
Abstract
Object
This study was intended to objectively demonstrate the effect of interspinous implantation through preoperative and postoperative radiological analyses in degenerative lumbar spinal stenosis.
Methods
This study included 20 segments of 14 cases that had been diagnosed as spinal stenosis through physical and radiological findings and had interspinous implantation (X‐stop®). On simple radiography, height and width of the intervertebral foramen, height of the anterior and posterior intervertebral disks, and interbody angle were measured. On magnetic resonance imaging (MRI), the intervertebral foramen and intradural areas were also measured. Changes in preoperative and postoperative measurements were compared, and correlation between radiological indicators was identified. Clinical evaluation was done using visual analog scale (VAS) and Oswestry disability index (ODI) scores. The relationship between the clinical outcomes and radiological changes was also evaluated.
Results
The comparison of preoperative and postoperative radiological measurements showed significant changes in height and width of the intervertebral foramen, and interbody angle on simple radiography, and in height of the intervertebral foramen on MRI. Regarding correlation between radiological indicators, there was correlation between height of the intervertebral foramen on simple radiography and area of the intervertebral foramen on MRI, and between the intervertebral foramen and intradural areas on MRI. For correlation between the clinical improvement level and the changes in radiological parameters, VAS correlated with intervertebral foramen height on simple radiography and increased area of the intervertebral foramen on MRI. However, for ODI, there was no factor showing significant correlation.
Conclusions
In patients with degenerative spinal stenosis showing neurogenic claudication, interspinous implantation was more effective in increasing the height and area of the intervertebral foramen than in increasing intradural area, and the short‐term clinical results were promising.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Lumbar spinal stenosis (LSS) is the most common indication for lumbar spinal surgery in the elderly. LSS is characterized by manifestation of an altered sensation and weakness in the lower extremities during standing and walking, which are relieved when resting or sitting [1]. Whenever standing space between the intervertebral foramen and the spinal canal becomes narrow leading to nerve compression, while sitting or bending the spine widens the space, lessening the compression [2].
Several interspinous implantations with a range of designs and compositions have been developed and used based on the advantages of LSS. Among these, the X‐stop® device (Metronic Spine LLC, Memphis, TN, USA), a Food and Drug Administration‐approved device, achieves the gap broadening with a relatively simple surgical procedure, and favorable results have been reported from short‐ and mid‐term follow‐ups in neurogenic claudication [3–5].
However promising these clinical results are, their true importance remains to be determined, since few studies have utilized objective indicators through preoperative and postoperative radiological analyses. The present study was undertaken to objectively demonstrate the effect of interspinous implantation in degenerative LSS showing neurogenic claudication through prospective analysis on preoperative and postoperative changes in radiological parameters.
Methods
Materials
Twenty segments of 14 cases had X‐stop® interspinous implantation among those diagnosed with spinal stenosis based on findings of physical examination findings and from MRI were included for this study. The mean age was 78.4 years (range 75–82 years). All subjects were men. Surgical procedure was conducted on a single segment in eight cases and on two segments in six cases. For the surgical site, L3‐4 was used in eight cases, L4‐5 in 10 cases, and L5‐S1 in two cases. The patients’ neurogenic claudication averaged 58 m (range 20–100 m). Muscular weakness and paresthesia were not evident in 10 cases, but a decrease in power of extensor hallucis longus (EHL) to grade 4 was found in four cases. The inclusion criteria were age over 60 years; claudication symptom while standing or walking, with relief when rest in a sitting or bending posture; and diagnosis of spinal stenosis or intervertebral foramen, compatible with the symptoms on preoperative MRI. Among these, the surgical procedure was mainly conducted in those who had received conservative treatment such as medication or physical therapy and exercise therapy for 3 months or more without improvement of symptoms. The exclusion criteria were unstable findings on preoperative flexion‐extension radiography or accompaniment of spondylolisthesis; severe compression as to cause cauda equina syndrome, bowel or bladder incontinences; and presence of osteoporosis with bone mineral density (BMD) < −2.5. We have experienced two cases of intro-operative spinous process fractures during the implantation. These cases were not included for this study. Follow-up MRI was conducted in all cases at 2 weeks postoperatively. Unstable findings on flexion-extension radiography was defined when (1) sagittal plane displacement >4.5 mm or (2) sagittal plane angulation >22° [6].
Operation protocol
Surgery was conducted in all patients under general anesthesia. Prior to surgery, the presence of a gap between the spinous processes that was sufficient to insert the implant was checked using a fluoroscope at the surgical site. The degree of flexion was also checked. A median incision of approximately 3 cm was made, followed by exposure of the site without damage to the supraspinous ligament, and the paraspinal muscle was detached and exposed to a level of the medial one‐third of the facet joint. A pilot hole was formed with a small dilator from right‐to‐left in the interspinous ligament, and it was placed to be as anterior as possible to reduce the risk of dislodgement and to maximize flexion of the vertebral body and enlargement of the intervertebral foramen. After the dilator was removed, a sizing distractor was inserted through the pilot hole until the end appeared in the left side, and then a size sufficient to maintain proper tension was selected. Excessive extension was prevented to avoid fracture of the spinous processes or iatrogenic kyphosis. The degree of extension and size of implant to be inserted were measured with a fluoroscope to form a proper gap between the spinous processes as well as for spinal alignment. Once the proper size of implant was decided, the distractor was eliminated, and the implant was inserted. A wing was put in the left screw hole and was fixed with a torque‐limiting hexagonal screw driver. Lastly, the position of the implant, gap between the spinous processes, extension of the intervertebral foramen, and spinal alignment were checked with a fluoroscope, and suturing was done in a routine manner without insertion of a drainage tube.
Radiological analysis
Comparative analysis of findings on preoperative and postoperative simple radiography and MRI were conducted. All postoperative measurements were done using radiographs taken 14 days after the operation. The simple radiograph was taken in a neutral position when the patient stood, and the height and width of the intervertebral foramen of the segment, heights of the anterior and posterior intervertebral disks, and interbody angle were measured preoperatively and postoperatively (Fig. 1). For the height of the intervertebral foramen, the longer dimension between the lower margin of the upper vertebra pedicle and the upper margin of the lower vertebra pedicle was measured. For determination of the width of the intervertebral foramen, the front‐rear distance of the intervertebral foramen was measured in an extension line of the lower endplate [7]. For determination of the height of the anterior intervertebral disk, the distance between the anterior end of the lower margin of the upper vertebra and that of the upper margin of the lower vertebra at the segment was measured, and height of the posterior intervertebral disk was measured at the posterior margin of the vertebrae in the same manner. For determination of interbody angle, the angle between the lower margin of the upper vertebra and the upper margin of the lower vertebra at the segment was measured.

Measures parameters on plain radiographs. a Foraminal height, b foraminal width, c anterior disk height, d posterior disk height, e intervertebral angle
In all cases, MRI (1.5 T Magneton vision; EXITE HD; GE, USA) was taken, and slice thickness was set to 3 mm in both T1 and T2. On MRI, the area of the intervertebral foramen and intradural area were measured. The area of the intervertebral foramen was measured by using the T2‐weighted image among sagittal planes at the slice where the intervertebral foramen was found to be largest among sites with the nerve root going out, and intradural area was measured by using the T2‐weighted image of axial view at the slice, where the intradural area was found to be smallest at the relevant intervertebral disk. These measurements were used for analysis. All measurements were made using the m‐view™ PACS system (MaroTech, Korea).
Changes in preoperative and postoperative measurements were compared, and correlations between radiological indicators were identified. Regarding measurement reliability, measurement was done per item two times each by two spine surgeons, and the mean value was used. To identify intra‐observer (K1) and inter‐observer (K2) reliability, the kappa coefficient test was conducted and measurement reliability was obtained. For preoperative and postoperative comparison of radiological results, t test was used, and for correlation analysis of radiological results, Pearson correlation ratio was used. For all statistical analyses, SPSS version 12.0 was used, and the result was deemed statistically significant at p < 0.05.
Clinical analysis
The clinical improvement level of preoperative and last follow-up visual analog scale (VAS) and Oswestry disability index (ODI) was demonstrated, and correlation of the improvement level between clinical indicators and radiological indicators was analyzed. Mean follow-up period was 17.5 months (range 12–21 months). For statistical analysis, a Pearson correlation ratio was used between changes in preoperative and postoperative VAS and ODI and changes in radiological parameters.
Results
For K1 and K2 reliability measurement for two observers, the kappa coefficient test was used. The result was found to be reliable by items (K1 = 0.80, K2 = 0.74).
The comparison of preoperative and postoperative radiological measurements showed increase in height and width of the intervertebral foramen, and interbody angle on simple radiography (Table 1). In MRI measurements, the area of the left intervertebral foramen changed from 68.66 mm2 preoperatively to 88.80 mm2 postoperatively, and the area of the right intervertebral foramen changed from 73.62 to 85.36 mm2 (p = 0.003 and p = 0.015, respectively). The intradural area increased from 118.18 mm2 preoperatively to 123.52 mm2 postoperatively; the increase was not statistically significant (p = 0.24).
In terms of the correlation between radiological indicators, correlation was shown between the height of the intervertebral foramen and that of the anterior and posterior intervertebral disks on simple radiography, between the height of the intervertebral foramen on simple radiography and area of the intervertebral foramen on MRI, and between area of the intervertebral foramen and intradural area on MRI (Table 2).
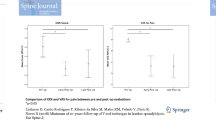
From the clinical results, VAS decreased from 6.3 preoperatively to 3.8 at the last follow‐up, and ODI improved from 38.5 preoperatively to 24.3 at the last follow‐up. Regarding the correlation between the clinical improvement and the changes in radiological parameters, VAS was correlated with height of the intervertebral foramen on simple radiography and with an increased area of the intervertebral foramen on MRI (Table 3).
Discussion
LSS manifests with degenerative changes of the spine, and symptoms may result from changes in area of the spinal canal according to posture, as well as anatomical changes. At spinal extension, the ligament flavum protrudes and the posterior annulus fibrous moves to the spinal canal, and the intervertebral foramen leads to neurogenic claudication. In previous anatomical studies with corpses, when the spine was moved from the flexion state to the extension state, the spinal canal itself decreased by 40 mm [2, 8]. Another study reported that at extension, area of the intervertebral foramen decreased by 24 % and area of the spinal canal by 16 % [9]. Results of an MRI‐based study in 12 asymptomatic applicants indicated that the area of the spinal canal decreased by 16 % at L4‐5 according to postural changes, and area of the intervertebral foramen decreased by 35 % [10]. Similar to the present study, changes in area of the spinal canal and that of the intervertebral foramen with postural changes were identified both anatomically and radiologically, and such changes influenced the actual manifestation of symptoms in patients. X‐stop® has advantageous effects on the spine in kinematical aspects. These include decreasing the range of motion (ROM) at flexion‐extension of the inserting site, increasing the area of the intervertebral foramen and area of the spinal canal, decreasing intervertebral pressure of the inserted segment, and decreasing the pressure applied to the facet joint and contact area. Good short‐ and mid‐term follow‐up results after X‐stop® implantation have been reported in many clinical studies. There was improvement in clinical symptoms in patients accounting for 60.2 % during 2‐year follow-up in a prospective study [5, 6], and a 4‐year follow‐up showed successful results in patients accounting for 78 % [11]. However, no previous studies have directly compared spinal stenosis patients and patients who had received decompression. The present direct comparison yielded a result that was only marginally different from previous studies, that is a success rate of 55–70 % of decompression surgery through foraminal incision. A recent study reported that 8 of 69 patients suffered from complications, and among these, reoperation was conducted in 4 cases [12]. The complications included dislocation of the implanted device and fracture of the spinous processes. The collective data indicate that treatment of spinal stenosis using X‐stop® is a minimally invasive surgical procedure that leads to good results without directly operating on the nerves, without serious complications. But, the clinical results are not satisfactory compared to previous laminectomy cases. Thus, for the present time, the procedure will be selectively available and should be regarded as one of the time saving procedural options available. Also, in one case with severe stenosis, the symptom initially improved after X‐stop® was inserted, but recurred at 7 months to a level similar to the preoperative condition.
Sobottke ret al. [7] reported that as a result of analysis on changes in radiological parameters after interspinous implantation with preoperative and postoperative simple radiographs, postoperative height and width of the intervertebral foramen, height of the anterior and posterior intervertebral disks, and interbody angle increased. But there was little correlation between the degree of radiological changes and the improvement in clinical findings, and changes in radiological parameters during follow‐up tended to return to the preoperative condition, and, in this case, clinical symptoms did not get worse. Siddiqui et al. [13] reported that as a result of preoperatively and postoperatively measuring area of the intervertebral foramen and that of the spinal canal, not on simple radiography but on MRI, the area of the intervertebral foramen increased by 20 % and that of the spinal canal increased by 21–23 %. The area of the intervertebral foramen increased by 16 and 29 %, respectively, but area of the spinal canal insignificantly increased by just 5 %. However, all patients showed postoperative improvement in neurogenic claudication and VAS, which indicated that regarding symptomatic improvement in spinal stenosis patients, not only spinal canal area but also area of the intervertebral foramen would play an important role.
In this study, regarding correlation between radiological indicators, correlations between height of the intervertebral foramen and that of the anterior and posterior intervertebral disks on simple radiography, between height of the intervertebral foramen on simple radiography and area of the intervertebral foramen on MRI, and between area of the intervertebral foramen and intradural area on MRI were shown. Also, postoperative changes in the height of the intervertebral foramen on simple radiography were measured; changes in the area of the intervertebral foramen could be estimated. Therefore, in an economic aspect, the surgical effect could be estimated just with simple postoperative radiography. It will be useful method for long‐term follow‐up.
Limitations of this study are relatively small number of cases and the short‐term follow‐up. The authors expect that useful information will be obtained with more cases and longer follow‐up.
Conclusions
In patients with degenerative spinal stenosis showing neurogenic claudication, interspinous implantation was more effective in increasing height and area of the intervertebral foramen than in increasing intradural area, and the simple radiographs were and efficient method to evaluate the postoperative state.
References
Verbiest H (1954) A radicular syndrome from developmental narrowing of the lumbar vertebral canal. J Bone Joint Surg Br 36:230–237
Chung SS, Lee CS, Kim SH (2000) Effect of low back posture on the morphology of the spinal canal. Skeletal Radiol 29:217–223
Lindsay DP, Swanson KE, Fuchs P, Hsu KY, Zucherman JF, Yerby S (2003) The effects of an interspinous implant on the kinematics of the instrumented and adjacent levels in the lumbar spine. Spine 28:2192–2197
Zucherman JF, Hsu KY, Hartjen CA et al (2004) A prospective randomized multi-center study for the treatment of lumbar spinal stenosis with the X STOP interspinous implant: 1 year results. Eur Spine J 13:22–31
Zucherman JF, Hsu KY, Hartjen CA et al (2005) Multicenter, prospective randomized trial evaluating the XSTOP interspinous process decompression system for the treatment of neurogenic intermittent claudication. Spine 30:1351–1358
White AA, Panjabi MM (1990) Clinical biomechanics of the spine, 2nd edn. JB Lippincott Co, Philadelphia, pp 23–45
Sobottke R, Schlüter-Brust K, Kaulhausen T et al (2009) Interspinous implants (X Stop, Wallis, Diam) for the treatment of LSS: is there a correlation between radiological parameters and clinical outcome? Eur Spine J 18:1494–1503
Schonstrom N, Lindahl S, Willén J et al (1989) Dynamic changes in the dimensions of the lumbar spinal canal: an experimental study in vitro. J Orthop Res 7:115–121
Infusa A, An HS, Lim TH et al (1996) Anatomic changes of the spinal canal and intervertebral foramen associated with flexion-extension movement. Spine 21:2412–2420
Schmid MR, Stucki G, Duewell S et al (1999) Changes in the cross-sectional measurements of the spinal canal and intervertebral foramina as a function of body position: in vivo studies on an open-configuration MR system. AJR Am J Roentgenol 172:1095–1102
Kondrashov DG, Hannibal M, Hsu KY, Zucherman JF (2006) Interspinous process decompression with the X-STOP device for lumbar spinal stenosis: a 4-year follow-up study. J Spinal Disord Tech 19:323–327
Barbagallo GM, Olindo G, Corbino L, Albanese V (2009) Analysis of complications in patients treated with the X-Stop Interspinous Process Decompression System: proposal for a novel anatomic scoring system for patient selection and review of the literature. Neurosurgery 65:111–119
Siddiqui M, Karadimas E, Nicol M, Smith FW, Wardlaw D (2006) Influence of X Stop on neural foramina and spinal canal area in spinal stenosis. Spine 31:2958–2962 (Phila Pa 1976)
Conflict of interest
The authors state that there are no conflicts of interest. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of the article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, HY., Choi, BW. Change of radiological parameters after interspinous implantation (X-stop®) in degenerative spinal stenosis. Eur J Orthop Surg Traumatol 23, 281–285 (2013). https://doi.org/10.1007/s00590-012-0986-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-012-0986-z