
Abstract
Object
Francis Murphey’s theory was analyzed to determine whether or not his opinion is evidence-based medicine and whether or not it can be applied clinically.
Methods
The English literature was reviewed using Medline in reference to Dr. Murphey’s theory of discogenic chronic LBP, which was first postulated in 1967. Deductive and inductive logic was utilized for the evaluation of his theory. We reviewed and analyzed his unprecedented study of the annulus fibrosus (AF) and posterior longitudinal ligament (PLL) under local anesthesia that was presented to the Congress of Neurological Surgeons in 1967 and 1972.
Results
He reported that: “It is found that the posterior longitudinal ligament and the remaining annulus fibrosus over the herniated discs are also exquisitely tender; even the slightest pressure on them produces pain.” We noticed that in Dr. Murphey’s presentation, he did not disclose any hard data, yet he concluded: “when an incomplete tear in the annulus occurs and if the tear is in the midline posterior, a fragment of nucleus will protrude in this tear, stretching the annulus and posterior longitudinal ligament, causing midline back pain. If the tear in the annulus is lateral, the pain is over the sacroiliac joint in the buttock and hip, and 20% of the patients in the lower abdomen, groin or testicle on that side.”
Conclusions
Because of a flaw in his understanding, in our opinion the unproven mechanical theory of discogenic LBP is weak inductive logic and does not justify discography and intra-discal procedures.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Background
The oldest description of pain is in the Book of Genesis, when God expelled Adam and Eve from the Garden of Eden: “Man is cursed to labor, and woman is cursed to submit to her husband and to bear children in pain.” In the medical literature, the oldest description of lower back pain (LBP) and sciatica was noted by Hippocrates (460–370 BC) [10]. He was the first to attribute LBP and sciatica to the spine and has been named the father of spine surgery. Rudolph Virchow (1821–1902), a German physician known as the father of pathology, discovered the first herniated disc and believed that it was a kind of neoplasm. He called it “Virchow’s tumor” [16]. In 1887, Sir Victor Horsley performed the first lumbar laminectomy in London [17]. Dr. Fedor Krause, a German neurosurgeon, performed the first lumbar discectomy transdurally in 1909 [14]. Dr. Alfred Taylor (1872–1942) carried out the first unilateral laminectomy followed by extradural discectomy at Presbyterian Hospital in New York City [15].
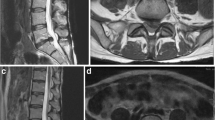
Prior to 1947, it was believed that the disc is a painless structure. Inman and Saunders in 1947 discovered nerve fibers in the annulus [6]. This was later confirmed by more sophisticated histological techniques, and today it is a known fact that the outer third of the annulus and the posterior longitudinal ligaments (PLL) are supplied by a branch of the sinuvertebral nerve [8]. It was Francis Murphey who first entertained the idea that the lumbar disc can be a source of LBP. Dr. Francis Murphey, Professor and Chairman of Neurosurgery at the University of Tennessee, at the Congress of Neurological Surgeons in 1967 in San Francisco lectured on “Sources and Patterns of Pain in Disc Disease” [12] (Fig. 1). He presented his unprecedented observations on operating on patients with herniated lumbar discs under conscious sedation and using local anesthesia; this was an observation that will never be reproduced in the future. He concluded from his intraoperative experience that a herniated disc can be a source of axial lower back pain, a concept concerning the existence of discogenic lower back pain. According to the current literature, 40% of patients experiencing chronic mechanical axial LBP are discogenic.

“Sources and patterns of pain in disc disease” by Murphey
Rationale
The rationale for our study was to determine the logical basis for discography and intradiscal procedures that are currently practiced in the management of axial LBP based on Francis Murphey’s theory.
Objective
Our research aimed to analyze Murphey’s theory (the original concept of discogenic LBP) using inductive and deductive logic and determining whether or not his theory was evidence-based medicine and has any relevance for clinical application.
Materials and methods
Study design
We designed this study to reassess the mechanical theory of Francis Murphey regarding the discogenic LBP addressed to the Congress of Neurological Surgeons using inductive and deductive logic. We reviewed the English literature to determine whether or not his observations had ever been duplicated by other investigators. We also carefully reviewed the literature to determine if the current procedures stemming from his theory in the diagnosis and treatment of a source of LBP, such as discography and intradiscal procedures, are evidence-based medicine.
Procedure
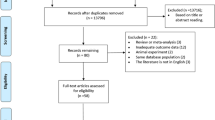
We meticulously reviewed Francis Murphey's lectures that were addressed to the Congress of Neurological Surgeons in 1967 and 1972. Inductive and deductive logic was utilized to assess his reasoning in order to determine whether or not his theory was evidence-based medicine [5]. In addition, we did a search on Medline for the source of discogenic LBP in order to see if anyone had duplicated his observation. For this reason the search was narrowed solely to the period between 1967 and 2008.
Statistical methods
Dr. Murphey did not disclose any useful hard data regarding his experience, nor were we able to collect any data from other sources after careful review of the English literature to use them in any statistical method to prove or disprove his concept.
Participants
The number of patients that were operated on by Dr. Murphey for his study is not known. We can only assume that all of his patients in this experience had had symptomatic herniated lumbar discs and the diagnosis had been confirmed by preoperative myelography, the only test that was available at that time.
Variables
It is unclear from the lectures whether or not the patients' symptoms were axial LBP only, LBP with sciatica, or a combination of both. Other demographic data were not disclosed by Dr. Murphey to classify the patients into different subgroups.
Data sources/measurement
Our data consist of limited information that was provided by Dr. Murphey to the Congress of Neurological Surgeons in 1967 and 1972. Ironically, at that lecture in 1972 in Denver, Colorado, Dr. Murphey had agreed with the topic of the lecture according to the record: “with stipulation that I did not have to review a lot of charts to back up what I intend to say.”
Results
Participants
Dr. Murphey did not disclose the number of patients that participated in his study.
Descriptive data
He failed to disclose any data in the 1967 and 1972 presentations.
Outcome data
“It is found that the posterior longitudinal ligament and the remaining annulus fibrosus over the herniated discs are also exquisitely tender; even the slightest pressure on them produces pain. In other cases, compression of the posterior longitudinal ligament and annulus does not produce pain. Strangely, while cutting these structures is not painful, compression or stretching is, as stated above, extremely painful.” He lectured in 1972: “I have already discussed the sources of pain from discs at the Congress on previous occasions well, and in everything I have ever written about discs, but let me review it again. Pressure on normal discs rarely causes pain. It is an established fact that in some discs, no matter how badly damaged they are, one cannot produce back pain by any maneuver. All of us, of course, have seen people who have had typical sciatic pain from a disc who never had back pain in their lives. I must confess that I have never taken the trouble to find out whether there are nerve fibers in such discs, but somebody should. At any rate, I have no idea why some ruptured discs are painful, and others are not” [13].
Main results
Dr. Murphey’s experience based on limited data resulted in an unproven conclusion of: “when an incomplete tear in the annulus occurs and if the tear is in the midline posteriorly, a fragment of nucleus will protrude in this tear, stretching the annulus and posterior longitudinal ligament, causing midline back pain. If the tear in the annulus is lateral, the pain is over the sacroiliac joint in the buttock and hip, and 20% of the patients in the lower abdomen, groin or testicle on that side.”
Furthermore, others have applied the concept clinically, such as in discography and the intra-discal procedures, such as chemonucleolysis, automated percutaneous lumbar discectomy, automated percutaneous intra-discal laser lumbar discectomy and intra-discal electro-thermal therapy, nucleoplasty and even discectomy for the treatment of the axial LBP.
Other analyses
Dr. Murphey’s lectures in 1967 and 1972 were only based on expert opinion statements without any scientific data presentation to back up his concept, and therefore his theory at best should be considered level V evidenced-based medicine.
Discussion
Key results
Based on our analysis Dr. Murphey’s theory at best is class V evidence-based medicine. It is not ironic that the decompression or denervation of the annulus and PLL (intradiscal procedures) as well as the excision of a herniated disc in patients with LBP without signs of radiculopathy have remained controversial [1, 4, 7, 9, 11]. In fact, the innovations of computerized tomography and magnetic resonance imaging have confirmed the fact that most of the population has an abnormal stretched annulus, yet the majority of these people do not experience the axial LBP. Dr. Murphey himself observed that “Pressure on normal discs rarely causes pain. It is an established fact that in some discs, no matter how badly damaged they are, one cannot produce back pain by any maneuver. All of us, of course, have seen people who have had typical sciatic pain from a disc who never had back pain in their lives. I must confess that I have never taken the trouble to find out whether there are nerve fibers in such discs, but somebody should. At any rate, I have no idea why some ruptured discs are painful, and others are not.” He also observed that “Strangely, while cutting these structures is not painful, compression or stretching is, as stated above, extremely painful.”
In reviewing his concept we are not questioning the observation that: “It is found that the posterior longitudinal ligament and the remaining annulus fibrosus over the herniated discs are also exquisitely tender, even the slightest pressure on them produces pain.” However, what we are questioning is whether or not the pain that was elicited in some of his patients, under sedation, was radicular pain rather than axial LBP, secondary to compression of a disc fragment on the adjacent nerve root, an issue that was not clarified in his lectures.
Interpretation
The important properties of logic, such as consistency, soundness and completeness, were the basis of our discussion.
Inductive reasoning
Inductive reasoning is used to ascribe properties or relations to types based on a number of observations or experiences, or to formulate laws based on limited observations of recurring phenomenal patterns. In the process of reasoning, the premises of an argument are believed to support the conclusion, but they do not ensure its truth [2].
Example of strong induction
All observed crows are black; therefore, all crows are black. This conclusion does not ensure the truth because of the possibility of the existence of different colored crows that have not been observed yet.
Example of a weak induction
I always put premium gas in my car; therefore, all cars require premium gas.
Dr. Murphey’s logic was weak induction because of the lack of CONSISTANCY and COMPLETENESS of the premise.
Premise: “It is found that the posterior longitudinal ligament and the remaining annulus fibrosus over the herniated discs are also exquisitely tender, even the slightest pressure on them produces pain . Pressure on normal discs rarely causes pain. It is an established fact that in some discs, no matter how badly damaged they are, one cannot produce back pain by any maneuver. All of us, of course, have seen people who have had typical sciatic pain from a disc who never had back pain in their lives." Result: Stretched annulus and PLL (herniated disc) are sources of axial LBP.
The inconsistent and incomplete observation led to a weak induction.
Deductive reasoning
Deductive reasoning was developed by Greek philosophers of the Classical period, including Aristotle, Thales and Pythagoras. Aristotelian deductive reasoning is reliant on its premises. That is, a false premise leads to a false result, and a true premise will produce a true result [3].
For example:
-
All oranges are fruit. All fruit grows on plants.
Conclusion: All oranges grow on plants. This conclusion relies on true premises, and therefore the conclusion is true.
-
All Americans emigrated from Africa. Afro-Americans are Americans.
Conclusion: All Americans are Afro-Americans.
In this case the first premise is false and has resulted in a false conclusion. In the case of Dr. Murphey’s theory:
-
Premises: (1): Herniated lumbar disc stretches the annulus and PLL. (2) The stretched annulus and PLL are sources of the axial LBP.
Result: The herniated lumbar disc is the source of axial LBP (discogenic LBP).
The first premise is accurate, but the second one is not, and this has led to an inaccurate conclusion.
Limitations
The limitation of our study was the lack of access to Dr. Murphey’s patient records in order to prove or disprove his theory. Furthermore, there has not been any duplication of his experience in the English literature, to the best of our knowledge, for further discussion of his theory. Therefore, based on the current information, his theory is unproven.
Conclusion
The mechanical theory of Francis Murphey regarding discogenic LBP, postulated in 1967 for the first time, is weak inductive logic. His lecture of 1972 addressed to the Congress of Neurological Surgeons is a class V evidence-based medicine (expert opinion). Therefore, in our opinion this unproven theory should not be used as a rationalization for discography and intradiscal procedures such as discectomy in the management of axial LBP.
References
Boult M, Fraser R, Jones N, Osti O, Dohrmann P, Donnelly P, Liddell J, Maddern GJ (2000) Percutaneous endoscopic laser discectomy. J Surg 70:475–479
en.wikipedia.org/wiki/Inductive_reasoning; Feb-27-2009
en.wikipedia.org/wiki/Deductive_reasoning; Feb-24-2009
Freeman B, Fraser R, Cain C, Hall D et al (2005) Intradiscal electrothermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine 30:2369–2377. doi:10.1097/01.brs.0000186587.43373.f2
Gabbay DM, Guenthner F (eds) (2001–2005) Handbook of philosophical logic, 13 vols, 2nd edn
Inman VT, Saunders JB (1947) Anatomical and physiological aspects of injuries to the intervertebral disc. J Bone Joint Surg 29:461
Kim YS, Chin DK, Yoon DH, Jin BH, Cho YE (2002) Predictors of successful out come for lumbar chemonucleolysis: analysis of 3,000 cases during the past 14 years. Neurosurgery 51(5 Suppl):S123–S128
Konttinen YT, Gronbald M, Antti-Poika I (1990) Neuroimmunohistochemical analysis of peridiscal nocioceptive neuro elements. Spine 15:383. doi:10.1097/00007632-199005000-00008
Marin FZ (2005) CAM versus nucleoplasty. Acta Neurochir Suppl (Wien) 92:111–114. doi:10.1007/3-211-27458-8_24
Marketos SG, Skiadas P (1999) Hippocrates: the father of the spine surgery. Spine 24:1381–1387. doi:10.1097/00007632-199907010-00018
Mayer HM (1994) Spine update. Percutaneous lumbar disc surgery. Spine 19:2719–2723
Murphey F (1967) Sources and patterns of pain in disc disease. Clin Neurosurg 15:343–351
Murphey F (1972) Experience with lumbar disc surgery. Clin Neurosurg 21:1–8
Oppenheim H, Krause F (1909) Uber Einklemmung bzw. Strangulation der cauda equine. Dtsch Med Wochenschr 35:697–700
Patwardhan RV, Hadley MN (2001) History of surgery for ruptured disk. Neurosurg Clin N Am 12:173–179
Robinson JS (1983) Sciatica and the lumbar disc syndrome: a historic perspective. South Med J 76:232–238
Tan TC, Black PM (2002) Sir Victor Horsley: pioneer of neurological surgery. Neurosurgery 50:607–611. doi:10.1097/00006123-200203000-00032
Acknowledgments
NA
Disclosure/Disclaimer
NA
Author information
Authors and Affiliations
Corresponding author
Additional information
This paper is original and has not been presented at any conferences.
Sources of Support (if applicable): NA
Rights and permissions
About this article
Cite this article
Alemo, S., Sayadipour, A. Sources and patterns of pain in lumbar disc disease; revisiting Francis Murphey’s theory. Acta Neurochir 152, 1555–1558 (2010). https://doi.org/10.1007/s00701-009-0315-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-009-0315-4