
Abstract
Purpose
The purpose of this population-based study was to clarify the incidence of knee pain by use of ultrasound (US).
Methods
Medical check-ups were conducted for residents of a mountain village in Japan. The subjects were 149 males and 252 females (802 knees) with a mean age of 63.5 ± 12.5 years. US was used to evaluate the medial joint space of both knees, with and without weight-bearing. For each patient, medial radial displacement of the medial meniscus (MRD) and number of osteophytes were evaluated. A questionnaire was used to determine whether the subjects were currently experiencing knee pain while walking, climbing stairs, or resting that had lasted more than one month. A visual analog scale was used to assess knee pain. The subjects were divided into two groups, those with knee pain (P group) and those without knee pain (non-P group), on the basis of whether a visual analog scale (VAS) was less than or more than 20 mm during walking, climbing stairs, or resting. Logistic regression analysis was used to identify the factors associated with knee pain.
Results
Significantly different weight-bearing MRD (WMRD), osteophytes, and pain while walking, climbing stairs, or resting (p < 0.01) were found between the two groups. Logistic regression analysis showed that WMRD was significantly associated with knee pain during walking or while climbing stairs.
Conclusion
We found that WMRD was significantly associated with knee pain while walking or climbing stairs, which are weight-bearing activities. On the basis of the findings of this study, we believe US is a useful tool for evaluating the factors associated with knee pain in a population-based study.
Level of evidence
Level III.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Despite the importance of knee pain, little is understood about its causes. Neogi et al. [1] investigated the relationship between the radiographic features of osteoarthritis and knee pain. Some studies have reported a significant association between MRI-graded meniscal tears and pain [2, 3] whereas others have not [4]. There have, however, been few reports of population-based studies of the relationship between the presence of a meniscus tear and knee pain [5].
Ultrasound (US) examinations are used for noninvasive assessment of musculoskeletal status. Recently, many studies have reported use of US to evaluate the knee joint, and US evaluation of the meniscal position under load-bearing has been discussed [9, 10]. Kawaguchi et al. [11] used US to evaluate medial radial displacement (MRD) of the medial meniscus in osteoarthritic (OA) and normal knees with and without weight-bearing. During follow-up they found that MRD of the medial meniscus increases with weight-bearing as OA progresses. Yanagisawa et al. [12] reported characteristic changes associated with the rate of development of knee osteoarthritis, and that MRD and osteophytes increase as Kellgren–Lawrence grade increases in morphological evaluation of the knee by use of US. It has therefore become accepted that evaluation of the knee by use of US is useful.
The purpose of this study was to examine the relationship the between MRD, determined by use of ultrasound screening, and knee pain.
Methods
Intra-observer agreement was analyzed for patients attending as outpatients at the Department of Orthopaedic Surgery at Gunma University. To calculate intra-observer agreement, a single observer examined 10 patients and measurements were performed three times at 1-week intervals.
To help prevent lifestyle-related diseases and to aid the early detection of cancer, medical check-ups have been conducted in Japan for residents of a village in which agroforestry and tourism are the main industries. This cross-sectional study was approved by the institutional review board of our institution. All participants, before giving their consent to participate in this study, were informed that their data would be published. In this study, the subjects were selected on the basis of:
-
1
no history of surgical treatment of the knee; and
-
2
no treatment of the knee at the time of this survey.
The exclusion criteria were a history of avascular necrosis, rheumatoid or other inflammatory arthritis, Paget’s disease, villonodular synovitis, joint infection, neuropathic arthropathy, and gout or pseudogout. On the basis of these criteria, the study included 149 males and 252 females (802 knees) with a mean age of 63.5 ± 12.5 years (range 40–87 years).
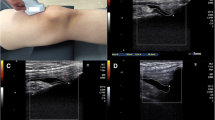
A questionnaire was administered requesting information regarding the subjects’ age, gender, and whether they were experiencing any knee pain, that had lasted more than one month, during walking, climbing stairs, or resting [6]. The location of the knee pain was not restricted, and patients with knee pain in all locations were included. A visual analog scale (VAS) was used to assess knee pain. A VAS consists of a line, 100-mm long, with ends labelled as the extremes of pain. Patients are asked to indicate which point along the line best represents their pain and the distance from the no-pain end to the mark made by the patient is the patient’s pain score. For each subject, we conducted a physical examination of the range of motion (ROM) of the knees, by use of a goniometer, while the patient was in the supine position. US was used to examine both knees to diagnose medial radial displacement (MRD) by use of the LOGIQ e device (GE Health Care, USA) with linear-array probes at 12 MHz. All US examinations were performed by one experienced knee surgeon who was unaware of other aspects of the evaluation. The US evaluations were performed with both knees in complete extension in both the standing and supine positions. MRD was measured on longitudinal US images at the site at which the medial collateral ligament (MCL) was most clearly visualized. Normal MCLs are hyperechoic, covering the medial femoral condyle, the outer margin of the medial meniscus, and the medial tibial plateau. MRD was measured as the distance from the outermost edge of the medial meniscus to a line connecting the femoral and tibial cortices. Marginal osteophytes were defined as those more than 2 mm from the femoral and tibial cortices. When marginal osteophytes were present in the femur or tibia, the MRD was measured on the clearly visualized normal cortical bone continuous with the femoral or tibial marginal osteophytes. Distances were measured by use of electronic calipers. A magnified image was used to measure MRD on the US monitor to an accuracy of 0.1 mm. We defined supine position MRD as weight-bearing medial radial displacement (WMRD) (Fig. 1) [7–12].

MRD was measured on longitudinal US images at the site at which the medial collateral ligament (MCL) was most clearly visualized. OP osteophyte, MM medial meniscus, MCL medial collateral ligament, upside dotted arrow medial radial displacement of the medial meniscus
Data analysis
The subjects were divided into two groups, those with knee pain (P group) and those without knee pain (non-P group), on the basis of whether their VAS was less than or more than 20 mm [13] during walking, climbing stairs, or resting. Age, gender, body mass index (BMI), WMRD, ROM, and the presence or absence of the osteophytes of the knee were compared by use of Welch’s t test and the chi-squared test. Stepwise forward logistic regression analysis was performed with age, gender, BMI, WMRD, ROM and the presence or absence of the osteophytes of the knee as explanatory variables. Moreover, we examined diagnostic efficacy for prediction of knee pain of setting the cut-off of MRD at >5 mm during weight-bearing activities. All statistical analysis was conducted by use of IBM SPSS Statistics 19 software (IBM Japan, Tokyo, Japan); the critical value for significance was set at p < 0.05.
Results
The intraobserver intraclass correlation coefficient (ICC) was 0.961 (p < 0.001) for measurement of WMRD distance. The kappa value was 0.956 for the presence or absence of osteophytes.
The evaluation of the P group during walking included 83 knees. Age was significantly higher in the P group than in the non-P group (p = 0.018). The number of females was significantly greater in the P group than in the non-P group (p = 0.003). BMI was not significantly different. Knee extension and knee flexion were significantly lower in the P group than in the non-P group (p < 0.001). WMRD was significantly greater in the P group than in the non-P group (p < 0.001). Osteophytes of the knee were present in 63.8 % (53/83 knees) of the subjects in the P group and 35.7 % (257/719 knees) of the subjects in the non-P group (Table 1).
Pain was felt in 75 knees when the patients were climbing stairs. Age was significantly higher in the P group than in the non-P group (p = 0.010), and the number of females was significantly greater in the P group than in the non-P group (p = 0.001). Knee extension and knee flexion were significantly lower in the P group than in the non-P group (p < 0.001). WMRD was significantly greater in the P group than in the non-P group (p < 0.001). Osteophytes of the knee were present in 65.3 % (49/75 knees) of the subjects in the P group and 35.8 % (261/727 knees) of the subjects in the non-P group (Table 2).
The P group during rest included 18 knees. The non-P group included the other 784 knees. Age, gender, and BMI were not significantly different. Knee extension and knee flexion were significantly lower in the P group than in the non-P group (p < 0.01). WMRD were significantly greater in the P group than in the non-P group (p < 0.01). Osteophytes of the knee were present in 61.1 % (11/18 knees) of the subjects in the P group and 38.1 % (299/784 knees) of the subjects in the non-P group (Table 3).
Logistic regression analysis showed that WMRD, extension of the knee, and age were significantly associated with knee pain during walking; the odds ratios for WMRD, extension of the knee, and age, were 1.35, 1.17, and 0.97, respectively. Logistic regression analysis showed that WMRD, extension of the knee, and gender were significantly associated with knee pain when climbing stairs; the odds ratios for WMRD, extension of the knee, and gender were 1.42, 1.14, and 2.53, respectively. Logistic regression analysis showed that only extension of the knee was significantly associated with knee pain during resting; the odds ratio for extension of the knee was 1.11 (Table 4).
The diagnostic efficacy of MRD value assessed by use of US for prediction of knee pain during walking was 51.8 % sensitive and 83.4 % specific, corresponding to a negative predictive value of 93.7 % and a positive predictive value of 26.5 % (the positive and negative likelihood ratios were 3.06 and 0.59, respectively) (Table 5). The diagnostic efficacy for prediction of knee pain during climbing stairs was 52.0 % sensitive and 83.1 % specific, corresponding to a negative predictive value of 94.3 % and a positive predictive value of 24.1 % (the positive and negative likelihood ratios were 3.06 and 0.58, respectively) (Table 5).
Discussion
The most important finding of this study was that weight-bearing medial radial displacement was significantly associated with knee pain while walking or climbing stairs, which are both weight-bearing activities. In addition, extension of the knee was significantly associated with knee pain while resting.
Previous reports have been equivocal with regard to whether age is a risk factor for knee pain. McAlindon et al. demonstrated a positive correlation with age [14] whereas others did not [15, 16]. This study showed that age was a risk factor for knee pain during walking. Dacre et al. [17] showed that females and elderly subjects might be more susceptible than other subjects to knee pain. Our study supported this, and showed that gender was a factor predicting knee pain while climbing stairs.
Although knee pain because of a loss of extension is often experienced, there have been few reports of this situation. This study showed that knee extension was significantly lower in the P group in all situations. In addition, extension of the knee was significantly associated with knee pain in all situations.
Although Lanyon et al. [18] reported that pain was associated with the presence of osteophytes on plain radiographs, the presence of osteophytes was not a factor associated with knee pain in our study.
MRI is used to evaluate intra-articular components and the position of the meniscus [19]. However, most images are obtained with the patient in a supine, non-weight-bearing position. In contrast, US can measure meniscal subluxation under axial loading. In addition, MRI is inconvenient, requiring much time to complete the test, and the instrumentation is very expensive. It is, therefore, difficult to use MRI to evaluate the knee joint in population-based studies. For these reasons, we elected to use US for evaluation of the MRD with and without weight-bearing.
Boxheimer et al. [19] demonstrated that meniscal displacement was strongly associated with complex meniscal tears, and that patients with displacement had significantly more pain than did patients with non-displaceable meniscal tears; this was irrespective of concomitant knee abnormalities, because meniscal extrusion may cause bulging and mechanical stretching of the joint capsule, which is richly innervated with pain fibers [21, 22]. Meniscus extrusion ≥3 mm was more frequently observed by MRI for painful than for painless knees [3]. However, only meniscus extrusion was examined in that study, and other pathology associated with knee pain, including tendinitis, bone marrow lesion, and inflammatory synovitis, were not examined. Our study showed that WMRD was a factor associated with knee pain during walking and climbing stairs. The knee pain found in a loaded joint was related to dynamic stress on loading and with movement, which may be why a strong correlation was observed between knee pain and WMRD. Although diagnostic efficacy for prediction of knee pain had low sensitivity, we were able to show a good diagnostic specificity.
Recently, MRD was found to contribute to the progression of joint space narrowing [23]. Although our study showed that US is a useful tool for detection of early changes in MRD, further investigations are necessary to clarify which type of intervention can be used to prevent the progression of MRD.
This study has several limitations. First, we studied meniscal displacement and peripheral joint space at the level of the MCL only; meniscal displacement and joint space in other directions were not estimated. Second, the detailed location of the knee pain could not be identified by use of a questionnaire. Knee pain described in this study might include anterior knee pain, tendinitis-related pain, and medial joint space pain. Third, the US investigations were conducted under static conditions with the knee extended. Flexion of the knee can increase stress on the posterior segment of the meniscus, and subsequently increase extrusion. Fourth, because this was a cross-sectional study, it is necessary to continue research in this area to confirm the changes in MRD by use of a longitudinal design.
Conclusion
To summarize, we found that weight-bearing medial radial displacement was significantly associated with knee pain while walking or climbing stairs, which are weight-bearing activities. On the basis of the findings of this study, we believe US is a useful tool for evaluating the factors associated with knee pain in a population-based study.
References
Neogi T, Felson D, Niu J, Nevitt M, Lewis CE, Aliabadi P, Sack B, Torner J, Bradley L, Zhang Y. Association between radiographic features of knee osteoarthritis and pain: results from two cohort studies. BMJ. 2009;339:b2844. doi:10.1136/bmj.b2844.:b2844.
Torres L, Dunlop DD, Peterfy C, Guermazi A, Prasad P, Hayes KW, Song J, Cahue S, Chang A, Marshall M, Sharma L. The relationship between specific tissue lesions and pain severity in persons with knee osteoarthritis. Osteoarthr Cartil. 2006;14(10):1033–40.
Wenger A, Englund M, Wirth W, Hudelmaier M, Kwoh K, Eckstein F. Relationship of 3D meniscal morphology and position with knee pain in subjects with knee osteoarthritis: a pilot study. Eur Radiol. 2012;22(1):211–20.
Kornaat PR, Bloem JL, Ceulemans RY, Riyazi N, Rosendaal FR, Nelissen RG, Carter WO, Le Hellio Graverand MP, Kloppenburg M. Osteoarthritis of the knee: association between clinical features and MR imaging findings. Radiology. 2006;239(3):811–7.
Englund M, Guermazi A, Gale D, Hunter DJ, Aliabadi P, Clancy M, Felson DT. Incidental meniscal findings on knee MRI in middle-aged and elderly persons. N Engl J Med. 2008;359(11):1108–15.
O’Reilly SC, Muir KR, Doherty M. Screening for pain in knee osteoarthritis: which question? Ann Rheum Dis. 1996;55(12):931–3.
Freidman L, Finlay K, Jurriaans E. Ultrasound of the knee. Skelet Radiol. 2001;30(7):361–77.
Naredo E, Cabero F, Palop MJ. Ultrasonographic findings in knee osteoarthritis: a comparative study with clinical and radiographic assessment. Osteoarthr Cartil. 2005;13(7):568–74.
Van Holsbeeck M, Introcaso JH. Musculoskeletal ultrasonography. Radiol Clin North Am. 1992;30(5):907–25.
Verdonk P, Depaepe Y, Desmyter S, De Muynck M, Almqvist KF, Verstraete K, Verdonk R. Normal and transplanted lateral knee menisci: evaluation of extrusion using magnetic resonance imaging and ultrasound. Knee Surg Sports Traumatol Arthrosc. 2004;12(5):411–9.
Kawaguchi K, Enokida M, Otsuki R, Teshima R. Ultrasonographic evaluation of medial radial displacement of the medial meniscus in knee osteoarthritis. Arthritis Rheum. 2012;64(1):173–80.
Yanagisawa S, Ohsawa T, Saito K, Kobayashi T, Yamamoto A, Takagishi K. Morphological evaluation and diagnosis of medial type osteoarthritis of the knee using ultrasound. J Orthop Sci. 2014;19(2):270–4.
Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain. 1986;27(1):117–26.
McAlindon TE, Cooper C, Kirwan JR, Dieppe PA. Knee pain and disability in the community. J Rheumatol. 1992;31(12):189–92.
Davis MA, Ettinger WH, Neuhaus JM, Barclay JD, Segal MR. Correates of knee pain among US adults with and without radiographic knee osteoarthritis. J Rheumatol. 1992;19(12):1943–9.
Bergström G, Bjelle A, Sundh V, Svanborg A. Joint disorders at ages 70, 75 and 79 years—a cross-sectional comparison. J Rheumatol. 1986;25(4):333–41.
Dacre JE, Scott DL, Da Silva JA, Welsh G, Huskisson EC. Joint space in radiologically normal knees. J Rheumatol. 1991;30(6):426–8.
Lanyon P, O’Reilly S, Jones A, Doherty M. Radiographic assessment of symptomatic knee osteoarthritis in the community: definitions and normal joint space. Ann Rheum Dis. 1998;57(10):595–601.
Boxheimer L, Lutz AM, Zanetti M, Treiber K, Labler L, Marincek B, Weishaupt D. Characteristics of displaceable and nondisplaceable meniscal tears at kinematic MR imaging of the knee. Radiology. 2006;238(1):221–31.
Heppelmann B. Anatomy and histology of joint innervation. J Peripher Nerv Syst. 1997;2(1):5–16.
Dye SF, Vaupel GL, Dye CC. Conscious neurosensory mapping of the internal structures of the human knee without intraarticular anesthesia. Am J Sports Med. 1998;26(6):773–7.
Hunter DJ, Zhang YQ, Tu X, Lavalley M, Niu JB, Amin S, Guermazi A, Genant H, Gale D, Felson DT. Change in joint space width: hyaline articular cartilage loss oralteration in meniscus? Arthritis Rheum. 2006;54(8):2488–95.
Sugita T, Kawamata T, Ohnuma M, Yoshizumi Y, Sato K. Radial displacement of the medial meniscus in varus osteoarthritis of the knee. Clin Orthop Relat Res. 2001;387:171–7.
Conflict of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Yanagisawa, S., Ohsawa, T., Saito, K. et al. Population-based study of the relationship between medial meniscus radial displacement, determined by use of ultrasound screening, and knee pain. J Orthop Sci 19, 954–958 (2014). https://doi.org/10.1007/s00776-014-0628-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00776-014-0628-x