
Abstract
Objectives
The aim of this study was to evaluate aging effects on the retentive forces (RFs) of different double-crown systems. The effects of abutment height, inner- and outer-crown-material, taper angle, and artificial aging were analyzed.
Material and methods
Inner (IC) and outer crowns (OC) (240), divided into four groups, 60 specimens each, were manufactured: A: IC = zirconia, OC = electroformed; B: IC = non-precious alloy, OC = electroformed; C: IC = precious alloy, OC = electroformed; D: IC = precious alloy, OC = conventionally cast (control group). Ten specimens each with three different abutment heights and two different tapers were used. Ten thousand separation cycles were performed for each specimen, and the RFs were measured at baseline, 5,000, and 10,000 cycles in the presence of artificial saliva. Data were imported into a statistical software (SPSS, V18) and analyzed by a multivariate ANOVA test. Significance level was set at 5 %.
Results
Group D showed highest RFs (baseline: 4.0 N; 5,000 cycles: 3.9 N; 10,000 cycles: 3.9 N) compared to A, B, and C (baseline: 2.6/3.5/2.6 N; 5,000 cycles: 2.5/3.4/2.5 N, 10,000: 2.5/3.3/2.5 N). RF was dependent on material (p < 0.001). The RF of groups A, B, and C were dependent on abutment height (p < 0.001), taper angle (p < 0.001), and artificial aging (p < 0.001). Group D showed no correlation between retentive force and abutment height (p = 0.550).
Conclusions
Wear caused loss of RF in all evaluated groups. However, the material used exhibited significant influence. Conventionally, cast DCs can provide higher RFs, and electroformed DCs can provide more predictable results.
Clinical relevance
In clinical cases with few and short abutment teeth, conventionally cast DCs can rather provide the necessary RF than electroformed DCs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The use of removable dental prosthesis (RDP) for partially edentulous patients has proven its clinical suitability successfully for decades [1–5]. Significant improvement of quality of life has been observed in patients after treatment with RDPs [6–8]. Double-crown systems are an alternative treatment option to traditional clasp-retained dentures. High intraoral comfort and favorable long-term survival rates were reported for conical [6, 9, 10] and telescopic double crowns [8, 11, 12]. In Germany, 53.1 % of all inserted RDPs were retained by double crowns in the year 1995 [4]. A number of studies evaluated the clinical performance of double-crown-retained RDPs. Koller et al. reported mean survival rates of 90.0 % to 95.1 % after 4 to 5.3 years for RDPs in 2011, including 11 clinical trials [13]. In a recent study, Szentpetery et al. reported a survival rate of 93.9 % for abutment teeth provided with telescopic crowns, while the survival rate for the crowns was 87.5 % after 3 years. The survival rate correlated to the “number of telescopic crowns,” “abutment distribution,” “vitality,” and “gender” [14]. Double-crown systems, besides those with clearance fit, provide all functions demanded of retentive elements like retention, guidance, support, and protection from movements. The chewing force is transferred along the long axis of the abutment tooth, preserving the integrity of the periodontal ligament [2, 5, 15–17]. Several design concepts like telescopic crowns, conical crowns, electroformed double crowns, and clearance fit double crowns were described for double-crown systems. All principles are intended to cover special fields of application and to provide sufficient retentive force (RF). Double crowns with friction fit provide RF utilizing a piston-cylinder effect [2, 17, 18], and conical crowns exhibit RF from a pressing effect caused by the geometry of the surfaces (“keying”) [2, 19]. Electroformed crowns get the RF from hydraulic impact and adhesion (“capillarity”) [18, 20, 21]. Clearance fit DCs do not provide any RF [22]. The RF of a telescopic crown depends on the contact surface between primary and secondary crowns and therefore on the accuracy of the dental laboratory technician [5]. The RF of conical crowns can be controlled by modifying the taper angle and abutment height [2, 19]. Beuer et al. reported that the RF of electroformed double crowns is dependent on the material of the primary crowns, taper angle, and abutment height [20]. The retentive forces of telescopic DCs are present over the whole removing process, while conical crowns and electroformed DCs can be removed forceless after an initial force is overcome [19, 22, 23]. The different types of retention result in different contact wear characteristics at the surfaces of the double crowns. Friction and keying cause wear by abrasion, adhesion, and consecutively surface spalling [12, 24]. The retention mode of electroformed double crowns is not based on direct surface contact of the two parts of the crowns. In theory, they should not subject any wear. Weigl et al. reported no significant loss of retentive force after 100,000 cycles of artificial aging [18]. Electroformed double-crown system enables clinical treatment concepts like the passive fit technique. From the dental laboratory point of view, less special skills are required. However, Weigl et al. reported low initial retentive forces for primary crowns fabricated from leucite-glass ceramics with a taper angle of 2° [18, 21]. No data are available on the wear of electroformed double-crown systems with primary crowns having a taper angle different from 0° or from other than all-ceramic materials. The aim of this study was to determine the retentive forces of electroformed DCs and to evaluate aging effects. In addition, the effects of “abutment height,” “taper angle,” and “material” of the primary crowns should be documented on the outcomes. The working hypothesis was that different fabrication methods of the secondary crowns will show different aging effects and therefore different influence on the retentive forces. Additionally, it was hypothesized that different tapers, abutment heights, and materials of the primary crown will show an impact on these aging effects.
Materials and methods
Mandibular premolars with different abutment heights of 5, 7, and 9 mm were designed using a computer program (AutoCad, AutoDesk, Munich, Germany). A total of 240 metal abutment teeth (n = 80 per height) were manufactured using rapid prototyping technology (Eosint 270, Electro Optical Systems, Kreiling, Germany). Impressions were made with polyether (Impregum, 3 M Espe, Seefeld, Germany), and mastercasts were fabricated (OctaStone, Hereaus Kulzer, Hanau, Germany).
The primary crowns (PC) were classified in three groups corresponding to abutment length and subsequently modeled in wax. Half of the specimens of each group were provided with a taper angle of 0° and the other half with a taper angle of 2°.
Four combinations of materials were tested:
-
60 precious alloy primary crowns with conventionally cast secondary crowns
-
60 precious alloy primary crowns with electroformed secondary crowns
-
60 non-precious alloy primary crowns with electroformed secondary crowns
-
60 zirconia primary crowns with electroformed secondary crowns
Figure 1 shows the distribution of the different groups of specimen.

Distribution of the different specimen groups
Primary crowns (120), 40 of each length divided into 20 of each taper angle, were fabricated from precious alloy (BioPortadur, Wieland, Pforzheim, Germany). Wax patterns were fabricated on the master casts, invested (StarVest-Optima-2, Weber Dental, Stuttgart, Germany), and cast in precious alloy. If necessary, the fit was improved by adjusting the crowns using a red ring diamond (Komet, Lemgo, Germany) as described in previous studies [25, 26]. All primary crowns were ground in a surveyor (F1, DeguDent, Hanau) with special burs providing a taper of 0° or 2°.
Sixty more primary crowns were fabricated from non-precious alloy (remanium 2000+, Dentaurum, Ispingen, Germany). The fabrication was similar to the precious alloy group; however, a suitable investing material (Jet 2000, Siladent, Goslar, Germany) was used. The primary crowns were fabricated according to the specifications described in Fig. 1.
Sixty primary crowns were made from zirconia. Wax patterns were scanned and digitized with a CAD/CAM-system (CEREC inLab, Sirona Dental Systems, Bensheim, Germany). The CAD/CAM-system did not offer the possibility to design double crowns virtually when the specimens were manufactured. However, today, almost all systems offer the possibility of designing primary crowns by a CAD program. The primary crowns were milled from presintered zirconia (YZ-Cubes, Vita, Bad Saeckingen, Germany) and sintered in a special furnace (Thermo-Star, Nabertherm, Lilienthal, Germany) at a temperature of 1,520 °C for 3 h. After the sintering process, the marginal accuracy was checked and adjusted if necessary [25, 26]. The zirconia primary crowns were milled and polished with a special bur kit (set 4430 and 4431, Komet) mounted in a turbine (TurboJet, Acurata, Thurmansbang, Germany) with water cooling. The zirconia crowns showed tapers and abutment heights as described in Fig. 1.
All manufactured primary crowns had a chamfer of 0.3 mm located 0.5 mm above the margin to avoid the influence of keying on the RFs.
Sixty precious alloy primary crowns were provided with conventionally cast secondary crowns (SC). Resin material (pattern resin, GC Corp., Tokio, Japan) was used for shaping the secondary crowns and invested (StarVest-Optima-2). Each resin pattern was covered with a thin layer of wax to avoid misfits by moisture expansion. After casting in precious alloy (BioPortadur, Wieland), the secondary crowns were cleaned. To eliminate any distortion of the retentive force measurements, no further treatment was conducted.
Another 180 secondary crowns were produced by electroforming technique. The electroforming process was accomplished according to the manufacturer's recommendations (AGC Micro, Wieland). A thin layer of conductive silver lacquer was brushed onto the primary crowns. Afterwards, a 300-μm layer of gold was applied in a 6-h process. The electroformed secondary crowns were faced with pattern resin to obtain stability.
All primary crowns were cemented (Ketac Cem, 3M ESPE) on the artificial abutment teeth. After 24 h, the retentive forces were measured.
A special device to enable artificial aging of the double crowns was required. A prerequisite for this device was to ensure that the secondary crowns could be removed in one direction only (Fig. 2).

Scheme of the specimen-holder. 1 Gadget to mount the die of the chewing simulator, 2 ball head joint, 3 guiding pins, 4 gadget to mount and dismount the specimen, 5 pattern resin to fixate the outer crown, 6 artificial tooth in a hemisphere of resin, 7 screw thread to mount the chewing simulator, 8 screw to adjust the specimen, 9 specimen
Ten thousand separation cycles were performed in a chewing simulator (ChewingSimulator CS 4, SD Mechatronik, Feldkirchen Westerham, Germany) at a descending speed of 60 mm/s and an ascending speed of 10 mm/s. The joining force was set at 20 N. Thermocycling at a temperature range between 5 °C and 55 °C was included to the artificial aging. The specimens were mounted perpendicularly to the long axis of the abutments.
Retentive force measurements were carried out at 0 (baseline), 5,000, and 10,000 separation cycles. A ring of wire was attached to the electroformed secondary crowns to enable removing. In case of the conventionally cast secondary crowns, the ring was already created in the wax pattern and cast. The measurements of retentive forces were performed in a universal testing machine (Type 1445, Zwick/Roell, Ulm, Germany) in the presence of artificial saliva (Glandosane, cell pharm, Bad Villbel, Germany). In order to avoid horizontal forces during separating process, the secondary crowns were connected to the testing machine via a wire of 0.5 m length [20]. The retentive force of each specimen was determined ten times in a row at a separation speed of 1,000 mm/min. The data were imported into a statistical program (SPSS 17.0, SPSS Inc., Munich, Germany).
Influence of “taper angle,” “abutment height,” “material,” and “artificial aging” on retentive forces was calculated. Statistical analysis was performed with multivariate ANOVA and t-tests at a level of significance of 5 %.
Scanning electron microscopy (SEM) (Supra 55 VP, Zeiss, Oberkochen, Germany) on surface changes was carried out on randomly chosen specimens from each group.
Results
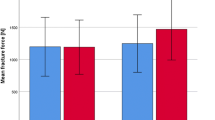
Precious alloy primary crowns with conventionally cast secondary crowns showed the highest mean retentive force of 4.89 N at baseline. The lowest force was 1.45 N after 10,000 separation cycles for zirconia primary crowns with electroformed secondary crowns. Nearly at all different times of the testing process, the precious alloy primary crowns with conventionally cast secondary crowns exhibited the highest mean values of retentive force. The double crowns with non-precious alloy primary crowns had the highest values of retentive force among the groups with electroformed secondary crowns. Mean values of retentive force decreased in most of the groups after aging. The groups with conventionally cast secondary crowns exhibited the highest standard deviations. The groups with electroformed secondary crowns showed standard deviation mean retentive values in the same range (Table 1).
According to the results of variance analysis “material” (p < 0.001), “abutment height” (p < 0.001), “taper angle” (p < 0.001), and “artificial aging” (p < 0.001) had a significant influence on the retentive force. The factor “abutment height” failed to exhibit significant influence (p = 0.550) on the retentive force of double crowns with cast secondary crowns. All other factors showed significant influence on the retentive forces in all groups.
T-tests were conducted to evaluate significant changes in retentive force within the different groups. Only two of six groups showed significant loss of retentive force among the double crowns with conventionally cast outer crowns. The electroformed groups showed miscellaneous outcomes, but 14 of 18 groups showed significant loss (Table 2).
Traces of wear (adhesive wear, abrasive wear, and surface spalling) were detected on most of the scanned specimens in the SEM. In the group with the precious alloy primary and conventionally cast secondary crowns, marks were located on both contact surfaces. In the groups with electroformed secondary crowns, the wear marks were found mostly on the inner surfaces of the secondary crowns. The zirconia primary crowns showed no indication for wear. The traces of wear on the primary crowns and the conventionally cast secondary crowns were narrow scratches (Fig. 3). The electroformed secondary crowns showed large areas of contact wear (Fig. 4). The surface of these extensive marks seemed to be completely flat at low magnification. However, closer examination revealed additional smaller scratches on the surface area of these areas (Fig. 5).

Abrasion mark on a conventionally cast secondary crown (magnification × 500)

Abrasion and adhesion marks on an electroformed secondary crown (magnification 500)

Abrasion mark on an electroformed secondary crown. Many small scratches on an extensive wear mark (magnification × 5,000)
Discussion
Different materials of fabricating secondary crowns led to different aging effects, so this part of working hypothesis could be accepted. However, the expectation that DCs with electroformed secondary crowns would show less signs of wear compared to those with conventionally cast secondary crowns could not be verified. The results of this study were contrary to the results reported by Weigl et al., who found no significant loss of RF at electroformed double crowns [18]. No consensus can be found in the literature concerning the number of cycles during artificial aging and its relevance for in vivo conditions. Some authors prefer 10,000 cycles [27, 28], and Weigl et al. chose 100,000 cycles [18]. Weigl et al. subjected electroformed double crowns with primary crowns made from all-ceramic material (Empress®, Ivoclar Vivadent) to 100,000 separation cycles. They found no statistically significant difference in RF before and after artificial aging [18]. Ten thousand separation cycles correspond to a clinical service time of 13 to 14 years expecting two insertions per day. Minagi et al. showed that after 10,000 cycles of artificial aging, a significant decrease of retentive force occurred. The investigated double crowns had a taper angle of 4° and an abutment height of 4 mm [27]. A study of Ohkawa et al. revealed loss of RF in all investigated crowns due to wear. The authors also described that DCs with tapers of 2°, 4°, and 6° exhibited less decrease of retentive force compared to those with a taper of 0° after 10,000 separation cycles [28]. Most of the tested groups in the present study showed a decrease of retentive force due to artificial aging. In accordance to the results of Ohkawa, specimens with a taper of 2° showed less signs of wear than those with 0° [28]. The groups which displayed the least loss of retentive force were those with conventionally cast secondary crowns. They also showed the highest retentive forces before and after artificial aging. Nevertheless, they exhibited the highest standard deviations of all test groups, while the electroformed double crowns had low standard deviations. It can be assumed that the retentive force of electroformed double crowns is more predictable than the RF of conventionally cast double crowns. Among the groups with electroformed secondary crowns, those with primary crowns of non-precious alloy showed the highest retentive forces. A possible reason for this could be the use of a special non-precious alloy activator. The silver laquer was applied with a paint brush as recommended by the manufacturer. The use of an air jet pistol is recommended by most of the manufacturers nowadays to ensure thin and uniform layers of the silver laquer. This might have a major influence on the retention mode of electroformed double crowns [29]. Further investigations on the influence of the metal activator and the thickness of the silver laquer layer on the retentive force of electroformed double crowns are required.
RDPs retained by double crowns show favorable survival rates dependent on various factors like “number of abutments,” “abutment distribution,” “vitality of the abutment tooth,” and “gender of the patient” [14]. Laboratory studies are suitable to survey some of the factors influencing and changing the retentive forces of double-crown systems. Advanced in vitro trials are able to mimic clinical situations to a high extent. For instance, the familiar fact that the presence of saliva affects the retentive force of double crowns was investigated by Gungor et al. [2]. Mucin-based artificial saliva products have proven its suitability to substitute human saliva [30]. All measurements were conducted under standardized laboratory conditions using a universal testing machine controlled by computer software as described in previous studies [18, 27, 28].
According to Gungor et al. the retentive force of a conical crown depends on “taper angle,” “abutment height,” and “cycles of wear” [2]. Ohkawa et al. analyzed the influence of “taper angle,” “abutment height,” and “artificial aging” on the retentive force of double crowns. They showed that the taper displayed higher influence on the retentive force than the abutment height. Furthermore, the DCs with a taper of 2° exhibited the least decrease of retentive forces after aging. Nevertheless, DCs with a taper angle of 0° showed the highest values of retentive force before and after artificial aging [28]. Beuer et al. revealed in 2010 that the retentive force of electroformed double crowns correlates with “taper angle,” “abutment height,” and “material of the primary crowns.” Zirconia primary crowns showed higher RFs than those made from precious alloy. Increasing abutment heights and decreasing taper angles also led to higher retentive forces [20]. In the present study, the retentive force of all groups was dependent on “material” (p < 0.001), “taper angle” (p < 0.001), and “artificial aging” (p < 0.001). In contrast to the specimens with electroformed secondary crowns (p < 0.001), in the group with conventionally cast secondary crowns, “abutment height” (p = 0.550) showed no significant influence on RFs. This can be explained by the fact that the dental technician manufacturing the crowns is adjusting the retentive forces of conventionally cast double crowns [5].
Becker and Körber postulated retentive forces of 3.5 to 7 N for telescopic and conical double crowns [31, 32]. Almost all conventionally cast double crowns fulfilled these requirements. Electroformed specimens with a taper angle of 0° almost reach this goal. The groups with electroformed secondary crowns and a taper angle of 2° showed results below 3.5 N. A major field of application for electroformed DCs is implant supported RDPs with passive fit concept. This concept helps to avoid mechanical stress on the dental implants and implant-supported prosthetics [33]. The advantages of this technology cannot be accomplished using DCs with a taper angle of 0°. Slightly deviant abutment angulations would lead to high degrees of tensile stress and wear during insertion and removal of the denture.
Bayer et al. pointed out that RDPs with conventionally cast double crowns provided lower retentive forces in vivo than in vitro [34].
The different traces of wear at the contact surfaces of the DCs apparent in the SEM pictures can be explained by the different modes of creating retentive force and by the fabrication technologies. Due to the fabrication process, the conventionally cast double crowns show contact and wear in small areas. These contact areas cause very small and linear abrasion marks. In theory, the two parts of electroformed double crowns should not get in contact at all. However, on the SEM pictures, it became obvious (Figs. 4 and 5) that contact was present. As a result of the precise fabrication process and the accurate fit of primary and secondary crowns, extended contact areas are more likely to be found compared to the conventionally cast DCs.
The following limitations apply to this study: (1) Only one DC was tested and subjected to artificial aging at a time. In clinical use, a minimum of two attachments is necessary. The influence of the second DC was not considered. (2) In vivo, the electroformed secondary crowns are luted to a supporting framework, which provides higher stability. In this study, the highest thickness for electroformed crowns was preset, and the secondary crowns were faced with resin (Pattern Resin, GC) to avoid plastic deformation. However, it cannot be excluded that this proceeding had a certain effect on the results. (3) Only one artificial saliva and (4) one electroforming system were tested. (5) Horizontal forces which are to be expected during the chewing process were not simulated. Further studies have to clarify the impact of these horizontal forces on the wear of electroformed double crowns.
Conclusion
Considering the limitations of the study, the following conclusions can be drawn:
-
1.
Conventionally cast DCs provided higher RFs than electroformed DCs.
-
2.
Electroformed DCs showed more homogenous RFs than conventionally cast DCs.
-
3.
The RFs of electroformed DCs were dependent on abutment height and taper angle, conventionally cast DCs only on taper angle.
-
4.
Electroformed DCs showed no advantage in terms of wear.
References
Behr M, Hofmann E, Rosentritt M, Lang R, Handel G (2000) Technical failure rates of double crown-retained removable partial dentures. Clin Oral Investig 4:87–90
Gungor MA, Artunc C, Sonugelen M (2004) Parameters affecting retentive force of conus crowns. J Oral Rehabil 31:271–277
Hofmann E, Behr M, Handel G (2002) Frequency and costs of technical failures of clasp- and double crown-retained removable partial dentures. Clin Oral Investig 6:104–108
Owall G, Bieniek KW, Spiekermann H (1995) Removable partial denture production in western Germany. Quintessence Int 26:621–627
Perel ML (1973) Telescope dentures. J Prosthet Dent 29:151–156
Grossmann AC, Hassel AJ, Schilling O, Lehmann F, Koob A, Rammelsberg P (2007) Treatment with double crown-retained removable partial dentures and oral health-related quality of life in middle- and high-aged patients. Int J Prosthodont 20:576–578
Inukai M, Baba K, John MT, Igarashi Y (2008) Does removable partial denture quality affect individuals' oral health? J Dent Res 87:736–739
Wostmann B, Balkenhol M, Kothe A, Ferger P (2008) Dental impact on daily living of telescopic crown-retained partial dentures. Int J Prosthodont 21:419–421
Bergman B, Ericson A, Molin M (1996) Long-term clinical results after treatment with conical crown-retained dentures. Int J Prosthodont 9:533–538
Igarashi Y, Goto T (1997) Ten-year follow-up study of conical crown-retained dentures. Int J Prosthodont 10:149–155
Mock F, Schrenker H, Stark H (2005) Success of telescopic crowns—a prospective long term study. Dtsch Zahnärztl Z 60:148–153
Stark H, Schrenker H (1998) Performance of telescopic crown retained dentures—a clinical long term study. Dtsch Zahnärztl Z 3:183–186
Koller B, Att W, Strub JR (2011) Survival rates of teeth, implants, and double crown-retained removable dental prostheses: a systematic literature review. Int J Prosthodont 24:109–117
Szentpetery V, Lautenschlager C, Setz JM (2010) Longevity of frictional telescopic crowns in the severely reduced dentition: 3-year results of a longitudinal prospective clinical study. Quintessence Int 41:749–758
Beschnidt SM, Chitmongkolsuk S, Prull R (2001) Telescopic crown-retained removable partial dentures: review and case report. Compend Contin Educ Dent 22:927–934
Eisenburger M, Gray G, Tschernitschek H (2000) Long-term results of telescopic crown retained dentures—a retrospective study. Eur J Prosthodont Restor Dent 8:87–91
Isaacson G (1969) Telescopic crown retainers for removable partial dentures. J Prosthet Dent 22:436–448
Weigl P, Hahn L, Lauer HC (2000) Advanced biomaterials used for a new telescopic retainer for removable dentures. J Biomed Mater Res 53:320–336
Besimo CH, Graber G, Fluhler M (1996) Retention force changes in implant-supported titanium telescope crowns over long-term use in vitro. J Oral Rehabil 23:372–378
Beuer F, Edelhoff D, Gernet W, Naumann M (2010) Parameters affecting retentive force of electroformed double-crown systems. Clin Oral Investig 14:129–135
Weigl P, Lauer HC (2000) Advanced biomaterials used for a new telescopic retainer for removable dentures. J Biomed Mater Res 53:337–347
Wenz HJ, Hertrampf K, Lehmann KM (2001) Clinical longevity of removable partial dentures retained by telescopic crowns: outcome of the double crown with clearance fit. Int J Prosthodont 14:207–213
Wenz HJ, Lehmann KM (1998) A telescopic crown concept for the restoration of the partially edentulous arch: the Marburg double crown system. Int J Prosthodont 11:541–550
Langer A (1981) Tooth-supported telescope restorations. J Prosthet Dent 45:515–520
Beuer F, Aggstaller H, Edelhoff D, Gernet W, Sorensen J (2009) Marginal and internal fits of fixed dental prostheses zirconia retainers. Dent Mater 25:94–102
Beuer F, Naumann M, Gernet W, Sorensen JA (2009) Precision of fit: zirconia three-unit fixed dental prostheses. Clin Oral Investig 13:343–349
Minagi S, Natsuaki N, Nishigawa G, Sato T (1999) New telescopic crown design for removable partial dentures. J Prosthet Dent 81:684–688
Ohkawa S, Okane H, Nagasawa T, Tsuru H (1990) Changes in retention of various telescope crown assemblies over long-term use. J Prosthet Dent 64:153–158
Diedrichs G, Rosenhain P (1991) Galvano-outer telescope by direct technique. Quintessenz 42:49–56
Hatton MN, Levine MJ, Margarone JE, Aguirre A (1987) Lubrication and viscosity features of human saliva and commercially available saliva substitutes. J Oral Maxillofac Surg 45:496–499
Becker H (1983) Retention mechanism of telescopic crowns. Zahnärtzl Prax 34:281–284
Körber K (1983) Conical crowns—a rational telescopic system. ZWR 92:38–43
Sahin S, Cehreli MC (2001) The significance of passive framework fit in implant prosthodontics: current status. Implant Dent 10:85–92
Bayer S, Stark H, Mues S, Keilig L, Schrader A, Enkling N (2010) Retention force measurement of telescopic crowns. Clin Oral Investig 14:607–611
Acknowledgements
The authors wish to thank Dr. Dietmar Krampe (Wieland Dental) for supporting the study with material.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Engels, J., Schubert, O., Güth, JF. et al. Wear behavior of different double-crown systems. Clin Oral Invest 17, 503–510 (2013). https://doi.org/10.1007/s00784-012-0746-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-012-0746-9