
Abstract
Imaginary tasks can be used to investigate the neurophysiology of gait. In this study, we explored the cortical control of gait-related imagery in 21 healthy volunteers using functional magnetic resonance imaging. Imaginary tasks included gait initiation, stepping over an obstacle, and gait termination. Subjects watched a video clip that showed an actor in gait motion under an event-related design. We detected activation in the supplementary motor area during major gait-related imagery tasks, and especially during gait initiation. During gait termination and stepping over an obstacle, the amount of cortical resources allocated to the imaginary tasks included a large visuomotor network comprising the dorsal and ventral premotor areas. We conclude that our paradigm to study the cortical control of gait may help in elucidating the pathophysiology of higher-level gait disorders.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Gait has been considered in the past decades only as an automatic process involving little or no higher cortical input. Apparently, central pattern generators (Grillner and Wallen 1985) can create gait utilizing little, if any, cortical resources. Growing evidence, however, suggests that this view may be too simplistic. The motor cortex and the pyramidal tract act as supraspinal inputs and play a key role not only in initiating locomotion but also in adapting the locomotor pattern to environmental and motivational conditions (Armstrong 1988; MacKay-Lyons 2002). In addition, clinical evidence indicates that various gait disorders should be ascribed to cerebral cortical lesions. In this regard, gait ignition failure may be caused by lesions in the supplementary motor area (Della Sala et al. 2002; Nadeau 2007). Automatic obstacle avoidance has been suggested to be a function of the dorsal stream of visual processing (McIntosh et al. 2004; Rice et al. 2006; Schindler et al. 2004).
Non-invasive imaging studies of the cortical involvement in gait control using functional magnetic resonance imaging (fMRI) have been limited in humans. The apparent incapability to walk inside an MR scanner represents a limitation for this kind of study. It has been suggested, however, that activation maps during movement execution are similar to those observed during the imagery of the same task (Jeannerod 2001; Munzert et al. 2009). Accordingly, imagined locomotion in functional magnetic resonance imaging has been proposed as a novel paradigm to study brain activation during motor tasks (Bakker et al. (2007a). In this context, several studies have focused on the behavioral and cerebral correlates of motor imagery, as well as the relationships with actual execution and motor planning (Jeannerod 2006).
Many efforts have been made to study the cortical control of gait using 18F-fluorodexoyglucose positron emission tomography (FDG-PET) and fMRI coupled with imaginary tasks (Bakker et al. 2007b; Malouin et al. 2003). The basic mental process of the imagination can vary widely across different subjects (Sirigu and Duhamel 2001). Mirror neurons are a particular class of visuomotor neurons that discharge when an individual performs a particular action but also when he/she observes the same behavior in another individual (Buccino et al. 2001; Rizzolatti and Craighero 2004). To minimize the interindividual differences in motor imagery, specific paradigms have been proposed. We have previously shown that gait-related activities incorporate the mental process of action observation and motor imagery (Wang et al. 2008a, b). The model was based on shared motor representations, which assumed a functional equivalence between intending, imagining, observing, and performing an action (Grezes and Decety 2001; Iseki et al. 2008).
Recent years have witnessed tremendous progress in the understanding of the corticol control of human walking due to advances in functional neuroimaging, electrophysiology, and optical imaging (Bakker et al. (2007b). However, many studies have been limited to a block paradigm design. Additionally, some reports have not examined the various components of gait separately. Other research has used PET (Malouin et al. 2003), optical imaging (Suzuki et al. 2008), and EEG (Yazawa et al. 1997) to investigate brain activation during the imagination of different gait-related tasks. However, a major advantage of fMRI over other techniques is the high spatial resolution that permits the identification of cortical areas that are active during a particular cognitive process. In this study, we explored the cortical control of gait-related imagery in 21 healthy volunteers using fMRI. Imaginary tasks included gait initiation, stepping over an obstacle, and gait termination.
Methods and materials
The study was approved by the institutional review board of the ChangGung Memorial Hospital and complied with the ethical standards established in the Declaration of Helsinki. The experiments were undertaken with the understanding and written consent of each subject. A total of 21 healthy right-handed gender-balanced volunteers (mean age, 21.5 ± 1.2 years; range, 20–25 years) were recruited to the study. The identity of participants was carefully preserved.
fMRI scanning
The experiments were conducted at the ChangGung Memorial Hospital using a 1.5-T MRI scanner (Intera, Philips, Best, Holland). Subjects viewed the stimuli via a mirror system. Contact lenses were used to correct visual acuity during the scans. The participants had their head movements restrained by a plastic fixation pad. MP-RAGE sequences yielding T1-weighted images were used as reference. Imaging parameters were TR/TE/flip angle = 9 ms/4.2 ms/90°. One hundred and eighty sagittal slices were acquired to cover the whole brain. Reconstructed images had spatial resolution of 0.86 mm × 0.86 mm × 1.0 mm. The BOLD sequence used a single-shot T2*-weighted GE-EPI sequence. Twenty-two slices were acquired with a slice thickness of 5 mm to cover the whole brain. Other imaging parameters were as follows: TR/TE/flip angle = 2,500 ms/50 ms/90°, matrix size = 128 × 128, FOV = 192 mm, in-plane resolution = 1.5 mm × 1.5 mm.
Paradigm design
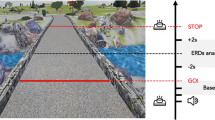
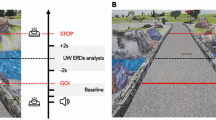
Ten fMRI sessions with an event-related design were conducted. Each session comprised three pseudorandomized blocks. Before the experiment, the paradigm was presented to the subjects for approximately 30 min when outside the scanner. Throughout the experiments, subjects were asked to identify themselves as the actor and to mentally imitate the movements viewed in the clips. Each block consisted of a video clip that showed an actor firstly standing and then walking in an egocentric perspective. During the standing position, the video clip showed an actor while standing upright without any movement. The actor subsequently walked over an obstacle lying on the floor and carefully stepped over it. Thereafter, the subject continued to walk, and then stopped and stood still. Each stimulus began and ended with the person standing in an egocentric view, and was separated by a fixed cross. Each stimulus lasted 16–18 s, with a 2–4 s interval for separation. All experiments were designed in order to obtain counterbalanced conditions, with a total session duration of 220 s. Figure 1 presents a graphical representation of the paradigm.

Graphical representation of the paradigm, including stills of different experimental stimuli. The durations of the WALK and STAND conditions varied between 16 and 18 s. The duration of the fixed cross was randomized between 2 and 4 s
fMRI data analysis
The fMRI data were analyzed using the SPM5 software (The Wellcome Trust Centre for Neuroimaging, London, UK) running under MATLAB 7.0 (MathWorks, Inc., Natick, MA, USA). The first two scans of EPI series were excluded to minimize T1 relaxation artifacts. Functional data were corrected for motion via sinc interpolation. The realigned images were then normalized into the standard SPM/MNI template and thus transformed into a standard stereotaxic space and resampled with a resolution of 2 mm × 2 mm × 2 mm. A Gaussian filter of 8-mm full width at half maximum (FWHM) was then applied to accommodate for anatomical variability across subjects, as well as to satisfy the assumptions of Gaussian field theory (Worsley et al. 1996). The data were then high-pass filtered with a cut-off period of 128 s to remove low frequency drifts in the BOLD signals. The hemodynamic response function was used to identify the activated voxels.
The subject-level statistical analyses were performed using the general linear model (GLM) for event-related designs. Linear contrasts of interest were constructed to obtain subject-specific estimates of cueing-related activity for the following main effects: (1) gait initiation, (2) stepping over an obstacle, (3) and gait termination.
To make broader inferences about the general population from which the subjects were drawn, these estimates for contrasts were entered into a standard SPM second-level analysis with subject treated as a random effect, using one-sample t test (Penny and Holmes 2007). The expected mean difference value for the t tests was set to zero. The threshold value for statistical significance (p < 0.05) was corrected for the false discovery rate (FDR) at the voxel level (Genovese et al. 2002). An extent threshold of ten voxels was used for activated regions. The activated locations were transformed into Talairach space (Talairach and Tournoux 1988). Anatomical labels (lobes, gyri) and Brodmann area (BA) of the local maxima of the activated clusters were determined using a 3D electronic brain atlas (Lancaster et al. 2000). At the predefined threshold, the gait initiation did not evoke significant brain activation. We adopted a small volume correction (SVC) approach as required for a priori hypothesis-driven analyses. The volume of interest (VOI) was placed in the supplementary motor area (SMA).
Results
After allowance for SVC, areas of activation during the initiation of gait are shown in Fig. 2. Coordinates of the VOI in bilateral SMA were derived from a previous study (Hanakawa et al. 1999) and were as follows: right SMA (2, −20, 68) and left SMA (−14, −2, 56). We found significant bilateral activation in SMA.

Cortical activation during the initiation of gait. After allowance for a small volume correction, the figure depicts activated areas during the gait initiation imaginary task (p < 0.05 FDR). The coordinates for the volume of interest in bilateral SMA were (2, −20, 68) for the right SMA, and (−14, −2, 56) for the left SMA
In the task of stepping over an obstacle, activations of motor-related areas were observed in bilateral SMA, bilateral dorsal premotor area (PMd), right ventral premotor area (PMv), bilateral superior parietal lobule (SPL)/precuneus, as well as in visual-related area including the bilateral cuneus/middle occipital gyrus (MOG) and left MT/V5 (Fig. 3). Additional activations were also observed in the cingulate, bilateral insula, and left putamen.

Cortical activation during the stepping over an obstacle. The figure depicts activated areas during the stepping over an obstacle imaginary task. Significant activations (p < 0.05 FDR) of motor-related areas were observed in bilateral SMA, bilateral dorsal premotor area (PMd), right ventral premotor area (PMv), bilateral superior parietal lobule (SPL)/precuneus, as well as in visual-related area including the bilateral cuneus/middle occipital gyrus (MOG) and left MT/V5. Additional activations were also observed in the cingulate, bilateral insula, and left putamen
Figure 4 depicts the effect observed during the termination of gait. Activated areas included right preSMA, right PMv and PMd, bilateral superior temporal gyrus, right inferior frontal gyrus (IFG), right inferior parietal lobule (IPL), left middle frontal gyrus (MFG), right cuneus/lingual gyrus, right insula, left caudate, right lentiform nucleus, and right thalamus. Areas of activation for gait-related imaginary tasks are depicted in Table 1.

Cortical activation during the termination of gait. The figure depicts activated areas in a task of gait-related imagery as the subject stopped (p < 0.05 FDR). Activated areas included right preSMA, right PMv and PMd, bilateral superior temporal gyrus, right inferior frontal gyrus (IFG), right inferior parietal lobule (IPL), left middle frontal gyrus (MFG), right cuneus/lingual gyrus, right insula, left caudate, right lentiform nucleus, and right thalamus
Discussion
Routine walking can be considered as the result of intricate dynamic interactions between a central program and its feedback mechanisms (Rossignol et al. 2006). Human gait is one of the most complex mechanisms for the interaction of the body with itself and the environment. A better understanding into the cortical control of human gait may hold promise for treatment of human gait disorders. In this study, we developed an event-related paradigm that enabled us to explore brain activity correlated with different gait stages.
Gait initiation
Gait initiation is a transitional process from the balanced upright standing to the beginning of steady-state walking (Jian et al. 1993; Winter 1995). Previous animal studies have clearly indicated that the mesencephalic locomotor region (MLR) and its descending projections play a significant role in the initiation of stepping movements (Mori et al. 2001). MLR has been shown to receive afferent projections from a number of sources including the basal ganglia, the sensorimotor cortex and the limbic system (Armstrong 1988). Altogether, converging evidence from experimental studies indicates that there is some correlation between higher cortical activity and locomotor activity.
In our study, we have provided evidence that SMA is preferentially activated during imaginary of gait initiation (Fig. 2). Besides controlling movement preparation and movement execution (Cunnington et al. 2003; Picard and Strick 2001), SMA may be thus implicated in the control of gait initiation. An event-related potential study has indicated that the differences of cortical activation pattern between gait initiation and bipedal stepping may be related to different levels of preparation and execution (do Nascimento et al. 2005). An EEG study (Yazawa et al. 1997) has reported a significant difference in the contingent negative variation (CNV) between gait initiation and simple foot dorsiflexion. Different activations of the frontal areas—including the SMA and the primary motor cortex—may account for such discrepancy. A report using near infrared spectroscopic (NIRS) has confirmed an enhanced activity in the prefrontal and premotor cortices in prepared walking tasks compared with simple walking (Suzuki et al. 2008). Due to a reduced spatial resolution, however, previous studies did not identify the exact origin of such activity. Altogether, our data clearly indicate that SMA is involved in gait initiation. This finding is consistent with clinical findings indicating that disturbances in gait initiation may be due to SMA lesions (Della Sala et al. 2002; Nadeau 2007).
Stepping over an obstacle
Obstacle avoidance movements while stepping over an obstacle could require a more complex cerebral activation compared with simple SMA activity during the initiation of gait. Beside the dynamic balance, walking requires the control of foot trajectory over obstacles (Reynolds and Day 2005). The dorsal stream is crucial in processing information necessary for automatic obstacles avoidance. Specifically, the superior parts of the posterior parietal cortex seem to play a major role (McIntosh et al. 2004; Rice et al. 2006; Schindler et al. 2004).
The MT/V5, the superior parietal cortex, and the premotor cortex show higher activation levels when movements are guided by visual feedback (Debaere et al. 2003). In keeping with previous findings, we have shown that stepping over an obstacle requires information from the visual and somatosensory systems. In addition, visual adaptation was required for stepping over an obstacle. In the present study, an extensive visuomotor network was activated during the imaginary task of stepping over an obstacle (Fig. 3).
Gait termination
Termination of gait requires a deceleration of the forward momentum of the body and the assumption of a stable posture. Therefore, gait termination is not merely a mirror image of gait initiation (Patla 2004). During termination of gait, activations were observed in the right prefrontal area, especially in the right inferior frontal gyrus and the preSMA (Fig. 4). Of interest, these areas have been shown to contribute to the response inhibition process (Coxon et al. 2009; Leung and Cai 2007; Xue et al. 2008). Activations in right superior temporal gyrus reflected the perception of biological movement (Allison et al. 2000; Santi et al. 2003). It is also likely that activations of this area may be related to locomotion and postural control (Jahn et al. 2004).
Conclusions
In the present study, we have demonstrated a corticol control over different phases of human gait. Our results are in line with clinical findings indicating that disturbances in gait initiation may be due to SMA lesions (Della Sala et al. 2002; Nadeau 2007). There is a caveat, however, as we did not directly monitored the imagery performance of our subjects. This limitation notwithstanding, our current observations may provide us an important key to elucidate the pathophysiology of higher-level gait disorders (Nutt et al. 1993; Thompson 2007; Thompson and Nutt 2007).
References
Allison T, Puce A, McCarthy G (2000) Social perception from visual cues: role of the STS region. Trends Cogn Sci 4(7):267–278
Armstrong DM (1988) The supraspinal control of mammalian locomotion. J Physiol 405:1–37
Bakker M, de Lange FP, Stevens JA, Toni I, Bloem BR (2007a) Motor imagery of gait: a quantitative approach. Exp Brain Res 179(3):497–504
Bakker M, Verstappen CC, Bloem BR, Toni I (2007b) Recent advances in functional neuroimaging of gait. J Neural Transm 114(10):1323–1331
Buccino G, Binkofski F, Fink GR, Fadiga L, Fogassi L, Gallese V, Seitz RJ, Zilles K, Rizzolatti G, Freund HJ (2001) Action observation activates premotor and parietal areas in a somatotopic manner: an fMRI study. Eur J Neurosci 13(2):400–404
Coxon JP, Stinear CM, Byblow WD (2009) Stop and go: the neural basis of selective movement prevention. J Cogn Neurosci 21:1193–1203
Cunnington R, Windischberger C, Deecke L, Moser E (2003) The preparation and readiness for voluntary movement: a high-field event-related fMRI study of the Bereitschafts-BOLD response. Neuroimage 20(1):404–412
Debaere F, Wenderoth N, Sunaert S, Van Hecke P, Swinnen SP (2003) Internal vs external generation of movements: differential neural pathways involved in bimanual coordination performed in the presence or absence of augmented visual feedback. Neuroimage 19(3):764–776
Della Sala S, Francescani A, Spinnler H (2002) Gait apraxia after bilateral supplementary motor area lesion. J Neurol Neurosurg Psychiatry 72(1):77–85
do Nascimento OF, Nielsen KD, Voigt M (2005) Influence of directional orientations during gait initiation and stepping on movement-related cortical potentials. Behav Brain Res 161(1):141–154
Genovese C, Lazar N, Nichols T (2002) Thresholding of statistical maps in functional neuroimaging using the false discovery rate. Neuroimage 15(4):870–878
Grezes J, Decety J (2001) Functional anatomy of execution, mental simulation, observation, and verb generation of actions: a meta-analysis. Hum Brain Mapp 12(1):1–19
Grillner S, Wallen P (1985) Central pattern generators for locomotion, with special reference to vertebrates. Annu Rev Neurosci 8:233–261
Hanakawa T, Katsumi Y, Fukuyama H, Honda M, Hayashi T, Kimura J, Shibasaki H (1999) Mechanisms underlying gait disturbance in Parkinson’s disease: a single photon emission computed tomography study. Brain 122(Pt 7):1271–1282
Iseki K, Hanakawa T, Shinozaki J, Nankaku M, Fukuyama H (2008) Neural mechanisms involved in mental imagery and observation of gait. Neuroimage 41(3):1021–1031
Jahn K, Deutschlander A, Stephan T, Strupp M, Wiesmann M, Brandt T (2004) Brain activation patterns during imagined stance and locomotion in functional magnetic resonance imaging. Neuroimage 22(4):1722–1731
Jeannerod M (2001) Neural simulation of action: a unifying mechanism for motor cognition. Neuroimage 14(1 Pt 2):S103–S109
Jeannerod M (2006) Motor cognition: what actions tell to the self. Oxford University Press, Oxford
Jian Y, Winter DA, Ishac MG, Gilchrist L (1993) Trajectory of the body COG and COP during initiation and termination of gait. Gait Posture 1(1):9–22
Lancaster JL, Woldorff MG, Parsons LM, Liotti M, Freitas CS, Rainey L, Kochunov PV, Nickerson D, Mikiten SA, Fox PT (2000) Automated Talairach atlas labels for functional brain mapping. Hum Brain Mapp 10(3):120–131
Leung H-C, Cai W (2007) Common and differential ventrolateral prefrontal activity during inhibition of hand and eye movements. J Neurosci 27(37):9893–9900
MacKay-Lyons M (2002) Central pattern generation of locomotion: a review of the evidence. Phys Ther 82(1):69–83
Malouin F, Richards CL, Jackson PL, Dumas F, Doyon J (2003) Brain activations during motor imagery of locomotor-related tasks: a PET study. Hum Brain Mapp 19(1):47–62
McIntosh RD, McClements KI, Schindler I, Cassidy TP, Birchall D, Milner AD (2004) Avoidance of obstacles in the absence of visual awareness. Proc Biol Sci 271(1534):15–20
Mori S, Matsuyama K, Mori F, Nakajima K (2001) Supraspinal sites that induce locomotion in the vertebrate central nervous system. Adv Neurol 87:25–40
Munzert J, Lorey B, Zentgraf K (2009) Cognitive motor processes: the role of motor imagery in the study of motor representations. Brain Res Rev 60(2):306–326
Nadeau SE (2007) Gait apraxia: further clues to localization. Eur Neurol 58(3):142–145
Nutt JG, Marsden CD, Thompson PD (1993) Human walking and higher-level gait disorders, particularly in the elderly. Neurology 43(2):268–279
Patla AE (2004) Adaptive human locomotion: influence of neural, biological, and mechanical factors on control mechanisms. In: Bronstein AM, Brandt T, Woollacott MH, Nutt JG (eds) Clinical disorders of balance, posture and gait, 2nd edn. Arnold, London, pp 20–38
Penny WD, Holmes AJ (2007) Random effects analysis. In: Friston K, Ashburner J, Kiebel S, Nichols T, Penny W (eds) Statistical parametric mapping: the analysis of functional brain images. Academic Press, London, pp 156–165
Picard N, Strick PL (2001) Imaging the premotor areas. Curr Opin Neurobiol 11(6):663–672
Reynolds RF, Day BL (2005) Visual guidance of the human foot during a step. J Physiol 569(Pt 2):677–684
Rice NJ, McIntosh RD, Schindler I, Mon-Williams M, Demonet JF, Milner AD (2006) Intact automatic avoidance of obstacles in patients with visual form agnosia. Exp Brain Res 174(1):176–188
Rizzolatti G, Craighero L (2004) The mirror-neuron system. Annu Rev Neurosci 27:169–192
Rossignol S, Dubuc R, Gossard JP (2006) Dynamic sensorimotor interactions in locomotion. Physiol Rev 86(1):89–154
Santi A, Servos P, Vatikiotis-Bateson E, Kuratate T, Munhall K (2003) Perceiving biological motion: dissociating visible speech from walking. J Cogn Neurosci 15(6):800–809
Schindler I, Rice NJ, McIntosh RD, Rossetti Y, Vighetto A, Milner AD (2004) Automatic avoidance of obstacles is a dorsal stream function: evidence from optic ataxia. Nat Neurosci 7(7):779–784
Sirigu A, Duhamel JR (2001) Motor and visual imagery as two complementary but neurally dissociable mental processes. J Cogn Neurosci 13(7):910–919
Suzuki M, Miyai I, Ono T, Kubota K (2008) Activities in the frontal cortex and gait performance are modulated by preparation. An fNIRS study. Neuroimage 39(2):600–607
Talairach J, Tournoux P (1988) Co-planar stereotaxic atlas of the human brain: 3-dimensional proportional system: an approach to medical cerebral imaging. Thieme Medical, Stuttgart, 122 p
Thompson PD (2007) Higher level gait disorders. Curr Neurol Neurosci Rep 7(4):290–294
Thompson PD, Nutt JG (2007) Higher level gait disorders. J Neural Transm 114(10):1305–1307
Wang C, Wai Y, Kuo B, Yeh YY, Wang J (2008a) Cortical control of gait in healthy humans: an fMRI study. J Neural Transm 115(8):1149–1158
Wang C, Wai Y, Weng Y, Yu J, Wang J (2008b) The cortical modulation from the external cues during gait observation and imagination. Neurosci Lett 443(3):232–235
Winter D (1995) Human balance and posture control during standing and walking. Gait & Posture 3(4):193–214
Worsley KJ, Marrett S, Neelin P, Vandal AC, Friston KJ, Evans AC (1996) A unified statistical approach for determining significant signals in images of cerebral activation. Human Brain Mapping 4(1):58–73
Xue G, Aron AR, Poldrack RA (2008) Common neural substrates for inhibition of spoken and manual responses. Cereb Cortex 18(8):1923–1932
Yazawa S, Shibasaki H, Ikeda A, Terada K, Nagamine T, Honda M (1997) Cortical mechanism underlying externally cued gait initiation studied by contingent negative variation. Electroencephalogr Clin Neurophysiol 105(5):390–399
Acknowledgments
The study was supported jointly by the National Science Council Taiwan (Grant NSC96-2321-B-182-002-MY2) and the ChangGung Memorial Hospital (Grant CMRPG360822).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wang, J., Wai, Y., Weng, Y. et al. Functional MRI in the assessment of cortical activation during gait-related imaginary tasks. J Neural Transm 116, 1087–1092 (2009). https://doi.org/10.1007/s00702-009-0269-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00702-009-0269-y