
Abstract
Purpose
Adolescent idiopathic scoliosis (AIS) is a three-dimensional spinal deformity that affects 5% of the population. This pathology has multiple known etiological factors such as family predisposition, female gender, low body mass index, decrease in lean and fat masses. However, recent studies suggest that ciliary dysfunction could be the origin of certain types of obesity and AIS. This study aims to verify the existence of a link between these two pathologies.
Methods
A retrospective, cross-sectional, descriptive and monocentric study, based on a cohort of adolescents with obesity treated in a paediatric rehabilitation centre for specific care between 1 January 2010 and 1 January 2019. The prevalence of AIS was calculated by radiographic measurements. The diagnosis of AIS was established if the Cobb angle was ≥ 10°, associated with intervertebral rotation.
Results
196 adolescents with obesity were included in the study (mean age 13.2 years, mean BMI 36 kg/cm2, gender ratio 2.1 of female to male.) The prevalence of AIS in adolescents with obesity was 12.2%, twice the prevalence of AIS in the general population. The characteristics of AIS in adolescents with obesity are predominantly female, 58.3% left thoracolumbar or lumbar principal curvatures, mean Cobb angle 26° and progressive in 29% of cases.
Conclusions
Our study established a correlation between AIS and obesity with a higher prevalence than in the general population. The morphology of these adolescents makes screening for AIS more difficult.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Adolescent idiopathic scoliosis (AIS) is a three-dimensional spinal deformity diagnosed clinically by the presence of a trunk rotation measured with the Bunnel scoliometer (angle of trunk rotation or ATR).
It is confirmed radiologically by the association of intervertebral rotation and frontal deviation of at least 10° [1].
The prevalence of idiopathic scoliosis in 8- to 15-year-olds ranges from 0.47 to 5.2% [2,3,4]. In 2010, one meta-analysis found a mean prevalence of AIS of 5% in the general population [5].
Multiple etiological factors can contribute to AIS such as genetic, hormonal and neurodevelopmental factors. Family predisposition, female gender and low body mass index (BMI) are all risk factors for developing AIS [3, 4]. A "typical" AIS patient is a tall female with decreased lean and fat masses [2, 6].
In Europe, a mutation of the POC5 gene is found in 10% of inherited AIS [7], and a POC5 variant is significantly associated with AIS in the Chinese population [8]. Poc5/POC5 is involved in the function of primary sensory cilia and embryonic nodal cilia [7]. It also appears to play an important role in the embryonic development of the rostro-caudal axis [9]. Another study confirms the existence of ciliary dysfunction in AIS, precisely a disruption of osteoblast ciliary mechano-sensation and a change in their cilia length [10]. Ciliopathies include a large number of pathologies characterised by significant phenotypic variability, of which obesity is a major symptom (e.g. Bardet-Biedl syndrome, or Alström syndrome) [11, 12].
Despite very different morphotypes, a primary cilium alteration is found in certain syndromic obesity and in AIS. Moreover, AIS mainly affects girls in the peri-pubertal phase and progresses during puberty, a period that involves significant anthropometric changes. To assess a potential link between obesity and AIS, we conducted a study in which the main objective was to analyse the prevalence of AIS in a cohort of adolescents with obesity. Secondary objectives were to describe the typical profile of AIS obese patients and to assess possible anthropometric characteristics of obese scoliotic adolescents.
Method
Design
This is a retrospective, cross-sectional, descriptive and monocentric study, based on a multicentre recruitment. The cohort of patients includes adolescents with obesity treated in our paediatric rehabilitation centre between 1 January 2010 and 1 January 2019.
Population
The inclusion and non-inclusion criteria are presented in Table 1. The patients were adolescents with obesity defined by a BMI ≥ 97° percentile of the BMI curves, according to gender and age. It is the clinical threshold recommended in France for children and adolescents who are overweight or obese (body weight curves from the Programme National Nutrition Santé-2010), taken from both French references and the International Obesity Task Force) (http://www.sante.gouvfr/IMG/pdf/PNNS_2011-2015.pdf).
Adolescents and their legal guardians were given oral and written information about the use of their medical records for research purposes. For this study, all data were anonymised in accordance with the Helsinki Declaration, as revisited in 2013, about Patient’s Rights. The ethics committee of our hospital accepted this research (n°2019–02-001). Because our study is retrospective, we have not submitted it to the national review committee (permanent authorization for retrospective studies: MR-003).
Outcome measures
The patients all benefited from an institutional therapeutic education programme for adolescents suffering from obesity, during 3 months. The treatment was multidisciplinary, combining physiotherapy, adapted physical activities and health education supervised by a dietician, a psychologist, and a paediatrician-nutritionist.
This intensive rehabilitation programme included high intensity physical activities. Some contra-indications were therefore systematically eliminated by carrying out a low dose EOS radiographic examination of the whole spine. This evaluation made it possible to eliminate certain pathologies such as growth spondylitis (Scheuermann's disease), spondylolisthesis, etc. A static spinal evaluation was also systematically carried out: presence of scoliotic curvatures by noting the topography, type of curvature structural with rotation or non-structural without rotation), Cobb angle and Risser test.
On the first day of the stay, total body fat was assessed by Tanita bio-electrical impedance (TANITA BC-420MA). It measured weight, height, BMI, fat mass (FM) and lean mass (LM).
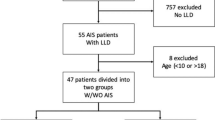
A total of 287 adolescent patients were treated for obesity management between 1 January 2010 and 1 January 2019 (Fig. 1). Of these, 85 records with missing data and 2 with refusal to participate in the study, were excluded, and four patients with secondary scoliosis were also excluded (one Klinfelter syndrome, one Prader-Willi syndrome, one craniopharyngioma operated with complete hypopituitarism, one latero-cervico-thoracic desmoid tumour). A total of 196 adolescents were included in this study.

Flow chart
Patients with radiographic scoliotic curvature with a Cobb angle ≥ 10° and intervertebral rotation were classified in the scoliosis group, and the others in the control group.
Data analysis
Qualitative data were presented as numbers and percentages. Quantitative data was expressed as mean and standard deviation and/or median and interquartile range. The normality of the numerical parameters was checked graphically and by the Shapiro–Wilk test.
In the cohort of adolescents with obesity, assessment of the frequency of scoliosis and anthropometric parameters were estimated with a confidence interval of 95%. The two groups were compared by Chi-2 or Fisher exact tests on qualitative parameters and by Student's t test or Mann–Whitney U test on quantitative anthropometric parameters. An evaluation of the correlations by the "Spearman/Coor Procedure" method was made between the Cobb angle and the quantitative data (age, weight, BMI, FM, LM).
The significance threshold was set at 5%. Statistical analysis was performed using SAS software, version 9.4 (SAS Institute, Cary, NC, USA).
Results
Descriptive evaluation of the cohort
Our cohort consisted of 196 patients whose anthropometric characteristics are described in Table 2. The gender ratio of male to female was 1/3.
The frequency of radiological scoliosis (defined by a Cobb angle ≥ 10° and vertebral rotation) was 12.2% (24/196) with a 95% confidence interval (CI 95%) of (8–17.6%), following a Gaussian distribution.
Characteristics of scoliosis in adolescents with obesity
Among the 24 adolescents with obesity and radiological scoliosis, the main structural curvature was predominantly left thoracolumbar or left lumbar (58.3%) (Table 3).
The mean Cobb angle of the main structural curvature was 26.4° (± 18.4°), with a median of 21° (minimum = 15°—maximum = 89°).
Comparison of scoliotic adolescents with obesity
Comparison of anthropometric data between the two groups showed a predominance of females in the scoliosis group (p = 0.04). Adolescents with AIS had less advanced bone growth evaluated by Risser classification (p = 0.026) (Table 4). There was a tendency towards a lower BMI in the scoliosis group, but no significant difference with the control group.
Comparison by Cobb angle
We evaluated and compared the scoliosis according to their Cobb angles. At the time of diagnosis (first X-ray), the Cobb angle was < 20° for 40% of patients, and > 30° for 20% of patients. We compared the anthropometric parameters in two sub-groups, according to the median Cobb angle (21°) (Table 5). There was no significant anthropometric difference between the two populations nor was there any correlation between anthropometric data and Cobb angle.
Evolution
Twenty-one out of 24 patients had their AIS followed up for 6 to 56 months (mean = 17.8 months). In 29% of cases (7 patients, including 4 females), the AIS was progressive (Cobb angle ≥ 30° and/or worsened > 5° between two radiographic evaluations).
Discussion
The aim of this study was to assess the prevalence of AIS in a cohort of exclusively adolescents with obesity. In our patients, the prevalence was 12.24% which is more than double the prevalence found in most studies [2,3,4,5]. To our knowledge, no other study has specifically assessed the prevalence of AIS in adolescents with obesity.
Studies indicate that patients with AIS have alterations in their body composition combining low BMI, decreased bone density, low percentage of fat and lean body mass (13–18). We could have expected to find a lower prevalence of AIS in our obese adolescent population than in the general population. However, our results show otherwise. There are several possible explanations for these results. In 2019, Escriva et al. evaluated the distribution of adiposity in young females with AIS. In scoliotic patients, the prevalence of underweight, overweight and obese subjects compared to age-matched non-scoliotic controls was assessed [13]. The proportion of adolescents with obesity was twice as high in AIS as in age-matched controls [13]. Durmala et al. have shown that classification of nutritional status by BMI underestimates the number of patients with obesity in AIS study [14, 15]. AIS diagnosis in adolescents with obesity is difficult due to the loss of anatomical relief. Thus, in subjects with obesity and scoliosis, ATR is less visible, waist folds are less marked, and trunk tilt is less frequent [16]. Furthermore, adolescents with obesity tend to have a more negative body image and to perform less physical activity. There are fewer opportunities to see them shirtless, making diagnostic situations less frequent [16]. Finally, the lower penetration of X-rays into fatty tissue decreases radiographic accuracy [17].
In our cohort, as in the general population, AIS affects mostly girls (75% of cases) [19]. This result is probably overestimated in our population, which is predominantly composed of girls (55.6%).
AIS in our patients with obesity has some specific features.
The mean angle of our scoliosis (26°) patients with obesity is high compared to the mean angle of AIS individuals in general population [3, 18]. 40% of our AIS patients had a Cobb angle below 19°. Zheng et al. found an average of 18° in 1021 AIS patients, aged 10–16 years (the population included 33 obese and 125 overweight patients) [20]. In Penha's study, 75% of AIS patients had a Cobb angle < 22° [21]. This difference with our results can be partly explained by the high variability of the scoliosis angle (standard deviation 15°–89°). Moreover, other explanations are possible. Obese children tend to be taller and show faster height gain, especially in the prepubertal period, compared to age-matched normal weight subjects [22, 23]. Peripubertal growth rate is a factor in the worsening of AIS [24].
This higher mean of Cobb angle could also be related to a delay in diagnosis, for the reasons given above, which limit early detection of scoliosis in obesity [16]. Therefore, it seems unlikely that scoliotic curvatures with an average Cobb angle of 26° have a postural origin.
-
The topography of the main scoliotic curvature in our population is not common: it is lumbar or left thoracolumbar in 58.3%. This is different from the typical distribution of scoliosis, which is right thoracic in 80% of AIS [24, 25]. It is possible that the lumbar spinal segment is more sensitive to morphological changes associated with obesity. There is a significant relationship between body weight and increased lumbar lordosis in obesity [26]. The explanation could be a hyper pressure on the vertebral bodies with asymmetric inhibition of the growth plates and peri-vertebral muscle maladjustment. This mechanism could also explain the aggravation of a pre-existing lumbar scoliotic curvature and therefore the over-representation of lumbar and thoracolumbar curvatures in our population. However, this hypothesis still needs to be proven.
-
In a little less than one third of cases, AIS in our adolescents is progressive, with no relation to gender or initial BMI.
-
We found no correlation between anthropometric parameters and Cobb angle, although we note a tendency for a lower BMI in the obese scoliotic group
Our study establishes a link between obesity and AIS. This population of obese scoliotic adolescents probably represents a subgroup with a different morphotype than the usual phenotypic description in AIS: AIS with a preferential lumbar or left thoracolumbar topography, found at a higher Cobb angle, due to the difficulties of screening in these patients [3, 4]. It is therefore important for the clinician to be particularly vigilant when screening for scoliosis in an adolescent suffering for obesity [16]. If there is any clinical doubt (tilt of the shoulder girdle, ATR from 5°), a weight-bearing total spine X-ray should be performed.
Recent work suggests possible explanations for this link. This study raises the possibility that ciliary dysfunction could be at the origin of AIS [7, 10]. Obesity is a prime symptom in some ciliopathies [11, 12]. Some types of obesity and AIS could therefore have a common origin via ciliary dysfunction.
Our research does not provide arguments in favour of this hypothesis.
Numerous genetic studies underway will make it possible to answer these hypotheses soon.
Conclusion
Scientific literature shows a strong correlation between AIS and a morphotype associating low BMI, decreased fat and lean masses. However, our study is the first to show that the prevalence of AIS in adolescent with obesity patients is twice as high as that found in general population. This scoliosis is more severe, which is probably due to delayed diagnosis. Adolescent obesity is a global public health problem. It is important to treat scoliotic deformities in this population by considering the difficulties of screening and diagnosis.
References
Negrini S, Aulisa AG, Aulisa L, Circo AB, de Mauroy JC, Durmala J, Grivas TB, Knott P, Kotwicki T, Maruyama T, Minozzi S, O’Brien JP, Papadopoulos D, Rigo M, Rivard CH, Romano M, Wynne JH, Villagrasa M, Weiss HR, Zaina F (2012) 2011 SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis 27(1):3. https://doi.org/10.1186/1748-7161-7-3
Konieczny MR, Senyurt H, Krauspe R (2013) Epidemiology of adolescent idiopathic scoliosis. J Child Orthop 7(1):3–9. https://doi.org/10.1007/s11832-012-0457-4
Penha PJ, Ramos NLJP, de Carvalho BKG, Andrade RM, Schmitt ACB, João SMA (2018) Prevalence of Adolescent Idiopathic Scoliosis in the State of São Paulo, Brazil. Spine (Phila Pa 1976) 43(24):1710–1718. doi: https://doi.org/10.1097/BRS.0000000000002725
Hengwei F, Zifang H, Qifei W, Weiqing T, Nali D, Ping Y, Junlin Y (2016) Prevalence of idiopathic scoliosis in chinese schoolchildren: a large, population-based study. Spine (Phila Pa 1976) 41(3):259–64. https://doi.org/10.1097/BRS.0000000000001197
Fong DY, Lee CF, Cheung KM, Cheng JC, Ng BK, Lam TP, Mak KH, Yip PS, Luk KD (2010) A meta-analysis of the clinical effectiveness of school scoliosis screening. Spine (Phila Pa 1976) 35(10):1061–71. https://doi.org/10.1097/BRS.0b013e3181bcc835
Wei-Jun W, Xu S, Zhi-Wei W, Xu-Sheng Q, Zhen L, Yong Q (2012) Abnormal anthropometric measurements and growth pattern in male adolescent idiopathic scoliosis. Eur Spine J 21(1):77–83. https://doi.org/10.1007/s00586-011-1960-x
Patten SA, Margaritte-Jeannin P, Bernard JC, Alix E, Labalme A, Besson A, Girard SL, Fendri K, Fraisse N, Biot B, Poizat C, Campan-Fournier A, Abelin-Genevois K, Cunin V, Zaouter C, Liao M, Lamy R, Lesca G, Menassa R, Marcaillou C, Letexier M, Sanlaville D, Berard J, Rouleau GA, Clerget-Darpoux F, Drapeau P, Moldovan F, Edery P (2015) Functional variants of POC5 identified in patients with idiopathic scoliosis. J Clin Invest 125(3):1124–1128. https://doi.org/10.1172/JCI77262
Xu L, Sheng F, Xia C, Li Y, Feng Z, Qiu Y, Zhu Z (2018) Common Variant of POC5 Is Associated With the Susceptibility of Adolescent Idiopathic Scoliosis. Spine (Phila Pa 1976) 43(12):E683–E688. https://doi.org/10.1097/BRS.0000000000002490.
Dantas TJ, Daly OM, Conroy PC, Tomas M, Wang Y, Lalor P, Dockery P, Ferrando-May E, Morrison CG (2013) Calcium-binding capacity of centrin2 is required for linear POC5 assembly but not for nucleotide excision repair. PLoS One 8(7):e68487. https://doi.org/10.1371/journal.pone.0068487
Oliazadeh N, Gorman KF, Eveleigh R, Bourque G, Moreau A (2017) Identification of elongated primary cilia with impaired mechanotransduction in idiopathic scoliosis patients. Sci Rep 7:44260. https://doi.org/10.1038/srep44260
Baker K, Beales PL (2009) Making sense of cilia in disease: the human ciliopathies. Am J Med Genet C Semin Med Genet 151C(4):281–295. https://doi.org/10.1002/ajmg.c.30231. (PMID: 19876933)
Mok CA, Héon E, Zhen M (2010) Ciliary dysfunction and obesity. Clin Genet 77(1):18–27. https://doi.org/10.1111/j.1399-0004.2009.01305.x
Escrivá D, Benet I, Burgos J, Barrios C (2019) Adiposity-age distribution and nutritional status in girls with adolescent idiopathic scoliosis. Spine Deform 7(4):565–570. https://doi.org/10.1016/j.jspd.2018.10.007
Durmala J, Matusik E, Durmala J, Matusik P (2013) Wadolowski K (2013) The usefulness of bioelectrical body composition analysis (BIA) in the proper assessment of nutritional status in children and adolescents with idiopathic scoliosis (IS). Scoliosis 8(Suppl 2):O35
Matusik E, Durmała J, Matusik P, Piotrowski J (2012) Evaluation of nutritional status of children and adolescents with idiopathic scoliosis: a pilot study. Ortop Traumatol Rehabil 14(4):351–362. https://doi.org/10.5604/15093492.1005093
Goodbody CM, Sankar WN, Flynn JM (2017) Presentation of adolescent idiopathic scoliosis: the bigger the kid, the bigger the curve. J Pediatr Orthop 37(1):41–46. https://doi.org/10.1097/BPO.0000000000000580
Uppot RN, Sahani DV, Hahn PF, Gervais D, Mueller PR (2007) Impact of obesity on medical imaging and image-guided intervention. AJR Am J Roentgenol 188(2):433–440. https://doi.org/10.2214/AJR.06.0409
Zheng Y, Wu X, Dang Y, Yang Y, Reinhardt JD, Dang Y (2016) Prevalence and determinants of idiopathic scoliosis in primary school children in Beitang district, Wuxi. China J Rehabil Med 48(6):547–553. https://doi.org/10.2340/16501977-2098
Konieczny MR, Senyurt H (2013) Krauspe R (2013) Epidemiology of adolescent idiopathic scoliosis. J Child Orthop 7(1):3–9. https://doi.org/10.1007/s11832-012-0457-4
Zheng Y, Dang Y, Yang Y, Sun N, Wang T, Li H, Zhang L, He C, Wong MS (2017) A case-control study of body composition, prevalence, and curve severity of the patients with adolescent idiopathic scoliosis in the East Part of China. Spine Deform 5(6):374–380. https://doi.org/10.1016/j.jspd.2017.04.002
Penha PJ, Ramos NLJP, de Carvalho BKG, Andrade RM, Schmitt ACB, João SMA (2018) Prevalence of adolescent idiopathic scoliosis in the State of São Paulo. Brazil Spine 43(24):1710–1718. https://doi.org/10.1097/BRS.0000000000002725
Vignolo M, Naselli A, Di Battista E, Mostert M, Aicardi G (1988) Growth and development in simple obesity. Eur J Pediatr 147(3):242–244. https://doi.org/10.1007/BF00442687
Davison KK, Susman EJ, Birch LL (2003) Percent body fat at age 5 predicts earlier pubertal development among girls at age 9. Pediatrics 111(4 Pt 1):815–821. https://doi.org/10.1542/peds.111.4.815
Cheng JC, Castelein RM, Chu WC, Danielsson AJ, Dobbs MB, Grivas TB, Gurnett CA, Luk KD, Moreau A, Newton PO, Stokes IA, Weinstein SL, Burwell RG (2015) Adolescent idiopathic scoliosis. Nat Rev Dis Primers 1:15030. https://doi.org/10.1038/nrdp.2015.30
Lenke LG, Betz RR, Harms J, Bridwell KH, Clements DH, Lowe TG, Blanke K (2001) Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Jt Surg Am 83-A:1169–1181
Smith AJ, O’Sullivan PB, Beales DJ, de Klerk N, Straker LM (2011) Trajectories of childhood body mass index are associated with adolescent sagittal standing posture. Int J Pediatr Obes 6(2–2):e97-106. https://doi.org/10.3109/17477166.2010.530664
Funding
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No competing financial interests exist for all authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Catanzariti, JF., Rimetz, A., Genevieve, F. et al. Idiopathic adolescent scoliosis and obesity: prevalence study. Eur Spine J 32, 2196–2202 (2023). https://doi.org/10.1007/s00586-023-07709-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07709-1