
Abstract
Elevated circulating concentrations of total l-homocysteine (thCys) and free asymmetric dimethylarginine (ADMA) are long-established cardiovascular risk factors. Low circulating l-homoarginine (hArg) concentrations were recently found to be associated with increased cardiovascular morbidity and mortality. The biochemical pathways of these amino acids overlap and share the same cofactor S-adenosylmethionine (SAM). In the present study, we investigated potential associations between hArg, l-arginine (Arg), ADMA and thCys in plasma of patients suffering from rheumatoid arthritis (RA), coronary artery disease (CAD) or peripheral artery occlusive disease (PAOD). In RA, we did not find any correlation between ADMA or hArg and thCys at baseline (n = 100) and after (n = 83) combined add-on supplementation of omega-3 fatty acids, vitamin E, vitamin A, copper, and selenium, or placebo (soy oil). ADMA correlated with Arg at baseline (r = 0.446, P < 0.001) and after treatment (r = 0.246, P = 0.03). hArg did not correlate with ADMA, but correlated with Arg before (r = 0.240, P = 0.02) and after treatment (r = 0.233, P = 0.03). These results suggest that hArg, ADMA and Arg are biochemically familiar with each other, but unrelated to hCys in RA. In PAOD and CAD, ADMA and thCys did not correlate.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
In humans, l-homoarginine (hArg) and l-homocysteine (hCys) are non-essential, non-proteinogenic amino acids, homologues of l-arginine (Arg) and l-cysteine (Cys), respectively. In their chemical structures, hArg and hCys differ from Arg and Cys each by a methylene (CH2, 14 Da) group. Arg plays an important role in metabolism and nutrition in growth, health and disease (Wu et al. 2009). Thus, Arg is the substrate of nitric oxide synthase (NOS) isoforms which catalyse the conversion of Arg to nitric oxide (NO) and l-citrulline (Tsikas 2008). NO possesses various biological activities including inhibition of vascular inflammation and platelet aggregation, prevention of adhesion of immune cells and vasodilatation (Moncada and Higgs 1993; Leiper and Vallance 1999). hArg may serve both as a substrate for NOS and as an inhibitor of NOS activity (Moali et al. 1998 and 2000; Bretscher et al. 2003). Asymmetric dimethylarginine (ADMA) is an endogenous inhibitor of NOS activity (Tsikas et al. 2000). Elevated circulating ADMA concentrations are generally considered a cardiovascular risk factor (Horowitz and Heresztyn 2007; Böger et al. 2009). Mean plasma and serum hArg concentrations in healthy subjects are of the order of 2 µM (Kayacelebi et al. 2014a). Low circulating hArg concentrations were found to be associated with cardiovascular and all-cause mortality in patients (März et al. 2010; Pilz et al. 2011; Drechsler et al. 2011; Choe et al. 2013). Low plasma hArg concentrations were also found in patients suffering from Takotsubo cardiomyopathy (Kayacelebi et al. 2014b). Furthermore, lower hArg concentrations were measured in plasma of male smokers compared to male non-smokers, while ADMA plasma concentrations were higher in smokers compared to non-smokers (Sobczak et al. 2014). This diametric change may suggest that hArg and ADMA could act antagonistically in the cardiovascular system (Tsikas and Kayacelebi 2014). Observations from our and other groups are supportive of an antagonism between hArg and ADMA in rheumatoid arthritis (Kayacelebi et al. 2014c) and in preeclampsia (Valtonen et al. 2008; Khalil et al. 2013). In these conditions, circulating hArg concentrations are rather elevated.
Although the biosynthesis of hArg has been investigated several decades ago (Ryan and Wells 1964; Ryan et al. 1969), both biosynthesis and biological activities of hArg in humans are incompletely understood. Recent studies indicate that l-arginine:glycine amidinotransferase (AGAT; EC 2.1.4.1) plays a pivotal role in hArg biosynthesis (Davids et al. 2012, Choe et al. 2013). Increased AGAT expression was found to be associated with increased hArg synthesis in vitro (Choe et al. 2013). Yet, the underlying biochemical mechanism of AGAT-catalysed synthesis of hArg remains still elusive.
S-adenosylmethionine (SAM) is the common methyl (CH3) donor in many enzymatic pathways that produce a variety of methyl groups-containing biomolecules, including ADMA, hCys and creatine. Interrelationships between Arg, hArg, ADMA and hCys are expectable because of partial biochemical overlap, and their determination may contribute to delineate the underlying mechanisms. While the relationship between circulating ADMA and hCys has been often investigated in the past, though with diverging results, we are not aware of studies investigating the relationship between circulating hArg and hCys in health and disease. With respect to circulating ADMA and hCys, these compounds were found to correlate in healthy and sick subjects both before and after oral administration (100 mg/kg body weight) of methionine, the precursor of SAM (Stühlinger et al. 2003). In elderly patients with stroke, a moderate correlation (r = 0.43, P = 0.01) between ADMA and hCys was reported (Yoo and Lee 2001). In 145 patients with coronary artery disease (CAD), plasma ADMA and hCys were found to correlate weakly (r = 0.25, P < 0.05) (Wang et al. 2006). In contrast, other groups found that hCys and ADMA did not correlate in normo- and hyperhomocysteinaemic subjects (Paroni et al. 2005; Antoniades et al. 2006).
As before (Wanby et al. 2003), there is currently no clear evidence to support the supposition that methionine-induced hyperhomocysteinaemia may be accompanied by elevated levels of ADMA. Thus, in healthy human subjects oral administration of methionine (0.1 g/kg) or hCys (0.01 g/kg) disproved endothelial function (assessed by measuring flow-mediated dilatation), but did not increase circulating ADMA concentration (Doshi et al. 2005). This observation suggests that methionine- or hCys-induced endothelial dysfunction may not be due to ADMA or due to disruption of the methylation status. Thus far, there is only a single study reporting on a weak correlation (r = 0.229, P = 0.012) between circulating ADMA and hCys in systemic lupus erythematosus (Perna et al. 2010), a rheumatic disease.
The emerging importance of hArg as a novel risk factor of cardiovascular diseases (März et al. 2010) prompted us to investigate possible associations between hArg and the two established cardiovascular risk factors hCys and ADMA. We chose rheumatoid arthritis (RA), because RA and other systemic rheumatic diseases are associated with increased cardiovascular disease (CVD)-related mortality (Lévy et al. 2008). Thus, the risk of heart failure in RA is almost twice that of the general population. In RA, total hCys concentration is higher compared to healthy subjects (Roubenoff et al. 1997). However, we recently showed that the increased risk in RA cannot be entirely explained by traditional cardiovascular risk factors (Willers and Hahn 2012). It is more likely that the increased risk for CVD in RA is related to inflammation and immune-mediated processes (Crowson et al. 2005; Willers and Hahn 2012; Wright et al. 2014). In RA, ADMA is assumed to play a particular, yet not fully understood role (Dimitroulas et al. 2012, 2013; Surdacki et al. 2007). Inhibition of NO synthesis by ADMA (Tsikas et al. 2000) may be one possible explanation for ADMA’s involvement in CVD. However, in a large cohort of RA patients, ADMA was found not to be associated with subendocardial viability ratio, a surrogate marker of coronary microvascular perfusion (Dimitroulas et al. 2014).
In the present work, we investigated potential associations between circulating concentrations of hArg, Arg, ADMA and thCys in patients suffering from RA. As the hArg-to-ADMA (hArg/ADMA) molar ratio in the circulation may better evaluate the relative effects of hArg and ADMA on CVD (Tsikas and Kayacelebi 2014), we included this parameter in our analyses. The relationship between the plasma concentrations of ADMA and thCys was also investigated in elderly patients suffering from peripheral arterial occlusive disease (PAOD) or coronary artery disease (CAD).
Materials and methods
Rheumatoid arthritis study
Plasma samples of 100 RA patients (88 females, 12 males) were collected in a previously reported placebo-controlled study (Willers et al. 2011). The study involved a placebo group and a verum group. In the placebo group, RA patients took soy oil. The RA patients of the verum group received a combined add-on supplementation for 12 weeks of omega-3 fatty acids, vitamins E and A, copper and selenium. The plasma hArg, Arg and ADMA concentrations of the RA patients were reported recently (Kayacelebi et al. 2014c). Plasma concentrations of hArg (Kayacelebi et al. 2014a) and ADMA (Tsikas et al. 2003) were measured by GC–MS/MS. Plasma Arg concentration was determined by GC–MS (Tsikas et al. 2003). In the samples of these studies, we measured plasma total hCys (thCys) by an enzyme-based assay from AXIS-Shield Diagnostics (Dundee, Scotland). The previously measured plasma hArg, Arg and ADMA concentrations were correlated with the newly determined plasma thCys concentrations. Written informed consent was provided by all subjects included in the study. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the Freiburg Ethics Committee International (Freiburg, Germany) and by the Ethics Committee of Charité-University of Medicine (Berlin, Germany).
PAOD and CAD studies
Blood (9 mL) was donated by 40 PAOD patients (31 males, 9 females; mean age 68 years) and 60 CAD patients (48 males, 12 females; mean age 62 years). After immediate blood centrifugation (2000×g, 5 min), EDTA plasma samples were separated and stored at −80 °C until analysis. Both studies were approved by the Ethics Committee of the Hannover Medical School. In these studies, plasma thCys, ADMA and Arg were measured by GC–MS/MS (Tsikas et al. 2003). hArg was not analysed in the plasma samples of these studies, because at the time of thCys, ADMA and Arg analysis no method was available for hArg in our group.
Statistical analysis and data presentation
Statistical analyses were performed and graphs were constructed by Origin 7.5G and GraphPad Prism 5.04. The concentrations of the biochemical parameters measured in the studies were found to be non-normally distributed. Therefore, nonparametric correlation (Spearman) between two parameters was performed, and statistical significance was tested by the nonparametric Mann–Whitney t test. A P value ≤0.05 was considered significant. Data are presented as mean ± SEM.
Results
Rheumatoid arthritis study
This is the first study to investigate potential interrelationships between circulating hArg, Arg, ADMA and thCys in patients suffering from RA. The results of the study are shown in Fig. 1 and the correlations are summarised in Table 1.

Relationship between the plasma concentration of hArg and ADMA or the plasma hArg/ADMA molar ratio and plasma total hCys (thCys) in patients with rheumatoid arthritis before (a) and after (b) a 12-week supplementation with placebo or omega-3 fatty acids, vitamins E and A, copper and selenium. As neither placebo nor verum changed significantly the plasma concentration of hArg, ADMA and thCys, the combined data are presented here for the whole population. Note the logarithmic scale on the y axis
There were no differences between the placebo and verum groups with respect to hArg, ADMA and Arg (Kayacelebi et al. 2014c). With respect to thCys, there were also no differences between placebo and verum groups. We therefore combined the thCys concentration data from the placebo and verum groups to a single group. Plasma thCys was found not to differ (P = 0.3534) between baseline (n = 100) and after 12 weeks (n = 83) treatment (12.4 ± 0.46 vs. 11.9 ± 0.51 µM) in the RA patients.
There was no correlation between thCys and the plasma concentration of hArg or ADMA; the plasma hArg/ADMA molar ratio also did not correlate with plasma thCys concentration (Table 1; Fig. 1). There was a correlation between the hArg or ADMA and Arg plasma concentrations in both groups before and after the 12 weeks treatment (Table 1; Fig. 1). Treatment (placebo or verum) seems to have attenuated the correlation between ADMA and Arg, but not the correlation between hArg and Arg (Table 1).
PAOD and CAD studies
In the PAOD study, the plasma concentrations of ADMA (n = 39), thCys (n = 40) and Arg (n = 40) were 529 ± 18 nM, 7.48 ± 0.77 and 56.5 ± 2.71 µM, respectively. There was a borderline correlation (r = 0.31, P = 0.055, n = 39) between plasma thCys and ADMA concentrations. The correlation between ADMA and Arg plasma concentrations was much stronger (r = 0.511, P = 0.0009, n = 39). thCys and Arg did not correlate (r = 0.237, P = 0.141, n = 40).
In the CAD study, the plasma concentrations of ADMA (n = 39), thCys (n = 40) and Arg (n = 40) were 505 ± 16 nM, 9.76 ± 0.41 and 72.2 ± 23.3 µM, respectively. There was no correlation between plasma thCys or ADMA (r = 0.17, P = 0.188, n = 40) and Arg (r = 0.17, P = 0.195, n = 39) concentrations, whereas plasma ADMA and Arg correlated with each other (r = 0.375, P = 0.003, n = 39).
Discussion
This is the first study to investigate the relationship between the newly emerged cardiovascular risk factor hArg and the long-established cardiovascular risk factors hCys and ADMA in plasma of patients suffering from rheumatoid arthritis (RA). On the basis of the concentrations of the analytes measured in the plasma samples, there is no relationship between hArg and thCys or between ADMA and thCys in RA. The literature data available for ADMA and thCys (Yoo and Lee 2001; Stühlinger et al. 2003; Wanby et al. 2003; Paroni et al. 2005; Antoniades et al. 2006; Wang et al. 2006) and our present observations in RA, PAOD and CAD argue against an unequivocal relationship between circulating concentrations of ADMA and thCys in health and disease. The second interesting finding of the present study is that the plasma concentrations of hArg and ADMA did not correlate with each other in RA. However, in our RA patients circulating hArg and ADMA correlated with the plasma concentration of Arg, i.e., their common precursor, confirming data reported by other groups for healthy and ill subjects (Jaźwińska-Kozuba et al. 2013; Khalil et al. 2013; van der Zwan et al. 2013). In PAOD and CAD, plasma thCys and ADMA also did not correlate with each other. Like in RA, in PAOD and in CAD, plasma ADMA and Arg were correlated. Taking all data together, it seems that hArg, ADMA and Arg are much closely related among themselves than with thCys.
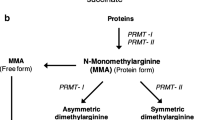
An explanation for lacking correlation between thCys and hArg, ADMA or Arg could be the large number of pathways in which Arg and the methyl donor SAM are involved. Estimates indicate that in young male adults, creatine synthesis rate is about 8 mmol per day, whereas the transmethylation flux is about two to three times higher (Mudd et al. 2007; Brosnan et al. 2011). Thus, the greatest part of daily produced SAM is utilised in the synthesis of creatine. In humans, methylation of the guanidine group (N G) of Arg residues in proteins is catalysed by protein arginine methyltransferases (PRMTs; Leiper and Vallance 1999), and this reaction is considered to be the sole source of ADMA. The major fraction of daily produced ADMA (about 90 %) is hydrolysed to dimethylamine (DMA) which is excreted in the urine. Healthy humans excrete about 10 mmol dimethylamine (DMA) per 1 mol creatinine (Tsikas et al. 2007). This rough calculation suggests that the guanidinoacetate methyltransferase (GAMT)-catalysed synthesis of creatine utilises approximately 100 times more SAM than the PRMT-catalysed synthesis of ADMA in healthy humans (Fig. 2). In a previous study, we found that patients with RA and spondyloarthritis (SA) excrete about 45 and 80 mmol DMA per 1 mol creatinine (Chobanyan-Jürgens et al. 2011), respectively. These observations suggest that in RA and SA about four to eight times more SAM is utilised compared to healthy subjects. In the RA patients of the present study, we determined an excretion rate of 58.1 ± 3.41 mmol DMA/mol creatinine at baseline (n = 39) and 58.7 ± 3.94 mmol DMA/mol creatinine after 12 weeks (n = 33) when combining placebo and verum groups. This is close to the DMA excretion rate of 60 ± 12 mmol DMA/mol creatinine measured in another cohort of 28 patients with rheumatic diseases including RA (Chobanyan-Jürgens et al. 2011). Similar excretion rates of DMA (53 ± 2.65 mmol DMA/mol creatinine, n = 49) were also observed in patients suffering from CAD (Tsikas et al. 2007). Thus, although patients suffering from RA, PAOD or CAD utilise several times more SAM than healthy subjects to produce ADMA, hCys synthesis seems to be independent of ADMA synthesis in these diseases.

S-adenosylmethionine (SAM) is the common methyl ([CH3]) donor in many enzymatic pathways leading to ADMA, hArg and hCys. Left panel Arginine residues in proteins are methylated on the guanidine group (N G) by protein arginine methyltransferases (PRMTs). For the sake of simplicity the free amino acid l-Arg is shown. Arginine:glycine amidinotransferase (AGAT) catalyses the formation of guanidinoacetate (GAA) from l-Arg and glycine (Gly). GAA is methylated by guanidinoacetate methyltransferase (GAMT) to form creatine. AGAT also catalyses the formation of l-homoarginine (hArg) from l-Arg and l-lysine. Right panel S-Adenosylhomocysteine (SAhCys) derived from SAM is hydrolysed by SAhCys hydrolase (SAH) to l-homocysteine (hCys) and adenosine. Note that the creatine biosynthesis pathway generates 20–100 times more hCys than the ADMA biosynthesis pathway in humans (roughly indicated by the arrow width on the right panel). See the text for more information
The GAMT-catalysed synthesis of creatine from guanidinoacetate (GAA) is presumably the most abundant SAM-consuming reaction in transmethylation reactions (Fig. 2). Because creatinine synthesis utilises 20–100 times more SAM than the ADMA synthesis from Arg in proteins by PRMTs, correlation between circulating thCys and ADMA is likely to fail in clinical studies, especially when performed on small populations. Arg is the substrate of AGAT which catalyses the formation of hArg and GAA, with the latter being methylated to creatinine by GAMT (Fig. 2). Because the formation rate of creatine is much higher than that of hArg, lack of an expected correlation between hArg and hCys appears plausible. Despite the lack of a correlation between circulating hArg and hCys observed in our RA patients, pharmacological and/or dietary intervention to lower thCys, such as high-dose vitamin supplementation, may be hazardous. Lowering hCys synthesis may be associated with inhibition of hArg biosynthesis, even if this is not seen in circulating concentrations of thCys and hArg. As low circulating hArg concentrations are associated with cardiovascular and all-cause mortality in patients suffering from cardiovascular diseases (März et al. 2010; Pilz et al. 2011; Drechsler et al. 2011; Choe et al. 2013), lowering plasma thCys concentration may potentially cause severe adverse effects in the renal and cardiovascular systems (Giustarini et al. 2009). It is noteworthy that treatment of high-risk patients with folic acid, vitamin B12 and vitamin B6 lowered thCys, but did not reduce the cardiovascular risk (Lonn et al. 2006). Measurement of circulating hArg in addition to ADMA in patients with cardiovascular diseases is recommended. As hCys formation from SAM requires catalysis by SAM hydrolase (SAH), measurement of activity and expression of this enzyme may provide additional useful information about formation and mode of biological action of hArg and ADMA.
In conclusion, in RA circulating concentrations of hArg, thCys, ADMA and Arg are rather normal. The biochemical relationship among plasma Arg and ADMA concentrations is more profound than between each of these biochemical parameters and hArg or thCys. Investigations of potential interrelationships between hArg and thCys in healthy subjects and patients suffering from different diseases are warranted. They are likely to contribute to delineating the enigmatic roles of hArg and thCys in physiology and pathology.
Abbreviations
- ADMA:
-
Asymmetric dimethylarginine (N G,N G-dimethyl-l-arginine)
- AGAT:
-
Arginine:glycine amidinotransferase
- CAD:
-
Coronary artery disease
- GAMT:
-
Guanidinoacetate methyltransferase
- GC–MS:
-
Gas chromatography–mass spectrometry
- GC–MS/MS:
-
Gas chromatography–tandem mass spectrometry
- hArg:
-
Homoarginine
- hCys/thCys:
-
Homocysteine/total homocysteine
- NO:
-
Nitric oxide
- NOS:
-
Nitric oxide synthase
- PAOD:
-
Peripheral arterial occlusive disease
- RA:
-
Rheumatoid arthritis
- SAH:
-
S-Adenosylhomocysteine hydrolase
- SAM:
-
S-adenosylmethionine
References
Antoniades C, Tousoulis D, Marinou K, Vasiliadou C, Tentolouris C, Bouras G, Pitsavos C, Stefanadis C (2006) Asymmetrical dimethylarginine regulates endothelial function in methionine-induced but not in chronic homocystinemia in humans: effect of oxidative stress and proinflammatory cytokines. Am J Clin Nutr 84:781–788
Böger RH, Maas R, Schulze F, Schwedhelm E (2009) Asymmetric dimethylarginine (ADMA) as a prospective marker of cardiovascular disease and mortality—an update on patient populations with a wide range of cardiovascular risk. Pharmacol Res 60:481–487
Bretscher LE, Li H, Poulos TL, Griffith OW (2003) Structural characterization and kinetics of nitric-oxide synthase inhibition by novel N5-(iminoalkyl)- and N5-(iminoalkenyl)-ornithines. J Biol Chem 278:46789–46797
Brosnan JT, da Silva RP, Brosnan ME (2011) The metabolic burden of creatine synthesis. Amino Acids 40:1325–1331
Chobanyan-Jürgens K, Pham VV, Stichtenoth DO, Tsikas D (2011) Elevated dimethylarginine dimethylaminohydrolase (DDAH) activity in rheumatoid arthritis and spondyloarthritis. Nitric Oxide 25:436–438
Choe CU, Atzler D, Wild PS, Carter AM, Böger RH, Ojeda F, Simova O, Stockebrand M, Lackner K, Nabuurs C, Marescau B, Streichert T, Muller C, Luneburg N, De Deyn PP, Benndorf RA, Baldus S, Gerloff C, Blankenberg S, Heerschap A, Grant PJ, Magnus T, Zeller T, Isbrandt D, Schwedhelm E (2013) Homoarginine levels are regulated by l-arginine:glycine amidinotransferase and affect stroke outcome: results from human and murine studies. Circulation 128:1451–1461
Crowson CS, Nicola PJ, Kremers HM, O’Fallon WM, Therneau TM, Jacobsen SJ, Roger VL, Ballman KV, Gabriel SE (2005) How much of the increased incidence of heart failure in rheumatoid arthritis is attributable to traditional cardiovascular risk factors and ischemic heart disease? Arthritis Rheum 52:3039–3044
Davids M, Ndika JD, Salomons GS, Blom HJ, Teerlink T (2012) Promiscuous activity of arginine:glycine amidinotransferase is responsible for the synthesis of the novel cardiovascular risk factor homoarginine. FEBS Lett 586:3653–3657
Dimitroulas T, Sandoo A, Kitas GD (2012) Asymmetric dimethylarginine as a surrogate marker of endothelial dysfunction and cardiovascular risk in patients with systemic rheumatic diseases. Int J Mol Sci 13:12315–12335
Dimitroulas T, Sandoo A, van Veldhuijzen JJZ et al (2013) Predictors of asymmetric dimethylarginine levels in patients with rheumatoid arthritis: the role of insulin resistance. Scand J Rheumatol 42:176–181
Dimitroulas T, Sandoo A, Smith JP, Kitas GD (2014) Asymmetric dimethylarginine is not associated with subendocardial viability ratio in rheumatoid arthritis. Int J Cardiol 172:285–286
Doshi S, McDowell I, Goodfellow J, Stabler S, Boger R, Allen R, Newcombe R, Lewis M, Moat S (2005) Relationship between S-adenosylmethionine, S-adenosylhomocysteine, asymmetric dimethylarginine, and endothelial function in healthy human subjects during experimental hyper- and hypohomocysteinemia. Metabolism 54(3):351–360
Drechsler C, Meinitzer A, Pilz S, Krane V, Tomaschitz A, Ritz E, März W, Wanner C (2011) Homoarginine, heart failure, and sudden cardiac death in haemodialysis patients. Eur J Heart Fail 13:852–859
Giustarini D, Dalle-Donne I, Tsikas D, Rossi R (2009) Oxidative stress and human diseases: origin, link, measurement, mechanisms, and biomarkers. Crit Rev Clin Lab Sci 46:241–281
Horowitz JD, Heresztyn T (2007) An overview of plasma concentrations of asymmetric dimethylarginine (ADMA) in health and disease and in clinical studies: methodological considerations. J Chromatogr B 851:42–50
Jaźwińska-Kozuba A, Martens-Lobenhoffer J, Kruszelnicka O, Rycaj J, Chyrchel B, Surdacki A, Bode-Böger SM (2013) Opposite associations of plasma homoarginine and ornithine with arginine in healthy children and adolescents. Int J Mol Sci 14:21819–21832
Kayacelebi AA, Beckmann B, Gutzki FM, Jordan J, Tsikas D (2014a) GC-MS and GC-MS/MS measurement of the cardiovascular risk factor homoarginine in biological samples. Amino Acids 46:2205–2217
Kayacelebi AA, Nguyen TH, Neil C, Horowitz JD, Jordan J, Tsikas D (2014b) Homoarginine and 3-nitrotyrosine in patients with takotsubo cardiomyopathy. Int J Cardiol 173:546–547
Kayacelebi AA, Pham VV, Willers J, Hahn A, Stichtenoth DO, Jordan J, Tsikas D (2014c) Plasma homoarginine (hArg) and asymmetric dimethylarginine (ADMA) in patients with rheumatoid arthritis: is homoarginine a cardiovascular corrective in rheumatoid arthritis, an anti-ADMA? Int J Cardiol 176:1129–1131
Khalil AA, Tsikas D, Akolekar R, Jordan J, Nicolaides KH (2013) Asymmetric dimethylarginine, arginine and homoarginine at 11–13 weeks’ gestation and preeclampsia: a case-control study. J Hum Hypertens 27:38–43
Leiper J, Vallance P (1999) Biological significance of endogenous methylarginines that inhibit nitric oxide synthases. Cardiovasc Res 43:542–548
Lévy L, Fautrel B, Barnetche T, Schaeverbeke T (2008) Incidence and risk of fatal myocardial infarction and stroke events in rheumatoid arthritis patients. A systematic review of the literature. Clin Exp Rheumatol 26:673–679
Lonn E, Yusuf S, Arnold MJ, Sheridan P, Pogue J, Micks M, McQueen MJ, Probstfield J, Fodor G, Held C, Genest J (2006) Heart outcomes prevention evaluation (HOPE) 2 investigators homocysteine lowering with folic acid and B vitamins in vascular disease. N Engl J Med 354: 1567–1577
März W, Meinitzer A, Drechsler C, Pilz S, Krane V, Kleber ME, Fischer J, Winkelmann BR, Böhm BO, Ritz E, Wanner C (2010) Homoarginine, cardiovascular risk, and mortality. Circulation 122:967–975
Moali C, Boucher JL, Sari MA, Stuehr DJ, Mansuy D (1998) Substrate specificity of NO synthases: detailed comparison of l-arginine, homo-l-arginine, their N omega-hydroxy derivatives, and N omega-hydroxynor-l-arginine. Biochemistry 37:10453–10460
Moali C, Brollo M, Custot J, Sari MA, Boucher JL, Stuehr DJ, Mansuy D (2000) Recognition of alpha-amino acids bearing various C = NOH functions by nitric oxide synthase and arginase involves very different structural determinants. Biochemistry 39:8208–8218
Moncada S, Higgs A (1993) The l-arginine-nitric oxide pathway. New Engl J Med 329:2002–2012
Mudd SH, Brosnan JT, Brosnan ME, Jacobs RL, Stabler SP, Allen RH, Vance DE, Wagner C (2007) Methyl balance and transmethylation fluxes in humans. Am J Clin Nutr 85:19–25
Paroni R, Fermo I, Fiorina P, Cighetti G (2005) Determination of asymmetric and symmetric dimethylarginines in plasma of hyperhomocysteinemic subjects. Amino Acids 28(4):389–394
Perna M, Roman MJ, Alpert DR, Crow MK, Lockshin MD, Sammaritano L, Devereux RB, Cooke JP, Salmon JE (2010) Relationship of asymmetric dimethylarginine and homocysteine to vascular aging in systemic lupus erythematosus patients. Arthritis Rheum 2010(62):1718–1722
Pilz S, Tomaschitz A, Meinitzer A, Drechsler C, Ritz E, Krane V, Wanner C, Bohm BO, März W (2011) Low serum homoarginine is a novel risk factor for fatal strokes in patients undergoing coronary angiography. Stroke 42:1132–1134
Roubenoff R, Dellaripa P, Nadeau MR, Abad LW, Muldoon BA, Selhub J, Rosenberg IH (1997) Abnormal homocysteine metabolism in rheumatoid arthritis. Arthritis Rheum 40:718–722
Ryan WL, Wells IC (1964) Homocitrulline and homoarginine synthesis from lysine. Science 144:1122–1127
Ryan WL, Johnson RJ, Dimari S (1969) Homoarginine synthesis by rat kidney. Arch Biochem Biophys 131:521–526
Sobczak A, Prokopowicz A, Radek M, Szula M, Zaciera M, Kurek J, Goniewicz ML (2014) Tobacco smoking decreases plasma concentration of the emerging cardiovascular risk marker, l-homoarginine. Circ J 78:1254–1258
Stühlinger MC, Oka RK, Graf EE, Schmölzer I, Upson BM, Kapoor O, Szuba A, Malinow MR, Wascher TC, Pachinger O, Cooke JP (2003) Endothelial dysfunction induced by hyperhomocyst(e)inemia: role of asymmetric dimethylarginine. Circulation 108:933–938
Surdacki A, Martens-Lobenhoffer J, Wloch A et al (2007) Elevated plasma asymmetric dimethyl-l-arginine levels are linked to endothelial progenitor cell depletion and carotid atherosclerosis in rheumatoid arthritis. Arthritis Rheum 56:809–819
Tsikas D (2008) A critical review and discussion of analytical methods in the l-arginine/nitric oxide area of basic and clinical research. Anal Biochem 379:139–163
Tsikas D, Kayacelebi AA (2014) Do homoarginine and asymmetric dimethylarginine act antagonistically in the cardiovascular system? Circ J 78:2094–2095
Tsikas D, Böger RH, Sandmann J, Bode-Böger SM, Frölich JC (2000) Endogenous nitric oxide synthase inhibitors are responsible for the l-arginine paradox. FEBS Lett 478:1–3
Tsikas D, Schubert B, Gutzki FM, Sandmann J, Frölich JC (2003) Quantitative determination of circulating and urinary asymmetric dimethylarginine (ADMA) in humans by gas chromatography-tandem mass spectrometry as methyl ester tri(N-pentafluoropropionyl) derivative. J Chromatogr B 798:87–99
Tsikas D, Thum T, Becker T, Pham VV, Chobanyan K, Mitschke A, Beckmann B, Gutzki FM, Bauersachs J, Stichtenoth DO (2007) Accurate quantification of dimethylamine (DMA) in human urine by gas chromatography-mass spectrometry as pentafluorobenzamide derivative: evaluation of the relationship between DMA and its precursor asymmetric dimethylarginine (ADMA) in health and disease. J Chromatogr B 851:229–239
Valtonen P, Laitinen T, Lyyra-Laitinen T, Raitakari OT, Juonala M, Viikari JS, Heiskanen N, Vanninen E, Punnonen K, Heinonen S (2008) Serum l-homoarginine concentration is elevated during normal pregnancy and is related to flow-mediated vasodilatation. Circ J 72:1879–1884
van der Zwan LP, Davids M, Scheffer PG, Dekker JM, Stehouver CDA, Teerlink T (2013) l-Homoarginine and arginine are antagonistically related to blood pressure in an elderly population: the Hoorn study. J Hypertens 31:1114–1123
Wanby P, Brattström L, Brudin L, Hultberg B, Teerlink T (2003) Asymmetric dimethylarginine and total homocysteine in plasma after oral methionine loading. Scand J Clin Lab Invest 63:347–353
Wang J, Sim AS, Wang XL, Salonikas C, Naidoo D, Wilcken DE (2006) Relations between plasma asymmetric dimethylarginine (ADMA) and risk factors for coronary disease. Atherosclerosis 184:383–388
Willers J, Hahn A (2012) Cardiovascular risk in patients with rheumatoid arthritis: assessment of several traditional risk parameters and of a German risk score model. Rheumatol Int 32:3741–3749
Willers J, Fasse S, Putschky N et al (2011) Combined add-on supplementation of omega-3 fatty acids, vitamin E, vitamin A, copper, and selenium in rheumatoid arthritis. Food Nutr Sci 2:714–723
Wright K, Crowson CS, Gabriel SE (2014) Cardiovascular comorbidity in rheumatic diseases: a focus on heart failure. Heart Fail Clin 10:339–352
Wu G, Bazer FW, Davis TA, Kim SW, Li P, Marc Rhoads J, Carey Satterfield M, Smith SB, Spencer TE, Yin Y (2009) Arginine metabolism and nutrition in growth, health and disease. Amino Acids 37:153–168
Yoo JH, Lee SC (2001) Elevated levels of plasma homocyst(e)ine and asymmetric dimethylarginine in elderly patients with stroke. Atherosclerosis 158:425–430
Acknowledgments
The authors are thankful to Bibiana Beckmann for excellent laboratory assistance.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kayacelebi, A.A., Willers, J., Pham, V.V. et al. Plasma homoarginine, arginine, asymmetric dimethylarginine and total homocysteine interrelationships in rheumatoid arthritis, coronary artery disease and peripheral artery occlusion disease. Amino Acids 47, 1885–1891 (2015). https://doi.org/10.1007/s00726-015-1915-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00726-015-1915-3