × 5 magnification with a wavelength of 514 nm. Digital images were imported into the ImageJ software program (ImageJ, NIH) to determine the total dentinal tubule penetration area. The sealer penetration depths into the dentinal tubules were evaluated for each specimen at the maximum depth using the method described by Bolles et al. [20]: the deepest penetration was measured from the canal wall to the point of maximum sealer penetration using the measuring tool in ImageJ. Each measurement was performed twice to ensure consistency and reproducibility. Furthermore, the mean sealer penetration depths were measured by averaging the penetration depths at four circumferential points (12, 3, 6 and 9 o’clock) [21] corresponding to the buccal, mesial, lingual and distal directions, respectively [22]. While analysing images, we used a superimposed grid to standardise the four directions (12, 3, 6 and 9 o’clock). The penetration depth was then measured twice in each direction using the measuring tool in Image J. The sealer penetration depths were calculated for each direction and averaged, yielding the mean penetration depth values (Figs. 1, 2, and 3).

The sealer penetration depth (AH Plus) at 1 mm (left) and 5 mm (right) from the apex

The sealer penetration depth (BC Sealer) at 1 mm (left) and 5 mm (right) from the apex

The sealer penetration depth (NTS) at 1 mm (left) and 5 mm (right) from the apex
Statistical analysis
The statistical software SPSS for Windows (Version 22.0, Chicago, IL, USA) was used for statistical analysis of the data. The level of significance was set at 0.05. The normality distribution of continuous variables was assessed with Kolmogorov-Smirnov tests.
The maximum depth penetration and mean penetration depth of the sealer into the dentinal tubules were compared between the three types of cement (NTS, AH Plus, BC Sealer) at 1 and 5 mm from the apex. Two-way analysis of variance was conducted, followed by univariate analyses and multiple comparisons tests of Tukey (HSD).
Results
Maximum depth penetration of sealer in dentinal tubules
The maximum depth penetration was not significantly different between the three types of cement at 1 mm from the apex (p = 0.692). At 5 mm, there was a significant difference between the three groups. The sealer depth penetration at 5 mm was significantly lower for AH Plus, followed by NTS, and it was higher for BC Sealer (p = 0.012) (Table 1).
The maximum depth penetration was significantly higher at 5 mm from the apex compared to the 1 mm level for the AH Plus (p < 0.001), BC Sealer (p < 0.001) and NTS groups (p < 0.001) (Table 1).
Mean penetration depth of the sealer in dentinal tubules
The mean depth penetration was not significantly different between the three groups at 1 mm from the apex (p = 0.496). At the 5-mm level, the mean penetration depth was significantly smallest for the AH Plus sealer (p = 0.033), and the difference was not significant between BC Sealer and NTS (p > 0.05) (Table 2).
The mean penetration depth was significantly higher at the 5-mm level compared to the 1-mm level for AH Plus (p < 0.001), BC Sealer (p < 0.001) and NTS (p < 0.001) (Table 2).
Discussion
The aim of this in vitro study was to assess the dentinal tubule penetration of three different sealers, AH Plus, BC Sealer and NTS, in terms of the penetration depth into dentinal tubules under CLSM.
In the current study, the sealer penetration depth was evaluated under confocal microscopy. Different microscopic techniques, such as light microscopy, scanning electron microscopy (SEM) and CLSM have been used to show root canal sealers within dentinal tubules. In the present study, CLSM was used instead of SEM because it allows the detection of sealer penetration along the canal circumference of each sample using fluorescence. With CLSM, the formation of high contrast points shows the sealer penetration within the dentinal tubules. Another advantage when using CLSM in segments is that the sealer can be visualised at various depths. It offers several advantages over conventional wide-field optical microscopy and SEM [23,24,25], including the ability to control the depth of field, reduction of background information away from the focal plane and the ability to assemble many optical sections, even from thick specimens. Picoh et al. [26] have reported that when using CLSM, artefacts can be practically excluded. When using CLSM, the sealer must be labelled with a fluorescent dye for evaluation. Rhodamine B (Sigma-Aldrich, St Louis, MO, USA) has been used as an indicator under CLSM because it allows for the identification of sealers within the dentinal tubules [27] and does not affect the physical properties of the sealers, as long as a small amount of dye (less than 0.2%) is mixed with the sealers [28].
In the current study, for the three groups, both the mean and maximum penetration depths were higher at the 5-mm level compared to the 1-mm level, in accordance with results from Camilleri [18], who found that AH Plus completely penetrated the dentinal tubules in the coronal and mid-root portions, while in the apical region, penetration was not always observed. These findings are also similar to those reported by McMichael et al. [29], who found that the BC Sealer penetration depth was significantly higher at 5 mm from the apex compared to the 1-mm level. One explanation may be that the number and diameter of dentinal tubules decrease apically in the root canal. Furthermore, some areas in the apical third are dentinal tubule free, and tissue-like cementum can contour the apical root canal wall, obstructing tubules [30]. Another explanation may be the better removal of the smear layer in the coronal region.
This study demonstrated that the maximum and the mean depth penetrations were significantly lower with AH Plus at 5 mm from the apex compared with NTS and BC Sealer. These results show that a calcium silicate-based sealer can penetrate dentinal tubules without applying intra-canal compaction pressure, which is usually used in gutta-percha filling techniques. This finding would be clinically significant because it would remove the necessity to use excessive force during obturation techniques, which could lead to the generation of root canal cracks or fractures. Compaction is not used in the single-cone technique, but this technique may result in voids in irregular canals [31, 32]. Celikten et al. found that at all levels, void volumes were the highest for the SC technique with the tested bioceramic sealer [33]. Persisting gaps allow for leakage and bacterial contamination, contributing to the failure of endodontic therapy. In the current study, the small particle size of BC Sealer may explain why it penetrated the deepest at this level (5 mm). McMichael et al. [29] have shown that BC Sealer penetrated tubules as deep as 2 mm when a single cone technique was applied. Jeong et al. [21] have also shown that penetration of a tricalcium silicate sealer into the dentinal tubules occurred independently of the obturation technique, a finding that is in accordance with our study, in which NTS penetrated tubules as deeply as 2000 μm (2 mm). Other studies comparing the sealer penetration depths of AH Plus, BC Sealer and MTA Fillapex have reported penetration depths varying from 23.4 to 84.3 μm [34, 35]. These shorter depths in dentinal tubules were attributed to the limitation of scanning electron microscopy (SEM), which only allows the specimen surfaces to be viewed. According to Mamootil et al. [13], physical and chemical properties, such as particle size, solubility, viscosity and surface tension, influence the depth and consistency of the material’s dentinal tubule penetration. However, this study included only maxillary central incisors, in order to control the confounding factors and eliminate the effect of root canal anatomy on sealer penetration into dentinal tubules. Further study should be performed on different root canal anatomy to confirm the results obtained.
Sealer penetration in dentinal tubules has the benefit of improving the mechanical retention of sealer to the dentinal walls [12, 36]. It may operate as a blocking agent, which could inactivate bacteria or prevent their repopulation inside tubules. It can also form a physical barrier to prevent bacterial microleakage and recontamination of the root canal system [12]. Additionally, sealers that penetrated into dentinal tubules can maintain their bactericidal action [37, 38], which is favourable for healing periapical lesions and preventing reinfection. This study did not examine the interface between the gutta-percha and dentin wall. Indeed, the incidence of voids in root canal filling material can result in the proliferation of residual microorganisms and may jeopardise the treatment outcome. Further studies are necessary to analyse the interfacial adaptation of these sealers to root canal walls.
Conclusions
Within the limits of this study, it can be postulated that BC Sealer and NTS demonstrated better dentinal tubule penetration results compared to AH Plus.
References
Michaud RA, Burgess J, Barfield RD, Cakir D, McNeal SF, Eleazer PD (2008) Volumetric expansion of gutta-percha in contact with eugenol. J Endod 34:1528–1532. https://doi.org/10.1016/j.joen.2008.08.025
Li GH, Niu LN, Zhang W, Olsen M, De-Deus G, Eid AA, Chen JH, Pashley DH, Tay FR (2014) Ability of new obturation materials to improve the seal of the root canal system: a review. Acta Biomater 10:1050–1063. https://doi.org/10.1016/j.actbio.2013.11.015
Duarte MAH, Ordinola-Zapata R, Bernardes RA, Bramante CM, Bernardineli N, Garcia RB, de Moraes IG (2010) Influence of calcium hydroxide association on the physical properties of AH Plus. J Endod 36:1048–1051. https://doi.org/10.1016/j.joen.2010.02.007
Gharib SR, Tordik PA, Imamura GM, Baginski TA, Goodell GG (2007) A confocal laser scanning microscope investigation of the epiphany obturation system. J Endod 33:957–961. https://doi.org/10.1016/j.joen.2007.03.011
Patel DV, Sherriff M, Ford TRP, Watson TF, Mannocci F (2007) The penetration of RealSeal primer and TubliSeal into root canal dentinal tubules: a confocal microscopic study. Int Endod J 40:67–71. https://doi.org/10.1111/j.1365-2591.2006.01184.x
Marciano MA, Guimarães BM, Ordinola-Zapata R, Bramante CM, Cavenago BC, Garcia RB, Bernardineli N, Andrade FB, Moraes IG, Duarte MA (2011) Physical properties and interfacial adaptation of three epoxy resin-based sealers. J Endod 37:1417–1421. https://doi.org/10.1016/j.joen.2011.06.023
Marin-Bauza GA, Rached-Junior FJA, Souza-Gabriel AE, Sousa-Neto MD, Miranda CES, Silva-Sousa YTC (2010) Physicochemical properties of methacrylate resin-based root canal sealers. J Endod 36:1531–1536. https://doi.org/10.1016/j.joen.2010.05.002
Jardine AP, Da Rosa RA, Santini MF, Wagner M, Só MV, Kuga MC, Pereira JR, Kopper PM, Só MVR (2016) The effect of final irrigation on the penetrability of an epoxy resin-based sealer into dentinal tubules: a confocal microscopy study. Clin Oral Invest 20:117–123. https://doi.org/10.1007/s00784-015-1474-8
Ersahan S, Aydin C (2013) Solubility and apical sealing characteristics of a new calcium silicate-based root canal sealer in comparison to calcium hydroxide-, methacrylate resin- and epoxy resin-based sealers. Acta Odontol Scand 71:857–862. https://doi.org/10.3109/00016357.2012.734410
Chang SW, Lee SY, Kang SK, Kum KY, Kim EC (2014) In vitro biocompatibility, inflammatory response, and osteogenic potential of 4 root canal sealers: Sealapex, Sankin apatite root sealer, MTA Fillapex, and iRoot SP root canal sealer. J Endod 40:1642–1648. https://doi.org/10.1016/j.joen.2014.04.006
da Silva EJNL, Zaia AA, Peters OA (2017) Cytocompatibility of calcium silicate-based sealers in a three-dimensional cell culture model. Clin Oral Invest 21:1531–1536. https://doi.org/10.1007/s00784-016-1918-9
Kokkas AB, Boutsioukis AC, Vassiliadis LP, Stavrianos CK (2004) The influence of the smear layer on dentinal tubule penetration depth by three different root canal sealers: an in vitro study. J Endod 30:100–102. https://doi.org/10.1097/00004770-200402000-00009
Mamootil K, Messer HH (2007) Penetration of dentinal tubules by endodontic sealer cements in extracted teeth and in vivo. Int Endod J 40:873–881. https://doi.org/10.1111/j.1365-2591.2007.01307.x
Wang Z, Shen Y, Haapasalo M (2014) Dentin extends the antibacterial effect of endodontic sealers against enterococcus faecalis biofilms. J Endod 40:505–508. https://doi.org/10.1016/j.joen.2013.10.042
Khalil I, Naaman A, Camilleri J (2016) Properties of tricalcium silicate sealers. J Endod 42:1529–1535. https://doi.org/10.1016/j.joen.2016.06.002
Chakar S, Changotade S, Osta N, Khalil I (2017) Cytotoxic evaluation of a new ceramic-based root canal sealer on human fibroblasts. Eur J Dent 11:141–148. https://doi.org/10.4103/ejd.ejd_2_17
Candeiro GT, Correia FC, Duarte MA, Ribeiro-Siqueira DC, Gavini G (2012) Evaluation of radiopacity, pH, release of calcium ions, and flow of a bioceramic root canal sealer. J Endod 38:842–845. https://doi.org/10.1016/j.joen.2012.02.029 Epub 2012 Apr 4
Camilleri J (2015) Sealers and warm gutta-percha obturation techniques. J Endod 41:72–78. https://doi.org/10.1016/j.joen.2014.06.007
Gillespie WT, Loushine RJ, Weller RN, Mazzoni A, Doyle MD, Waller JL, Pashley DH, Tay FR (2006) Improving the performance of EndoREZ root canal sealer with a dual-cured two-step self-etch adhesiveIIApical and coronal seal. J Endod 32:771–775 Epub 2006 Apr 4
Bolles JA, He J, Svoboda KK, Schneiderman E, Glickman GN (2013) Comparison of Vibringe, EndoActivator, and needle irrigation on sealer penetration in extracted human teeth. J Endod 39(5):708–711
Jeong JW, DeGraft-Johnson A, Dorn SO, Di Fiore PM (2017) Dentinal tubule penetration of a calcium silicate-based root canal sealer with different obturation methods. J Endod 43:633–637. https://doi.org/10.1016/j.joen.2016.11.023
Russell A, Friedlander L, Chandler N (2017) Sealer penetration and adaptation in root canals with the butterfly effect. Aust Endod J. https://doi.org/10.1111/aej.12238
Tedesco M, Chain MC, Bortoluzzi EA, da Fonseca Roberti Garcia LDFR, Alves AMH, Teixeira CS (2018) Comparison of two observational methods, scanning electron and confocal laser scanning microscopies, in the adhesive interface analysis of endodontic sealers to root dentine. Clin Oral Invest:1–9. https://doi.org/10.1007/s00784-018-2336-y
Chandra SS, Shankar P, Indira R (2012) Depth of penetration of four resin sealers into radicular dentinal tubules: a confocal microscopic study. J Endod 38:1412–1416. https://doi.org/10.1016/j.joen.2012.05.017
Amos WB, White JG (2003) How the confocal laser scanning microscope entered biological research. Biol Cell 95:335–342. https://doi.org/10.1016/s0248-4900(03)00078-9
Pioch T, Stotz S, Buff E, Duschner H, Staehle HJ (1998) Influence of different etching times on hybrid layer formation and tensile bond strength. Am J Dent 11:202–206
Al-Haddad A, Abu Kasim NH, Che Ab Aziz ZA (2015) Interfacial adaptation and thickness of bioceramic-based root canal sealers. Dent Mater J 34:516–521. https://doi.org/10.4012/dmj.2015-049
Thota MM, Sudha K, Malini DL, Madhavi SB (2017) Effect of different irrigating solutions on depth of penetration of sealer into dentinal tubules: a confocal microscopic study. Contemp Clin Dent 8:391–394. https://doi.org/10.4103/ccd.ccd_114_17
McMichael GE, Primus CM, Opperman LA (2016) Dentinal tubule penetration of tricalcium silicate sealers. J Endod 42:632–636. https://doi.org/10.1016/j.joen.2015.12.012
Mjör IA, Smith MR, Ferrari M, Mannocci F (2001) The structure of dentine in the apical region of human teeth. Int Endod J 34:346–353. https://doi.org/10.1046/j.1365-2591.2001.00393.x
Weis MV, Parashos P, Messer HH (2004) Effect of obturation technique on sealer cement thickness and dentinal tubule penetration. Int Endod J 37:653–663
Bergmans L, Moisiadis P, De Munck J, Van Meerbeek B, Lambrechts P (2005) Effect of polymerization shrinkage on the sealing capacity of resin fillers for endodontic use. J Adhes Dent 7:321–329
Celikten B, Uzuntas CF, Orhan AI, Tufenkci P, Misirli M, Demiralp KO, Orhan K (2015) Micro-CT assessment of the sealing ability of three root canal filling techniques. J Oral Sci 57:361–366. https://doi.org/10.2334/josnusd.57.361
Balguerie E, van der Sluis L, Vallaeys K, Gurgel-Georgelin M, Diemer F (2011) Sealer penetration and adaptation in the dentinal tubules: a scanning electron microscopic study. J Endod 37:1576–1579. https://doi.org/10.1016/j.joen.2011.07.005
Shokouhinejad N, Sabeti M, Gorjestani H, Saghiri MA, Lotfi M, Hoseini A (2011) Penetration of epiphany, epiphany self-etch, and AH Plus into dentinal tubules: a scanning electron microscopy study. J Endod 37:1316–1319. https://doi.org/10.1016/j.joen.2011.05.002
Ordinola-Zapata R, Bramante CM, Graeff MS, del Carpio Perochena A, Vivan RR, Camargo EJ, Garcia RB, Bernardineli N, Gutmann JL, de Moraes IG (2009) Depth and percentage of penetration of endodontic sealers into dentinal tubules after root canal obturation using a lateral compaction technique: a confocal laser scanning microscopy study. Oral Surg Oral Med Oral Pathol Oral Rad Endod 108:450–457. https://doi.org/10.1016/j.tripleo.2009.04.024
Branstetter JVFJ, Von Fraunhofer JA (1982) The physical properties and sealing action of endodontic sealer cements: a review of the literature. J Endod 8:312–316. https://doi.org/10.1016/S0099-2399(82)80280-X
Heling I, Chandler NP (1996) The antimicrobial effect within dentinal tubules of four root canal sealers. J Endod 22:257–259. https://doi.org/10.1016/S0099-2399(06)80144-5
Funding
This work was supported by the Medical Research Council of Saint-Joseph University (grant number: FMD136 – CRENDU01/November/2016).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study does not contain any research involving human participants or animals.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
El Hachem, R., Khalil, I., Le Brun, G. et al. Dentinal tubule penetration of AH Plus, BC Sealer and a novel tricalcium silicate sealer: a confocal laser scanning microscopy study. Clin Oral Invest 23, 1871–1876 (2019). https://doi.org/10.1007/s00784-018-2632-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-018-2632-6