
Abstract
Dental decay and dental treatment are suggested to be related to body growth in children. The aim of this study was first to assess the relation between dental caries and body proportions cross-sectionally in a Suriname caries child population and secondly to investigate whether dental treatment had a significant influence on body growth of these children in a randomised controlled trial using different treatment strategies. Three hundred eighty 6-year-old children with untreated dental decay participated in the study. Caries prevalence and presence of dentogenic infections were recorded. All children were randomly assigned to four different treatment groups ranging from full dental treatment to no invasive treatment at all. Body growth was evaluated by children’s height, weight and body mass index. Participants were evaluated after 6 months and 1, 2 and 3 years. Cross-sectionally, negative correlations were observed between anthropometric measures and the number of untreated carious surfaces and caries experience of the children. Next, no significant differences in growth pattern between the treatment groups were observed. Based on these results, it is suggested that caries activity is a negative predictor for body growth in children and dental intervention does not show significant improvement within 3 years.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
For many years, it is suggested that oral infections negatively affect general health [1]. Several possible explanations for an oral-systemic relationship have been described [2]. Synergism is assumed because some general disease conditions can be associated with oral manifestations that increase the risk of oral disease, and some oral diseases in turn can act as risk factors for general health [3]. Particularly from the field of periodontology, an association has been described between periodontal diseases and certain systemic conditions such as cardiovascular diseases, respiratory diseases, diabetes mellitus, low birth weight and preterm birth [1, 2, 4–8].
Possible systemic effects of dental caries have not been investigated as thoroughly as the systemic effects of periodontal diseases. However, similar outcomes may be expected since dental caries is, like periodontitis, a chronic multifactorial infectious disease. Immune factors have been found to play an essential role in the aetiology of chronic multifactorial diseases [9–12]. De Soet et al. [13] reported an association between dental caries and systemic parameters of inflammation. Moreover, systemic responses to Streptococcus mutans and infected dental pulps have been described [6, 13–15]. Based on these findings, it is suggested that dental caries may induce a systemic immune response that may especially occur when caries progresses into pulpal inflammation [16, 17].
Apart from these immunologic parameters, a reliable clinical diagnostic tool for the measurement of general health is desired in order to identify adverse health outcomes caused by dental decay. Assessment of children’s height and weight is widely accepted as a valid clinical indicator of general health and well-being [18]. Body growth is influenced by genetic, constitutional and environmental factors, including malnutrition and the occurrence of infectious diseases [19, 20]. Dental caries is one of the most prevalent infectious diseases worldwide [3], and it can thus be hypothesised that the possible systemic effects of dental caries could be reflected in a deviant growth pattern. Several studies confirmed this hypothesis as they showed that dental decay and dental treatment affected general body growth in children [21–26]. For example, Acs et al. [21] reported that children with nursing caries weighed significantly less compared to their matched controls. They also presented children with early childhood caries that exhibited growth retardation and showed a “catch-up growth” after dental rehabilitation [21–23]. Furthermore, Aydan et al. [24] reported that children with rampant or nursing caries showed significantly less height or lower weight compared to their matched controls. The affluent studies indicate that with respect to aetiology, it could be that toothache and infection alter eating and sleeping habits, dietary intake and physiological processes that underlie normal growth [21, 24, 27].
If body growth in children is adversely affected by dental decay, problems can be expected especially in those countries and communities where populations are at high risk to develop dental decay due to nutritional deficiencies, high sugar consumption, inadequate exposure to fluorides and limited access to oral health services [28–38]. One of these countries is Suriname. The Interior of Suriname, covering about 80% of the country, is sparsely populated by tribal communities. Children living throughout the Interior, especially in the Creole population, show an increasing percentage of growth retardation that has mainly been attributed to a shortage of protein in the diet [39]. However, given the knowledge that these children also have limited access to oral care services and suffer from untreated dental decay [40], it might be questioned if dental caries and/or concomitant dentogenic infection underlies this growth retardation as well. Insight in this relationship could have important implications for oral health care planning in these countries.
The purpose of the current study was to investigate the relation between oral health and body growth of prepubertal children living throughout the rainforest of Suriname. The study was based on the following hypotheses: Dental caries is inversely proportional to body stature in prepubertal children, and children with untreated dental decay show less body growth compared to children that receive dental treatment of their carious teeth. To test these hypotheses, the study was divided into two parts:
-
1.
The aim of the first part was to analyse the relation between dental caries and body proportions cross-sectionally in a child population with diagnosed dental decay.
-
2.
The aim of the second part of the study was to investigate whether treatment of dental decay had a significant influence on the general health, in terms of body growth, of prepubertal children. Based on a randomised controlled trial (RCT) design, four different dental treatment strategies were applied in order to distinguish the key components of dental treatment that account for the hypothesised improvement in body growth.
Materials and methods
The study population was 6-year-old school children living in the Interior of Surinam, with a non-contributory medical history and with dental decay but without any former dental treatment experience. Seventeen schools, located in two different regions of the rainforest and selected from the database of the Medical Mission, participated in the study. Ethical clearance was obtained from the Director of the Surinam Ministry of Health. All schools were informed about the study and its objectives. The teachers were obligated to inform the parents. The parents or the teacher (in case the parents were illiterate) gave their approval for participation of the child by signing an informed consent letter. Without this approval, children were excluded from the study.
Dental examination
All children received dental examination using a mouth mirror and a dental probe. Dental caries status was recorded individually in terms of dmfs, a numeric expression of the caries prevalence [41]. All children were examined by one of the authors who was calibrated with a gold standard (Cohen’s kappa 0.89). This standard was developed by consensus between two experienced investigators on scoring 25 pictures of molars with and without dentine carious lesions. For the purpose of this study, caries experience in the primary and the permanent dentition were combined in one parameter: total-dmfs. The combined number of total decayed surfaces (total-ds) in primary and permanent dentition was noted separately in order to be able to identify possible effects of untreated carious lesions.
The presence of pulpal inflammation (pulp) was reported if a carious lesion had reached the pulp and/or when pulpal exposure was expected on excavation. The presence of fistulas and/or abscesses (AbFi) as a result of the dentogenic infection was noted. For the purpose of this study, these variables were dichotomized into ‘one or more present’ or ‘not present’.
Anthropometric measures
Height and weight of all children were measured, and from these anthropometric data, the individual body mass index (BMI, weight/height2) was calculated. Height was assessed to the nearest 0.1 cm using a digitally standardised Height Measuring Unit (Soehnle®, Germany). Weight was assessed to the nearest 0.01 kg using a calibrated digital Gamma 7401 scale (Soehnle®). These body growth measurements were performed by one of the team members who was not familiar with the sequence of group allocation of the children.
In order to follow up individual growth, height scores and BMI calculates were transformed into standard deviation scores (SDSH, SDSBMI). In this manner, each child was its own control in the follow-up years. The SDS values in the current study were calculated according to Dutch references [42–45] since there was no growth chart of rainforest children available.
Randomisation and treatment groups
With respect to the RCT part of the study, the Consolidated Standards of Reporting Trials (CONSORT) guidelines were followed. A power analysis indicated that for a one-way ANOVA with four groups, with 80% power, 5% significance level and somewhat less than a medium effect size (f = 0.20), 69 patients per treatment group were sufficient [46]. Taking 30% loss-to-follow-up into account, 100 patients per group were recruited at baseline.
The children were collected from their classroom by one of the participating health care workers who were not familiar with the sequence of group allocation of the children. Upon entrance, the children received a number which corresponded to a specific group number on a computerised random list that was in the possession of the dentist who performed the oral examination of the children.
Children in group 1 received full dental treatment of their primary dentition: All cavities that did not show signs of pulpal inflammation, as described earlier, or dentogenic infection nor gave rise to any pain complaints were restored according to the atraumatic restorative treatment (ART) approach [47]. Teeth with deep carious lesions, where pulpal exposure was likely to be expected in case of excavation, were extracted. Group 2 did not receive any restorative care. Only carious primary teeth with pulpal involvement were extracted. Group 3 only received ART restorative care of cavities that did not show pulpal involvement, whilst deep carious lesions were left untreated. Group 4 received neither restorative treatment nor extraction of any of their carious primary teeth. In all groups, cavities in permanent molars were restored according to the ART approach or extracted when caries had progressed into the dental pulp. When a child reported dental pain, the perpetrating tooth was extracted irrespective of the treatment group. At the end of the study, all children were treated with extractions or ART restorations.
All dental treatments at baseline were performed by four Dutch dentists. At the time of the evaluations, dental treatments, according to the initially allocated group, were performed by other Dutch dentists. The examination of the children at baseline and at the follow-up sessions was performed by the same person not participating in the dental treatments.
Evaluation
The children were evaluated at the start of the study, after 6 months and 1, 2, and 3 years. At each evaluation, the child’s oral health status was evaluated according to the same standards mentioned above. Caries increment was recorded and height and weight were measured. All children received dental treatment according to their treatment group protocol.
Statistical analysis
Statistical analyses were performed using SPSS for Windows, version 12.0.1. Kolmogorov–Smirnov (KS) tests were used to analyse the normality of the distributions of the different continuous parameters. All significant differences were detected at a 95% confidence level.
Variables that showed a normal distribution were analysed using parametric tests (independent samples t tests, general linear model (GLM) for repeated measures). Variables that showed a non-normal distribution were analysed using non-parametric statistics (Spearman correlation, Wilcoxon signed rank tests). Cross-sectional analyses to detect a relationship between dental caries and body proportions were performed at baseline and at all evaluation time points. Body growth was only evaluated on the long run, between baseline and 3 years, rather than between all separate time points.
Results
Part I: cross-sectional analysis
The sample consisted of 380 children (mean age 6.1 years, SD 0.5, range 5.1–7.1). At baseline, the mean total-dmfs was 14.0 (±10.1) and consisted of the decayed factor only because none of the children had received any form of dental treatment before their first visit. This variable showed a skewed distribution (KS, two-sided p < 0.001). The anthropometric data at baseline are summarised in Table 2. Height, weight and BMI were normally distributed (KS, two-sided p > 0.05).
A negative correlation was found between caries prevalence (total-dmfs) and SDSH at baseline (R = −0.13, p = 0.01). This means that children with more decay were more negatively diverging from the standard mean at their individual growth chart. At the different evaluation time points during the study, length and weight measures appeared to show various correlations with the number of untreated dental carious surfaces (total-ds) and caries status (total-dmfs) of the children (Table 1). For BMI or SDSBMI, no significant correlations were found. Independent samples t tests could not prove any significant relation between dentogenic infections and body proportions.
Part II: RCT
Study population
The flowchart in Fig. 1 represents details about the enrolment and allocation of the children. At the enrolment, the caries-free children were excluded. Furthermore, 34 children did not receive the allocated intervention because they showed a contributory medical history or because they had received dental treatment before. The remaining 380 children showed an equal distribution of males (192) and females (188) over the four treatment groups (χ 2 = 4.21, df = 3, p = 0.24), and no differences in mean age amongst the groups were observed (F (3,376) = 0.43, p = 0.73). The demographic characteristics of the sample are presented in Table 2. The children were all from Creole origin. According to the records of the Medical Mission, there were no differences with respect to economical status, care services, medical health burdens, nutritional habits or educational level between the two regions.

Flowchart of the study population
Although all possible efforts were performed to trace the participating children, an increasing dropout was seen during the course of the study (Fig. 1), though equally distributed amongst the different groups at each evaluation as proven by non-significant chi-square tests. The main reasons for absence were illness, moving to another district or work of the parents in the fields. Children that were absent at one evaluation could reappear on the next and were therefore not regarded as lost to follow-up. When a child had missed three or more evaluation visits, he or she was excluded from the study (25 children, 6.6%). At T4, 79 children were absent (20.8%). Therefore, the longitudinal analysis of body growth was performed on 301 children.
Oral health, longitudinal analysis
During the course of the study, all children showed caries activity and developed new dental decay as is shown by the increase in total-dmfs presented in Fig. 2. In this figure, means and standard errors are indicated. The caries increment was significant for children in group 3 where the total-dmfs increased from 11.7 (±9.0) to 16.3 (±10.1; Wilcoxon signed rank test (WSR), p 3 < 0.001) and in group 4 where the total-dmfs increased from 15.4 (±10.7) to 18.4 (±12.4; WSR, p 4 = 0.035). Attention should be paid to the overall drop that was observed between 2 and 3 years and that was most probably caused by exfoliation. Regarding the dentogenic infections, WSR tests showed that during the course of the study, the mean number of carious teeth with suspected pulp involvement decreased significantly in groups 1 and 2 (p < 0.001). An increase was seen in group 4 (p 4 = 0.002). McNemar tests showed that during the course of the study, the number of children that had one or more AbFi decreased in groups 1 and 2 (p (group1) = 0.021, p (group2) < 0.001), whereas an increase was observed in group 4 (p = 0.031).

Caries experience (dmfs-total) during the course of the study. Means and standard errors
Body growth, longitudinal analysis
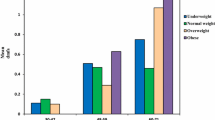
Data of body growth during time are presented in Fig. 3. During the course of the study, all children showed a significant increase in height, weight and BMI (GLM, all p < 0.001). Girls showed a significantly larger increase compared to boys regarding all three growth parameters (GLM, all p < 0.001). All children showed a normal individual growth pattern, and no significant changes regarding the SDS values for heights were observed between baseline and 3 years. No significant differences in growth patterns between the four treatment groups were observed (Figs. 3 and 4).

Body growth between baseline and 3 years. Parameters have different dimensions: height (cm; from 100 cm), SDSH (m), weight (kg), BMI (kg2/cm)

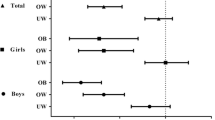
Anthropometric measures per group between baseline and 3 years. SDSHeigth, SDSBMI = standard deviation score height or BMI total rehabilitation (diamond), extraction (square), ART (triangle), no treatment (ex)
Discussion
In this study, a negative correlation was observed between body proportions and the presence of dental caries. In other words, in this particular Surinam Bush Creole population with untreated dental decay, shorter children and/or children that show lower weight tended to have more decay or vice versa.
When discussing a possible relation between dental decay and body growth, one might pose the “hen and egg” question on top. Do children exhibit a diverging growth pattern due to their oral status or does the oral status cause a retard in body growth? The design of the current study was based upon hypotheses regarding the relation between dental decay and body growth as it had been described in existing literature [21–26]. It would be almost impossible to cover all the possible variables that could be suggested to play a minor or major role in this highly complicated interplay between physical processes. The authors resigned in the assumption that healthy children in a homogenous population should show comparable growth patterns. Except for their dental status, the children in the current study population were matched for medical records, and correct randomisation should level out individual bias of other factors that might influence the growth of these children.
The finding from the current study that children with more dental decay showed lower height and weight is in line with earlier studies [21–26, 28, 48]. However, the results can hardly be compared since these studies were conducted retrospectively, concerned case reports, concerned a younger age group or children from heterogeneous backgrounds or consisted of children with diagnosed non-organic growth retardation. The current study includes children with homogeneous demographic characteristics such as age, race, nutritional status, habitat, economic background and both medical and dental history. As such, this study is considered unique and incomparable to studies that have been undertaken upon this subject so far.
The correlation between weight and dental caries could not be established at all time points in the current study. Children that develop dental decay often exhibit cariogenic dietary habits that are highly caloric and inductive of overweight. When these carious lesions progress, the child might develop dental pain that can lead to a refusal of food, provoke lower weight gain or retarded growth. These two patterns may occur simultaneously in different children of one population with the consequence that an overall effect is levelled out. This same argument might explain the absence of a correlation between BMI and dental caries, whereas within BMI, an internationally accepted measure for growth, weight is represented [41, 43].
Considering the longitudinal analyses, it was observed that with regard to the stable standard deviation scores of height and BMI during the course of the study, all children showed a normal growth pattern in accordance with their own individual growth curves. Although the curves of children with higher caries rates were in lower SDS ranges, they all showed comparable patterns, and it could thus be concluded that none of the dental intervention strategies had an affect on the body growth of the children in the course of 3 years. This finding is contradictory to those of other studies where a catch-up growth was observed after dental rehabilitation in children with rampant caries and diagnosed, non-organic growth retardation [22, 23, 25]. However, it is not known whether the children in the current study were retarded in their body growth at baseline since no reference growth charts are available for Surinamese children or for this Bush Creole population in particular.
In the current study, girls showed more growth compared to boys. It has been documented that girls show earlier pubertal growth acceleration than boys [44]. Creole girls might experience their menarche at an earlier age than Caucasian girls, and the early onset of their growth acceleration might thus be visible in the results. At baseline, an age of 6 years was set as an inclusion criterion with regard to the cognitive level of the child to cooperate with the dental treatment. Though it seems to be a rather short period of time to evaluate body growth, 3 years was chosen as a cutoff in order to minimise the risk for bias from individual variation both in pubertal onset and in natural tooth exfoliation [49].
Dental caries is classified as an infectious disease, and it has been well established that body growth is negatively influenced by infectious diseases [19, 20]. With the invasive treatment of dental caries, the symptoms of this infectious disease might be contended, but the disease itself is not eradicated. Apparently, all children remained caries-active because they all developed new dental decay during the course of the study. It is therefore suggested that caries activity rather than caries experience may be a negative predictor for body growth in children. This would involve a more prominent role for primary preventive measures within any oral health care programme.
However, body growth is influenced by numerous factors, e.g. regular-occurring other infectious diseases such as malaria and worms and malnutrition [50–52]. Based on the results of the current study, it is therefore not possible to draw definite conclusions upon an exclusive cause-and-effect relationship between neither dental decay or caries activity and body growth. Probably, immunity could serve as a possible link [48, 49]. Future studies should include systemic infectious parameters that can possibly identify more specifically the systemic effects of dental decay and trace responsible underlying factors or mechanisms. These studies should also include children with higher caries levels. The children from the current study showed a moderate caries prevalence according to the severity criteria of the WHO [40, 53]. It could be hypothesised that in children with more dental decay, relations between caries or dental treatment and body growth appear even more evident.
In this study, a negative correlation was found between individual body proportions and dental caries prevalence in a caries-active, prepubertal Surinam child population. No significant influence of dental treatment on the body growth of these children could be established. Based on these results, it might be suggested that caries activity is a negative predictor for body growth in children. Future studies should focus on child populations with more caries and include systemic parameters for infection before definite conclusions upon a true relation between dental caries and systemic health can be drawn.
References
Garcia RI, Henshaw MM, Kall EA (2000–2001) Relationship between periodontal disease and systemic health. Periodontology 25:21–36
Li X, Kolltveit KM, Tronstad L, Olsen I (2000) Systemic diseases caused by oral infection. Clin Microbiol Rev 13:547–558
Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C (2005) The global burden of oral diseases and risks to oral health. Bull World Health Organ 83:661–669
Beck JD, Slade G, Offenbacher S (2000) Oral disease, cardiovascular disease and systemic inflammation. Periodontology 23:110–120
Drangsholt MT (1998) A new causal model of dental disease associated with endocarditis. Ann Periodontol 3:184–196
Glurich I, Grossi S, Albini B, Ho A, Shah R, Zeid M, Baumann H, Genco RJ, De Nardin E (2002) Systemic inflammation in cardiovascular and periodontal disease: a comparative study. Clin Diagn Lab Immunol 9:425–432
Loesche WJ, Schork A, Terpenning MS, Chen YM, Dominguez BL, Grossman N (1998) Assessing the relationship between dental disease and coronary heart disease in elderly U.S. veterans. J Am Dent Assoc 129:301–311
Mojon P (2002) Oral health and respiratory infection. J Can Dent Assoc 68:340–345
Balfour S (2007) Bacteria in Crohn’s disease mechanisms of inflammation and therapeutic implications. J Clin Gastroenterol 41:S37–S43
de Sa AR, Moreira PR, Xavier GM, Sampaio I, Kalapothakis E, Dutra WO, Gomez RS (2007) Association of CD14, IL1B, IL6, IL10 and TNFA functional gene polymorphisms with symptomatic dental abscesses. Int Endod J 40:563–572
Pietruska M, Zak J, Pietruski J, Wysocka J (2006) Evaluation of mCD14 expression on monocytes and the blood level of sCD14 in patients with generalized aggressive periodontitis. Adv Med Sci 51(Suppl 1):166–169
Tetley TD (2005) Inflammatory cells and chronic obstructive pulmonary disease. Curr Drug Targets Inflamm Allergy 4:607–618
de Soet JJ, Schriks MCM, Kratz E, Poland DCW, van Dijk W, van Amerongen WE (2003) Dental caries related to plasma IgG and alpha1-acid glycoprotein. Caries Res 37:79–84
Hahn CL, Liewehr FR (2007) Update on the adaptive immune responses of the dental pulp. J Endod 33:773–781
Kim SA, Lim SS (2002) T lymphocyte subpopulations and interleukin-2, interferon-gamma, and interleukin-4 in rat pulpitis experimentally induced by specific bacteria. J Endod 28:202–205
Duggal MS, Nooh A, High A (2002) Response of the primary pulp to inflammation: a review of the Leeds studies and challenges for the future. Eur J Paediatr Dent 3:111–114
Skogedal O, Tronstad L (1977) An attempt to correlate dentin and pulp changes in human carious teeth. Oral Surg Oral Med Oral Pathol 43:135–140
de Onis M, Blössner M (2003) The World Health Organization global database on child growth and malnutrition: methodology and applications. Int J Epidemiol 32:518–526
Bhutta ZA (2006) Effect of infections and environmental factors on growth and nutritional status in developing countries. J Pediatr Gastroenterol Nutr 43(suppl):513–521
Mata LJ, Urrutia JJ, Albertazzi C, Pellecee O, Arellano E (1972) Influence of recurrent infection on nutrition and growth of children in Guatemala. Am J Clin Nutr 25:1267–1275
Acs G, Lodolini G, Kaminsky S, Cisneros GJ (1992) Effect of nursing caries on body weight in a pediatric population. Pediatr Dent 14:302–305
Acs G, Lodolini G, Shulman R, Chussid S (1998) The effect of dental rehabilitation on the body weight of children with failure to thrive: case reports. Compend Contin Educ Dent 19:164–171
Acs G, Shulman R, Wai Hg M, Chussid S (1999) The effect of dental rehabilitation on the body weight of children with early childhood caries. Pediatr Dent 21:109–113
Ayhan H, Suskan E, Yildirim S (1996) The effect of nursing or rampant caries on height, body weight and head circumference. J Clin Pediatr Dent 20:209–212
Elice CE, Fields HW (1990) Failure to thrive: review of the literature, case report, and implications for dental treatment. Pediatr Dent 12:185–189
Nicolau B, Marcenes W, Allison P, Sheiham A (2005) The life course approach: explaining the association between height and dental caries in Brazilian adolescents. Community Dent Oral Epidemiol 33:93–98
Thomas CW, Primosch RE (2002) Changes in incremental weight and well-being of children with rampant caries following complete dental rehabilitation. Pediatr Dent 24:109–113
Alvarez JO, Caceda J, Woolley TW, Carley KW, Biaocchi N, Caravedo L, Navia JM (1993) A longitudinal study of dental caries in primary teeth of children who suffered from infant malnutrition. J Dent Res 72:1573–1576
Diehnelt DE, Kiyak HA (2001) Socioeconomic factors that affect international caries levels. Community Dent Oral Epidemiol 29:226–233
Gray MM, Davies-Slowik J (2001) Changes in the percentage of 5-year-old children with no experience of decay in Dudley towns since implementation of fluoridation schemes in 1987. Br Dent J 190:30–32
Haugejorden O, Birkeland JM (2002) Evidence for reversal of the caries decline among Norwegian children. Int J Paediatr Dent 12:306–315
Jamieson LM, Thomson WM, McGee R (2004) Caries prevalence and severity in urban Fijian school children. Int J Paediatr Dent 14:34–40
Marthaler TM, O’Mullane DM, Vrbic V (1996) Symposium report: the prevalence of dental caries in Europe 1990–1995. Caries Res 30:237–255
Miura H, Araki Y, Haraguchi K, Arai Y, Umenai T (1997) Socioeconomic factors and dental caries in developing countries: a cross-national study. Soc Sci Med 44:269–272
Pakhomov GN (1999) Future trends in oral health and disease. Int Dent J 49:27–32
Pilot T (1988) Trends in oral health: a global perspective. N Z Dent J 84:40–45
Reich E (2001) Trends in caries and periodontal health epidemiology in Europe. Int Dent J 51:392–398
Speechley M, Johnston DW (1996) Some evidence from Ontario, Canada, of a reversal in dental caries decline. Caries Res 30:423–427
van der Crabben SN, Heymans HAS, van Kempen AAMW, Holman R, Sauerwein HP (2004) Qualitative malnutrition due to incorrect complementary feeding in Bush Negro children in Suriname. Ned Tijdschr Geneeskd 148:1093–1097 (in Dutch)
van Gemert-Schriks MCM, Amerongen WE, ten Cate JM (2009) Caries prevalence and oral health in Surinam schoolchildren. Community Dent Health 26:116–120
World Health Organization (1997) Oral health surveys: basic methods, 3rd edn. World health Organization, Geneva
Burgemeijer RJF, Fredriks AM, van Buuren S, Verloove-Vanhorick SP, Wit JM (1998) Dutch growth charts. Manual for children’s growth registration and use of growth charts. Bohn Safleu van Loghum, Houten (in Dutch)
Fredriks AM, van Buuren S, Wit JM, Verloove-Vanhorick SP (2000) Body index measurements in 1996–7 compared with 1980. Arch Dis Child 82:107–112
Gerver WJM, de Bruin R (1996) Paediatric morphometrics: a reference manual. Bunge, Utrecht (in Dutch)
van Buuren S, Fredriks M (2001) Worm plot: a simple diagnostic device for modelling growth reference curves. Stat Med 20:1259–1277
Cohen J (1988) Statistical power analysis for the behavioural sciences, 2nd edn. Erlbaum, Mahwah, pp 102–384
Frencken JE, Pilot T, Songpaisan Y, Phantumvanit P (1996) Atraumatic restorative treatment (ART): rationale, technique and development. J Public Health Dent 56:135–140
Low W, Tan S, Schwartz S (1999) The effect of severe caries on the quality of life in young children. Pediatr Dent 21:325–326
Moslemi M (2004) An epidemiological survey of the tome and sequence of eruption of permanent teeth in 4–15-year-olds in Tehran, Iran. Int J Paediatr Dent 14:432–438
Uauy R (2007) Academic–industry partnerships in addressing nutrition–[Infection–immunity–inflammation] interactions. Br J Nutr 98:S17–S23
Uauy R, Kain J, Mericq V, Rojas J, Corvalán C (2008) Nutrition, child growth and chronic disease prevention. Ann Med 40:11–20
Walker SP, Wachs TD, Gardner JM, Lozoff B, Wasserman GA, Pollitt E, Carter JA, International Child Development Steering Group (2007) Child development: risk factors for adverse outcomes in developing countries. Lancet 369:145–157
Marthaler TM, Møller IJ, von de Fehr FR (1990) Symposium report: caries status in Europe and predictions of future trends. Caries Res 24:381–396
Acknowledgements
This study was supported by the Netherlands Institute of Dental Sciences (IOT), the Netherlands Foundation for the advancement of Tropical Research (WOTRO), the Foundation “De Drie Lichten” in The Netherlands and 3M-ESPE. Furthermore, the authors would like to thank the director of the Surinam Ministry of Health and the Medical Mission of Suriname for their intensive and enthusiastic cooperation, the provision of all facilities and their inspiring input.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
van Gemert-Schriks, M.C.M., van Amerongen, E.W., Aartman, I.H.A. et al. The influence of dental caries on body growth in prepubertal children. Clin Oral Invest 15, 141–149 (2011). https://doi.org/10.1007/s00784-010-0380-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-010-0380-3