
Abstract
Objectives
A selective intensified prevention (SIP) was introduced at individual schools in deprived areas in Marburg County (Germany) in 1995. The outcome of the program was evaluated in sixth graders (mean age: 12.06 years) in comparison to a control region.
Materials and methods
Caries experience was recorded by applying International Caries Detection and Assessment System (ICDAS) II criteria. Tooth brushing habits and other independent variables were examined psychometrically. To compare the mean caries scores, non parametric tests were applied. The influence of various independent variables on caries experience was assessed by stepwise backward logistic regression analysis. The matching criteria age, gender, ethnicity and maternal education were used to parallelize the samples.
Results
ICDAS scores of 2–6 were detected uniformly more often in the control region than in the test group. Combining ICDAS scores 3–6, children from the control region (mean D3–6MFT: 1.73) showed roughly double the caries experience compared to the test group (mean D3–6MFT: 0.88, p < 0.005). The D5,6MFT score of the test group amounted to 0.50, and the corresponding value of the reference group was 0.77 (p = 0.043). Multivariate analysis disclosed fissure sealants, early start of tooth brushing and topical fluoride application to be associated with the prevention of dental caries. High frequency of sugar intake was associated with the presence of dentine lesions.
Conclusions
The results of our study confirm the positive effect of SIP on the dental health of 12-year-old pupils living in deprived areas.
Clinical relevance
On the basis of ICDAS II, targeted preventive measures can be applied in children with increased caries risk. Frequent applications of fluoride varnish inhibit the progression of initial lesions in this group.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the mid 1980s, the caries prevalence among children and young people in the Federal Republic of Germany was quite high [1]. Beginning in 1989, it became possible to intensify preventive care for school children because changes in the public health insurance system gradually improved the general conditions for preventive dentistry in Germany. From this time on, public health insurance companies were obliged to pay both for preventive action taken in schools (for 6- to 12-year- olds) as well as for individual prevention (for 12- to 18-year-olds). In 1993, individual prevention was extended to include children 6–11 years of age. In addition, preventive sealing of fissures on molars was also incorporated into the range of services covered by statutory health insurance. In Marburg County, the regular application of fluoride varnish was introduced at the beginning of the 1980s to Marburg schools. The success of this concept has been already evaluated [2, 3].
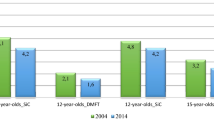
The systematic evaluation of group prevention within the scope of "national surveys" also showed that dental health of 12-year-olds, in particular, improved considerably between 1994 and 2004 [4].
Despite the observed caries decline, caries experience is still often found to be polarized. This "polarization" of caries experience has rather intensified in the course of recent decades [5] and is due to the fact that the social class a family belongs to strongly determines how it makes use of preventive and curative measures [6]. Many studies show a correlation between enhanced caries risk and socioeconomic deprivation [7]. That is why the clause concerning group prevention was amended in 1993 with the goal of having prevention providers introduce intensive prevention for children with increased caries risk. Hence deficits in the family were to be compensated by "selective intensive prevention" (SIP) in kindergartens and schools. Comprehensive prevention based on fluoride varnish applications has proven to be an effective method [8, 9]. In Marburg County, SIP is offered at individual schools in underprivileged districts comprising the following measures:
-
Enhanced health education
-
Oral hygiene instructions four times per year
-
Fluoride varnish applications four times per year
Traditionally, caries is recorded at cavitation level in public dental health programs in schools. This is standard practice in the WHO recommendations for caries diagnosis [10]. Non-cavitated lesions are often not taken into consideration. But having the latter information may help to design targeted prevention programs to prevent the progression of initial carious lesions [11]. In order to investigate correlations between specific parameters and dental caries in a population, it is useful to record incipient lesions (D1, 2) and dentine caries (D3) as well. Certain connections between the outcome variables for caries and the independent variables can only be shown on the basis of D1, 2 [3]. A suitable method is the International Caries Detection and Assessment System (ICDAS) II [12], which has already been validated [13] and is being used in clinical studies [14–16].
Building on experience with basic prevention founded on the application of fluoride varnish twice a year [2, 3], supplementary intensive prevention measures began to be introduced to schools in deprived areas of some regions in Germany. Since there are at present no studies of the efficacy of this SIP, the aim of this study was to evaluate the effect of SIP in sixth graders in comparison to a control region without SIP using the ICDAS II criteria.
Subjects and methods
Study areas and population
The study was approved by the Committee for Ethics of the medical faculty, University of Marburg, Germany (file number: Studie 200/06, chairman: Prof. G. Richter). The subjects in the study group (living in Marburg-Biedenkopf County in the German State of Hesse) were compared to a control group (recruited in Osnabrück County in the German State of Lower Saxony) which is a demographically similar region. In the study region, all schools being involved in the intensified prevention were participating in the study. For the control group, children were recruited from schools in socially deprived areas without intensive prevention measures. The fluoride concentration in the tap water of both regions had been constant for many years and did not exceed 0.25 mg F/l.
The examinations were performed between November 2007 and June 2008. A total of 19 schools were investigated in both regions. The examination was focusing on sixth-grade children. The dental examinations were supplemented by collecting data on the parents. All pupils willing to participate had been registered by their parents and informed consent was given. Mentally or physically disabled adolescents were not included in the study.
The gross sample covered 1,403 sixth graders and a total of 925 pupils took part in the study (65.9 % response rate). A total of 236 pupils came from the study region (76.1 % response rate) and 689 from the control region (63 % response rate). The mean age of all participants amounted to 12 (±0.6) years.
Organization of the study and dental examination
The examinations in the schools were performed by one examiner (K.W.), who had been calibrated by an experienced epidemiologist (K.P.) combining theoretical information, preliminary diagnostic training with slides and examination of patients. The diagnoses were checked against those recorded by the reference examiner. The inter-examiner reliability (kappa) showed a value of 0.74, the intra-examiner reliability a value of 0.86.
The examinations took place either in a classroom or in the first aid room. Before, supervised toothbrushing was performed by each participant as ICDAS can only be applied in clean teeth. Single sites of teeth which had not been cleaned thoroughly by the children themselves were cleansed of dental plaque by the examiner. The dental status of each child was surveyed using an examination table, along with a halogen lamp, bottled compressed air which for drying the teeth, plane mirrors and CPI probes. The extent of tooth surface restoration (from untreated to missing) was registered first, then the stage of the caries was assessed using the ICDAS II criteria [17]. Due to legal restrictions, no radiographs could be taken; instead, Fiber Optic Transillumination (FOTI) was applied. The presence of sealants was determined, without identifying whether they were complete or not.
Ascertaining the exposure to preventive measures
Documentation from dental public health service of the children in the study group was used to investigate which preventive measures had been applied to the individual child during the years at school. The frequency of oral hygiene instructions, dietary counseling and fluoride varnish applications was recorded.
In the control group, no school-based preventive measures with topical fluoride application were offered.
Specific aspects and characteristics of children's exposure to preventive measures were ascertained by having the parents fill in questionnaires prior to the dental examinations. With this, demographic information such as age, gender, marital status, education, occupational status or ethnic origin (language used in the family as stated by the parents) were assessed. In order to minimize absences due to insufficient language skills among families with an immigrant background, alternative letters and questionnaires for parents were available in Turkish, Russian, Kurdish (two versions) and Arabic, of which practically only the first two were used, and then in small numbers.
The following variables were surveyed with the parent's questionnaire: (a) Topical fluoridation at the dental office (don't know/no/yes) and if so, how many times; since school enrollment (b) use of fluoride supplements at home in the past (don't know/no/yes) and if so, for how long; (c) use of fluoridated salt at home (don't know/no/yes) and if so, since when; (d) age at which the child began practicing dental hygiene (before the first year of life/after the first year of life.
The social status of the families was categorized by the level of education and the occupational status. If the data from the mother and the father differed, the highest value of both was used. As we were not able to collect data concerning family income, the transliterated occupational status got a double weight and was added to the transliterated level of education [18]. The resulting index exhibited values between 3 and 23. Social status index values from 3 to 14 were assessed as low, from 15 to 19 as average and from 20 to 23 as high social status.
Information on nutrition was recorded using a children's questionnaire. In addition, the children's questionnaire asked which foodstuffs were eaten or drunk in six specific everyday situations. The questions included (a) a description of the situation and (b) a selection of various foods typical of the situation. A list was made of healthy (harmless to teeth) and cariogenic foods. The frequency of consumption was indicated using answer scales graduated in fives (never, seldom, occasionally, often, always) which were given point values from 0 to 4. The individual points were added together to yield the sugar index.
Data collection and statistical analysis
The on-site findings were registered on a documentation form noting type of school, gender and the date of examination of the child. After finalizing the dental examination, the form for the findings, the questionnaires, and the blank for preventive measures applied at school were collated. After entering the data into an Excel database the statistical analysis was performed using SPSS, Version 17.0.
The samples were parallelized by composing matched pairs with children from the control region. The following matching criteria were used: gender, age, mother’s education, and ethnic origin. “Statistical twins” were found in the reference group for 89.0 % of the test group. Thus each group consisted of 210 children (total n = 420, 49.0 % girls and 51.0 % boys).
The outcome variables surveyed provided the basis for calculating the following indices: D3–6MFT (including ICDAS codes 3–6), D5,6MFT, D1,2F-S and D3-6F-S.
Mann–Whitney U-tests were used to test the significance of the differences between averages. The significance level was set at α = 0.05.
To examine the extent of influence of various independent variables on the dependent variable D3–6MFT, a "stepwise backward logistic regression analysis" was undertaken. All variables surveyed with the questionnaire and fissure sealings were included in the evaluation. The dependent variable was dichotomized (D3–6MFT = 0 or >0).
Results
Dental examinations
The analysis was performed with the data for the parallelized groups in order to be able to compare the two regions independently of confounding factors. It became apparent that ICDAS scores of 2–6 were detected uniformly more often in the control region than in the test group (Fig. 1). The difference was significant for every code. The proportion of filled tooth surfaces was also significantly higher in the control region. However, the ICDAS code 1 was found more frequently in the test group than in the control group.

Mean values of ICDAS codes and FS of the test (MR) and control region (OS)
The mean caries scores are shown in Fig. 2. The average values were significantly lower in the test region than in the control group, except for the level of initial lesions (D1,2-S). If we include ICDAS scores 3–6 in the calculation of the D component, the difference between the two groups becomes clearest. Then the children from the control region exhibit roughly twice as much caries (D3–6MFT = 1.73, D3–6FS = 1.94) as the children from the test region (D3–6MFT = 0.88, D3–6FS = 0.95).

Mean caries scores in the test (MR) and control region (OS). D1–6T mean number of teeth with ICDAS scores 1, 2, 3, 4, 5 or 6; D3–6T mean number of teeth with ICDAS scores 3, 4, 5 or 6; D5,6T mean number of teeth with ICDAS scores 5 or 6; D3–6S mean number of tooth surfaces with ICDAS scores 3, 4, 5 or 6; D1,2S mean number of surfaces with ICDAS scores 1 or 2; MT mean number of missing teeth due to caries; FT mean number of filled teeth
A D3–6MFT index of 0 was found among 60.0 % of sixth graders in Marburg and 45.2 % of those in Osnabrück. The largest observed D3–6MFT score was 12 (Fig. 3).

Frequency distribution of the D3–6MFT in the test (MR) and control region (OS)
The group of sixth graders in the test group had an average of 2.68 fissure sealants. In the control group, the average amounted to 2.20 teeth with sealants.
Evaluation of the questionnaires
As far as oral hygiene is concerned, 61.0 % of the parents in the test group and 53.3 % of the parents in the control group indicated that they had started brushing their child's teeth in the first year of life (p = 0.004). In the second year of life, 18.6 % (test group) and 17.6 % (control group) had begun. In the test region, 19.6 % of the children had begun to brush their teeth in the third year of life or later. In the control group, this was 26.1 %.
There were no significant differences between the families in the test and control regions in the use of fluoridated table salt (53.8 % vs. 52.4 %).
By contrast, a difference was discovered in the use of fluoride varnish in dentist's offices. In the test region, 59.5 % of sixth graders had received fluoride varnish applications from their family dentist. Among the young people in the control region, the corresponding portion was only 41.4 %.
According to the statements of the parents, 77.6 % of the young people in the test group and 81.0 % of those in the control group had received fluoride tablets at some time; 7.6 % (test group) and 5.2 % (control group) could not remember whether they had taken fluoride tablets or made no statement on this point. On average, fluoride tablets were taken by the pupils in the test region for 1.88 years and in the control group for 2.63 years (p < 0.005).
Results of the binary logistical regression
The binary logistical regression was done for the entire group at the level of dentine caries (D3–6MFT). The final logistic regression model is presented in Table 1. Stepwise logistic regression analysis identified that fissure sealants were significantly associated with the prevention of dental caries (p = 0.023, odds ratio [OR] = 0.856). High frequency of sugar intake (sugar index) was significantly associated with the presence of dentine lesions (D3–6MFT) (p = 0.038, OR = 1.030). Early start of tooth brushing and topical fluoride application were also left over in the final model.
Discussion
In the course of this study, the dental health of 12-year-olds was ascertained in two regions in Germany, and all findings were classified according to the ICDAS II criteria. Because only a few studies have hitherto been conducted using this system, comparisons with the results of other authors are only possible to a limited degree. One problem was to transliterate the ICDAS codes in DMFT findings in accordance with the WHO standard. Braga et al. [14] compared the caries experience of 252 children aged 3 to 5 years. For this purpose, the dmft score was determined according to WHO criteria on the one hand and according to ICDAS criteria on the other. The difference in the dmft index between the two methods was not significant when the cut-off point for caries was set at code 3 and registered using the ICDAS system. If codes 1 and 2 (initial enamel caries) were included as "d", the ICDAS method yielded dmft scores which were four or three times higher, respectively, compared to the WHO standard method. If caries was only included in the dmft calculation at ICDAS code 4, this resulted in a significantly lower dmft score than if registered in accordance with the WHO standard. Jablonski-Momeni et al. [13] showed that ICDAS-II code 3 corresponds histologically to a dentine lesion.
In this study, the cut-off point for caries was also set at code 3 when calculating the DMFT index and marked as D3–6MFT. If we choose this approach, the difference between sixth graders with and without intensive preventive care stands out most clearly: the average D3–6MFT index in the test group of the parallelized sample amounted to 0.88, in the comparison group to 1.73 (Fig. 2). The D5,6MFT was contrasted with this by way of comparison. The difference in caries experience between the groups (test group: 0.50; control group: 0.77) remained significant, yet shrank by two-thirds. This clearly shows that the difference between the test and control group depends greatly on the mode used to record caries [19].
In order to detect children with an enhanced caries risk in the course of our study, social characteristics in the respective settings were also used along with the schools' DMFT averages. Many authors suggest this method as a possible strategy for detecting individuals who are at risk and can be better reached in "settings" (schools or municipal regions) or by focusing more strongly on specific ethnic minorities [20, 21]. The SiC index can be used as a benchmark for increased caries risk in a population [22].
We were able to enhance the validity of our results by successfully parallelizing the samples based on five characteristics. Nearly every pupil in Marburg was paired with a "statistical twin" from the extensive comparison group in Osnabrück. This enabled us to avoid a subsequent "selectivity bias" in the test group.
Topically applied fluoride preparations prevent caries not only by increasing the remineralization rate, but also by inhibiting the progression of initial lesions [23]. The results of our study appear to corroborate this effect: for initial lesions with an ICDAS characteristic of 1 and 2, an average of 1.80 was found in the test region, and 2.14 in Osnabrück (Fig. 2). Here, the groups did not differ significantly from each other.
Using the ICDAS II method in caries epidemiological studies is undoubtedly more laborious (the tooth surfaces must be dried with compressed air, patients are examined lying down) and also entails a more elaborate mode of recording. The examination of a child using ICDAS II criteria takes longer than using the WHO standard, and yields a larger amount of data which also takes longer to process. On the other hand, the ICDAS method can detect not only carious lesions needing restorative treatment, but also the stages of disease at which prevention is still effective, thus enabling invasive measures to be postponed. As this study shows, the mean difference between averages of caries scores of test and comparison groups depends on the cut-off point used (D3–6MFT vs. D5,6MFT). This indicates that early stages of caries should also be included in the evaluation of preventive measures. In view of the increase in the number of "caries free" young people according to WHO criteria, it is also recommendable to shift to a more finely graded registration of caries in order to be able to estimate a suspected shift in the direction of caries lesions which only cavitate later on.
To compare caries prevalence in this study with other national and international results, it is advisable to use the D5,6MFT since it is by definition closer to the WHO standard. Hence a comparison with the most recent national studies turns up similar values: among 12-year-olds, an average of 0.72 DMF teeth were registered [24]. A comparison with European data is only possible to a limited extent at this juncture, because at present there are but a few published studies including ICDAS criteria in the age group of 12-year-olds. Augustsdottir et al. [16] examined 757 twelve-year-olds in a national study in Iceland. Here, the average D3–6MFT was 1.43, while the average D1,2S was 4.47 and thus substantially higher than in our study. The SiC index for 12-year-old children in Iceland was 3.7 by visual examination.
Considering that the 12-year-olds in this study were recruited primarily from settings with above-average caries experience, the D5,6MFT scores in both regions (0.5 or 0.77, respectively) can be assessed as especially positive. This suggests a further decline among young people with a higher caries risk. The goal set by the “German Dental Association” for 2020 — average DMFT score <1 for 12-year-olds [25], has also been reached in a sample with high caries prevalence.
As the multivariate analysis of the overall sample showed, fissure sealing exhibits the most distinct effect of the measures used in individual prevention. In this context, sixth graders in Marburg showed a higher level of fissure sealing and restorative treatment, implying that intensive group prevention also enhances the willingness to make use of individual prevention and dental treatment. Marburg pupils are not only examined by public health dentists employed by the community twice a year, but also receive information on preventive measures from their family dentists. Another indication of increased use of individual prevention is the fact that fluoride varnish applications from the family dentist were more frequent among Marburg sixth graders, despite the offer of group prevention, than in the control group. In the regression analysis, the positive influence of fluoride varnish applications overall (group and individual prevention) on the D3–6MFT was confirmed. In the literature, various fluoride varnish programs are assigned caries reduction rates from 18 % to more than 70 % [8, 9, 26].
The regression analysis also yielded a correlation between caries experience and the number of sugar impulses. In the literature, we find various statements regarding the influence of diet. Pereira et al. [27] found a connection between the sugar intake of 12-year-olds in Brazil and non-cavitating lesions, but not with the DMF-S value. A data analysis from a random sample of 1,450 preschoolers in Great Britain showed a significant caries-inhibiting effect if the teeth were brushed twice a day with toothpaste containing fluoride. Foods and beverages containing sugar were not associated with the appearance of caries unless the children only brushed their teeth once a day or less [28]. In a study of American preschoolers, the consumption of chips was correlated with caries as a significant factor along with the traditional risk parameters (i.e., the presence of plaque, sugar intake and socioeconomic status) [29]. Although a current overview of the role of nutrition and health mentions that the cariogenic effect of sugary foodstuffs can be reduced by using fluoridated products and good oral hygiene [30], it is nonetheless made clear that a primary goal should be to reduce sugar intake because this is related to dental health.
The results of our study confirm the positive effect of the Marburg intensive prevention program on the dental health of 12-year-old pupils with a high risk of caries. The caries diagnosis with the ICDAS II proved in the course of the study to be a suitable instrument for more clearly illustrating group differences. The less frequent occurrence of ICDAS codes 3 and 4 in the test group demonstrates that the fluoride varnish program studied here inhibits primarily the progression of initial lesions.
References
Naujoks R (1985) Die Mundgesundheit der deutschen Bevölkerung. Internationaler Vergleich und Ausblick. ZWR 94:714–719
Momeni A, Hartmann T, Born C, Heinzel-Gutenbrunner M, Pieper K (2007) Association of caries experience in adolescents with different preventive measures. Int J Public Health 52:393–401
Pieper K, Born C, Hartmann T, Heinzel-Gutenbrunner M, Jablonski-Momeni A (2007) Association of preventive measures with caries experience expressed by outcome variables. Schweiz Monatsschr Zahnmed 117:1038–1044
Schulte A, Momeni A, Pieper K (2006) Caries prevalence in 12-year-old children from Germany. Results of the 2004 national survey. Community Dent Health 23:197–202
Truin GJ, van Rijkom HM, Mulder J, van't Hof MA (2005) Caries trends 1996–2002 among 6- and 12-year-old children and erosive wear prevalence among 12-year-old children in The Hague. Caries Res 39:2–8
Cooper H, Smaje C, Arber S (1998) Use of health services by children and young people according to ethnicity and social class: secondary analysis of a national survey. Br Med J 317:1047–1051
Ellwood RP, Davies GM, Worthington HV, Blinkhorn AS, Taylor GO, Davies RM (2004) Relationship between area deprivation and the anticaries benefit of an oral health programme providing free fluoride toothpaste to young children. Community Dent Oral Epidemiol 32:159–165
Helfenstein U, Steiner M (1994) Fluoride varnishes (Duraphat): a meta-analysis. Community Dent Oral Epidemiol 22:1–5
Marinho VC, Higgins JP, Logan S, Sheiham A (2003) Topical fluoride (toothpastes, mouth rinses, gels or varnishes for preventing dental caries in children and adolescents). Cochrane Database Syst Rev 4
World Health Organization (1997) Oral health surveys. Basic methods, 4th ed. World Health Organization, Genf
Ismail A (2004) Diagnostic levels in dental public health planning. Caries Res 38:199–203
Pitts NB (2004) “ICDAS” — an international system for caries detection and assessment being developed to facilitate caries epidemiology and appropriate clinical management. Community Dent Health 21:193–198
Jablonski-Momeni A, Stachniss V, Ricketts DNJ, Heinzel-Gutenbrunner M, Pieper K (2008) Reproducibility and accuracy of the ICDAS-II for detection of occlusal caries in vitro. Caries Res 42:79–87
Braga MM, Oliveira LB, Bonini GA, Bönecker M, Mendes FM (2009) Feasibility of the International Caries Detection and Assessment System (ICDAS-II) in epidemiological surveys and comparability with standard World Health Organization criteria. Caries Res 43:245–249
Sohn W, Ismail A, Amaya A, Lepkowski J (2007) Determinants of dental care visits among low-income African-American children. J Am Dent Assoc 138:309–318
Augustsdottir H, Gudmundsdottir H, Eggertsson H, Jonsson SH, Gudlaugsson JO, Saemundsson SR, Eliasson ST, Arnadottir IB, Holbrook WP (2010) Caries prevalence of permanent teeth: a national survey of children in Iceland using ICDAS. Community Dent Oral Epidemiol 38:299–309
International Caries Detection and Assessment System (ICDAS) Coordinating Committee (2009) Criteria Manual. Bogota, Colombia and Budapest, (www.icdas.org)
Winkler J (1998) Die Messung des sozialen Status mit Hilfe eines Index in den Gesundheitsurveys der DHP. In: Ahrens W, Bellach BM, Jöckel KH (eds) Messung soziodemographischer Merkmale in der Epidemiologie. RKI-Schriften 1/98. MMV Medizin Verlag, München, pp 69–74
Amarante E, Raadal M, Espelid I (1998) Impact of diagnostic criteria on the prevalence of dental caries in Norwegian children aged 5, 12 and 18 years. Community Dent Oral Epidemiol 26:87–94
Brugman E, Verrips GH, Danz MJ, Kalsbeek H (1998) Dental prevention among Turkish and Moroccan parents in The Hague. Community Dent Health 5:109–114
Truin GJ, König KG, Bronkhorst EM, Frankenmolen F, Mulder J, van’t Hof MA (1998) Time trends in caries experience of 6- and 12-year-old children of different socioeconomic status in The Hague. Caries Res 32:1–4
Bratthall D (2000) Introducing the Significant Caries Index together with a proposal for a new global oral health goal for 12-year-olds. Int Dent J 50:378–384
Featherstone JDB, Ten Cate JM (1988) Physicochemical aspects of fluoride-enamel interactions. In: Ekstrand J, Fejerskov O, Silverstone LM (eds) Fluoride in dentistry. Munksgaard, Copenhagen, pp 125–149
Pieper K (2010) Epidemiologische Begleituntersuchungen zur Gruppenprophylaxe 2009. Gutachten. Deutsche Arbeitsgemeinschaft für Jugendzahnpflege e.V (DAJ), Bonn
Ziller S, Micheelis W, Oesterreich D, Reich E (2006) Goals for oral health in Germany 2020. Int Dent J 56:29–32
Sköld MU, Petersson LG, Lith A, Birkhed D (2005) Effect of school-based fluoride varnish programmes on approximal caries in adolescents from different caries risk areas. Caries Res 39:273–279
Pereira SM, Tagliaferro EP, Pardi V, Cenci MS, Cortellazzi KL, Ambrosano GM, Meneghim Mde C, Pereira AC (2010) Sugar consumption and dental health: is there a correlation? Gen Dent 58:e6–e12
Gibson S, Williams S (1999) Dental caries in preschool children: associations with social class, toothbrushing habit and the consumption of sugars and sugar containing foods. Caries Res 33:101–103
Johansson I, Lif Holgerson P, Kressin NR, Nunn ME, Tanner AC (2010) Snacking habits and caries in young children. Caries Res 44:421–430
Palacios C, Joshipura KJ, Willett WC (2009) Nutrition and health: guidelines for dental practitioners. Oral Dis 15:369–381
Acknowledgement
This study was supported by the German Federal Government (Grant No. BMBF 01EL0617).
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pieper, K., Weber, K., Margraf-Stiksrud, J. et al. Evaluation of a preventive program aiming at children with increased caries risk using ICDAS II criteria. Clin Oral Invest 17, 2049–2055 (2013). https://doi.org/10.1007/s00784-012-0907-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-012-0907-x