
Abstract
Purpose
The aim of this study is to evaluate the factors that affect health-related quality of life (HRQoL) in untreated adolescent idiopathic scoliosis (AIS) patients in adulthood. We investigate the effect of clinical and radiological parameters on the SRS-22 results.
Methods
A total of 286 untreated adolescent idiopathic scoliosis patients at adult age between April 2021 and April 2022 who were admitted to our clinic were included in the study. Rotational deformities were evaluated with a scoliometer. Cobb angles, coronal balance, clavicle angle, coronal pelvic tilt, trunk shift, and apical vertebral translation were measured in standing anteroposterior X-rays. The effect of each clinical and radiological parameter on SRS-22 results was evaluated.
Results
No correlation was found between gender, age, curve type, presence of gibbosity or diagnosis time, and SRS-22 scores. A negative correlation was found between the BMI of the patients and the self-image scores (r = − 0.246, p < 0.01) and function scores (r = − 0.193, p < 0.05). Main thoracic (MT) gibbosity negatively correlates with self-image and total SRS-22 scores. Also, negative correlations were found between lumbar/thoracolumbar (LTL) gibbosity, function, and pain scores. MT Cobb angle magnitude was negatively correlated with self-image, mental health, and total SRS-22 scores. There were negative correlations between clavicle angle and mental health score, coronal pelvic tilt and self-image score, and apical vertebral translation and pain score.
Conclusion
BMI, MT gibbosity, LTL gibbosity, MT Cobb angle, clavicle angle, coronal pelvic tilt, and apical vertebral translation were negatively correlated with SRS-22 domains in untreated AIS patients in adulthood.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adolescent idiopathic scoliosis (AIS) is defined as a > 10° of lateral curvature of the spine with vertebral rotation. Although AIS affects 2–3% of adolescents, only 0.3–0.5% of the curves progress to more than 20° and require treatment. Patients with Cobb’s angle of 20–40° require conservative treatment methods, while patients with a deformity of > 40° deformity and growth potential require surgery in adolescence [1,2,3,4]. Curves > 40–50° are expected to increase by 1° every year in adulthood; recently, curve progression has been reported to continue even after skeletal maturity, especially in patients with > 30° [1, 5, 6]. Patients with neglected curves, those who refuse treatment, those who do not notice their deformity until adulthood, and those who are lost to follow-up prevent us from knowing the exact fate of non-operated deformities in adulthood. Some alterations in the quality of life can be expected in such patients.
Several studies have investigated the health-related quality of life (HRQoL) of adult patients with untreated AIS patients in adulthood and have demonstrated comparable results to those without spinal deformity [5, 6]. Although these patients experience back pain, respiratory problems, lower physical performance, psychological disturbance, and body image anxiety, they do not lag behind in adulthood functions, such as having a job, getting married, and having children [1, 5,6,7]. These studies investigated the effects of age, surgical or non-surgical treatments, Cobb’s angles, and body mass index (BMI) on HRQoL. Additionally, the effects of gibbosity as a clinical feature and radiological features that can affect HRQoL such as coronal balance, clavicle angle, and trunk shift were evaluated. However, the effect of the period after the diagnosis of scoliosis on the quality of life has never been investigated.
The HRQoL of patients with AIS is a widely studied subject and scoliosis-specific questionnaires have been developed to evaluate the disease-specific quality of life. The SRS-22 especially emphasizes the aforementioned problems that patients with AIS experience and can also be used for assessment in adulthood or after undergoing different treatments [5,6,7,8,9,10,11,12,13,14]. We aimed to evaluate the clinical and radiological factors that could affect HRQoL in adult patients with untreated AIS in adulthood. We investigated the effect of clinical and radiological parameters on the SRS-22 results in these patients.
Methods
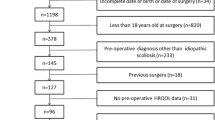
Our institutional review board reviewed and approved this single-center cross-sectional study (2021/113). All patients were fully informed and written informed consent was obtained. Adult patients with untreated AIS admitted to our clinic between April 2021 and April 2022 were included in the study. All the included patients were aware that they had scoliosis or had been referred to a spine specialist by another physician. The inclusion criteria were patients who were 20–50 years old, with or without a previous diagnosis of AIS in childhood. Patients with postural disturbances, coronal plane deformities < 10°, and with congenital, neuromuscular, or other secondary scoliosis were excluded from the study. Finally, 286 patients (194 females and 92 males) were enrolled in the study. Patients were defined as untreated if they did not undergo a standard physiotherapy program.
All patients were asked to complete the SRS-22 questionnaire before the radiological evaluation. The SRS-22 is the most widely used disease-specific questionnaire, and the reliability and validity of the Turkish version have been demonstrated [10]. The SRS-22 evaluates the self-reported pain, the functional capacity of the patient, the self-image perception of the patient, and mental health. The age, sex, occupation, weight, and height of the patients were recorded, and the BMI was calculated for all patients. Patients were asked when the diagnosis of scoliosis was made by a doctor and was recorded. Rotational deformities were clinically evaluated using a scoliometer in the proximal thoracic (PT), main thoracic, and lumbar/thoracolumbar (LTL) regions. The Cobb’s angle, coronal balance, clavicle angle, coronal pelvic tilt, trunk shift, and apical vertebral translation were measured on standing anteroposterior spine radiographs. Because it was not appropriate to use the Lenke classification for the curvatures included in the study, the patients were divided into three groups according to the gibbosity apex measurements using a scoliometer: thoracic curves, LTL curves, and double curves according to the gibbosity measurements with scoliometer at the apex. If the direction of the scoliometer changed in the thoracic and lumbar curves, it was considered as a double curve. The effects of each clinical and radiological parameter on the SRS-22 results were evaluated.
SPSS (version 20, IBM, Chicago, IL, USA) program was used for the statistical analysis. The Shapiro–Wilk test was used to examine the normal distribution of the continuous data with normal distribution. Among the descriptive statistics, age is expressed as mean ± standard deviation. Since the SRS-22 scores and angle values did not fit the normal distribution, they are expressed as medians (min–max) in the tables. The number and percentage values are provided for nominal variables. Relationships between the SRS scores and continuous data were examined using Spearman's correlation coefficient (Fig. 1).
Results
The average age of the patients was 28.64 ± 7.41 years (range 20–50 years) and the average time to scoliosis diagnosis was 5.97 ± 6.21 years (0–30 years). Sixty-eight of the patients (24%) had just received their scoliosis diagnosis. The average BMI of the patients was 23.51 ± 2.58 kg/m2.
Of the included patients, 34 patients (11.9%) had a PT gibbosity, 220 (76.9%) had an MT gibbosity, and 198 (69.2%) had an LTL gibbosity. PT Cobb’s angle was measured in 48 patients (16.7%), MT Cobb’s angle was measured in 235 patients (82.1%) and LTL Cobb’s angle was measured in 209 patients (73%). The clinical and radiological measurements of the patients are presented in Table 1. The SRS-22 scores for the entire cohort were 4.06 ± 0.60 for function, 3.29 ± 0.79 for pain, 3.25 ± 0.74 for self-image, 3.16 ± 0.82 for mental health, and 3.50 ± 0.87 for satisfaction; the total score was 3.45 ± 0.57. There were no significant differences in the SRS-22 domains according to the curve type.
No correlation was found between sex, age, curve type, or presence of gibbosity and the SRS-22 scores. A negative correlation was found between the patients’ BMI and the SRS-22 self-image scores (r = − 0.246, p = 0.003) and function scores (r = − 0.193, p = 0.021). As the BMI values of the patients increased, their self-image and function scores decreased. Although we found no correlation between age and the SRS-22 results, self-image scores decreased as the time since scoliosis diagnosis increased (r = −0.189, p = 0.024) (Table 2).
When the effect of scoliometer measurements on SRS-22 scores was evaluated, no relationship was found between PT gibbosity and the SRS-22 scores. MT gibbosity negatively correlates with self-image (r = −0.170, p = 0.042) and total SRS-22 (r = −0.182, p = 0.030) scores (Fig. 2). In addition, negative correlations were found between LTL gibbosity and the function (r = −0.184, p = 0.028), and pain (r = −0.202 p = 0.015) scores (Fig. 3). No correlations were found for other the SRS-22 sub-scores (Table 3).

a Coronal balance is the distance between CSVL and C7PL. The clavicle angle represents the angle between the line connecting the highest points of the clavicles and the horizontal line. Coronal pelvic tilt represents the angle between the line connecting the highest points of the iliac crest and horizontal line b Apical vertebral translation is the distance between CSVL and the midpoint of the apical vertebra c Trunk Shift. After drawing a horizontal line between the margins of the trunk through the apical vertebra (yellow line), the difference between the midpoint of this line and CSVL is calculated as trunk shift. (\(\frac{\text{The length of horizontal yellow line}}{2}-\text{The length of horizontal red line}\)). CSVL: Central sacral vertical line, C7PL: C7 plumb line

Correlations between main thoracic gibbosity and SRS-22 scores

Correlations between lumbar/thoracolumbar gibbosity and SRS-22 scores
The magnitudes of the PT and LTL Cobb angles did not affect the SRS-22 scores. The MT Cobb angle magnitude was negatively correlated with the self-image, mental health, and total SRS-22 scores (Fig. 4). Other correlations between the radiological measurements and SRS-22 scores are shown in Table 4. There were negative correlations between the clavicle angle and mental health score, between coronal pelvic tilt and self-image score, and between apical vertebral translation and pain score. The trunk shift did not affect the SRS-22 scores (Table 4).

Correlations between main thoracic Cobb angles and SRS-22 scores
Discussion
The natural history of AIS has been proposed in previous studies. Recently, patient-perceived questionnaires have been used to determine HRQoL. A decrease in physical capacity, cosmetic issues, and respiratory trouble have been revealed as the main problems experienced by patients with untreated AIS [1, 2, 6, 15]. Although the HRQoL of untreated AIS patients has recently been studied, the relationship between clinical or radiological parameters and HRQoL remains unclear. The SRS-22 is ideal for demonstrating HRQoL in adult patients with untreated AIS [12, 16]. In this study, we found correlations between our measurements and SRS-22 domains.
Although high BMI values delay the diagnosis of curvature in adolescence, preoperative BMI was found to have no relation to curve correction in adolescence. Both low BMI and high BMI values are associated with worse outcomes and satisfaction scores [7, 17,18,19]. Similar to adolescent patients, overweight adult patients with scoliosis have worse quality of life scores than normal or underweight patients [20, 21]. Kieser et al. demonstrated the effect of BMI on pain and function scores in adult patients with spinal deformities using various questionnaires including the total SRS-22 score. However, they did not evaluate all domains of the SRS-22 [21]. In this study, BMI was found to be negatively correlated with the self-image and function domains. Although this study demonstrated lower function and self-image scores, high BMI did not affect SRS-22 pain scores. Increased BMI was found to be associated with chronic low back pain in both normal and scoliosis patients [21, 22]. It is expected that additional weight on a curved spine can cause more pain on a straight one. This study could not demonstrate a relationship between pain scores and BMI.
The study by Watanabe et al. found that patients with non-operated AIS with structural LTL curves experienced more pain than MT and DM curves in the middle ages. The study included 107 patients with curves > 30° [6]. In contrast, we included all curves > 10°, and they were classified according to the gibbosity in thoracic and LTL regions. Ohashi et al. found a correlation between low back pain and L3–L4 tilt [5]. Erwin et al. compared thoracic and thoracolumbar curves and found that patients with thoracolumbar curves had worse scores. Contrary to these results, we found no differences between the curve types when using the SRS-22 questionnaire in this study. We probably obtained different results due be the inclusion of smaller curves that produced less pain or L3–L4 tilt. Including all the curves allowed us to obtain more accurate correlations. Moreover, not using standard radiological classifications and using gibbosity to determine the structural curves may have affected our results.
In addition to using a rib hump measured with a scoliometer to determine the structural curves in this study, the correlations between the magnitude of gibbosity magnitude and SRS-22 domains were analyzed. The increase in the thoracic rib hump caused a decrease in the self-image scores and total SRS-22 scores of the patients. Additionally, LTL gibbosity was found to be negatively correlated with the SRS-22 function and pain scores. In contrast to previous studies, we used the rib hump as a quality-of-life parameter, and not as a method of evaluating the efficacy of treatment; our results revealed that the magnitude of MT and LTL gibbosity magnitudes were related to the HRQoL. The correlations that we demonstrated will guide the physicians or physiotherapists who treat adult patients with AIS.
Cobb’s angle measurement is the most commonly used radiological parameter to determine deformity correction. Several studies have demonstrated a relationship between Cobb’s angle and HRQoL in AIS both in adolescence and adulthood [7, 23, 24]. In contrast, Ward et al. claimed that there was no relationship between the Cobb’s angle and the SRS-22 scores in patients > 18 years of age and with curves > 40° curves [25]. In this study, we found that the MT Cobb’s angles were negatively correlated with the self-image, mental health, and total SRS scores, whereas no such correlation was found for the PT and LTL Cobb’s angles. Our results suggest that the study design filled the gap between the aforementioned studies. We included curves > 10°, which differs from Ward’s study. Since a correlation was shown between LTL gibbosity and HRQoL, it was expected that there also would be a correlation with the LTL Cobb’s angles; however, this was not seen in our study.
The other radiological parameters that we used in this study are rarely investigated as factors influencing HRQoL, especially in adult patients with untreated AIS [23, 26]. Li et al. demonstrated a weak correlation between apical vertebral translation and self-image scores among adolescents. In addition, they used the T1 tilt angle to evaluate the relationship between shoulder imbalance and HRQoL and found a weak correlation [23]. There are opposing views on whether the T1 tilt angle is related to the SRS-22 scores [27, 28]. We used the clavicle angle to evaluate the shoulder imbalance and found a negative correlation between the clavicle angle and mental health score. Negative correlations were observed between the coronal pelvic tilt and self-image score, and between the apical vertebral translation and pain score in this study. These parameters were also related to the SRS-22 total scores. Trunk shift did not affect the SRS-22 scores in this study. Previous studies have not provided a definitive regarding the effect of these parameters on HRQoL [7, 23,24,25,26]. Knowing the relationship between radiological parameters and the HRQoL can enable healthcare professionals to direct area-specific treatment according to the patient's curvature and HRQoL domain.
This study included a large population of patients who had just learned about their disease and who had known about it for a very long time. Although there was no difference between the newly detected patients and those who had received their scoliosis diagnosis at least a year ago, there was a negative correlation between the time since diagnosis and the self-image scores. This is a newly demonstrated correlation, and further investigation is required.
The present study had several limitations. First, this study did not evaluate the patient deformity at maturity due to its cross-sectional design, and we were unable to demonstrate the relationship between HRQoL and curve progression. In addition, as this was a single-center study, some sociocultural or socioeconomic differences may have affected the results of our study. In our opinion, since our hospital is easily accessible in the country's capital and serves different socio-cultural groups, this limitation may have only minimally affected the results.
Conclusions
It is very difficult to establish the effect of each parameter in a patient with a deformity especially when several factors can affect it at the same time. We determined and evaluated suspicious clinical and radiological suspicious parameters and evaluated them. BMI, MT gibbosity, LTL gibbosity, MT Cobb’s angle, clavicle angle, coronal pelvic tilt, and apical vertebral translation were negatively correlated with the SRS-22 domains in adult patients with untreated AIS. Our results can guide physicians in the management of patients with untreated AIS.
Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. Code availability Statistics code is available upon request.
References
Weinstein SL (2019) The natural history of adolescent idiopathic scoliosis. J Pediatr Orthop 39(Issue 6, Suppl 1):S44–S46. https://doi.org/10.1097/BPO.0000000000001350
Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA (2008) Adolescent idiopathic scoliosis. Lancet 371(9623):1527–1537. https://doi.org/10.1016/S0140-6736(08)60658-3
Haberal B, Yaradılmıs YU (2021) Adolescent idiopathic scoliosis: a bibliographic analysis of the most 50 cited articles. J Turk Spinal Surg 32(1):1–7. https://doi.org/10.4274/jtss.galenos.2021.376
Tambe AD, Panikkar SJ, Millner PA, Tsirikos AI (2018) Current concepts in the surgical management of adolescent idiopathic scoliosis. Bone Joint J 100-B (4):415–424. https://doi.org/10.1302/0301-620X.100B4.BJJ-2017-0846.R2
Ohashi M, Watanabe K, Hirano T, Hasegawa K, Katsumi K, Shoji H, Mizouchi T, Endo N (2018) Predicting factors at skeletal maturity for curve progression and low back pain in adult patients treated nonoperatively for adolescent idiopathic scoliosis with thoracolumbar/lumbar curves: a mean 25-year follow-up. Spine (Phila Pa 1976) 43(23):E1403–E1411. https://doi.org/10.1097/BRS.0000000000002716
Watanabe K, Ohashi M, Hirano T, Katsumi K, Mizouchi T, Tashi H, Minato K, Hasegawa K, Endo N (2020) Health-related quality of life in nonoperated patients with adolescent idiopathic scoliosis in the middle years: a mean 25-year follow-up study. Spine (Phila Pa 1976) 45(2):E83–E89. https://doi.org/10.1097/BRS.0000000000003216
Erwin J, Carlson BB, Bunch J, Jackson RS, Burton D (2020) Impact of unoperated adolescent idiopathic scoliosis in adulthood: a 10-year analysis. Spine Deform 8(5):1009–1016. https://doi.org/10.1007/s43390-020-00142-0
Ersen O, Ozyurek S, Ekinci S, Bilgic S, Koca K, Oguz E, Sehirlioglu A (2013) Are distal fusion level and quality of life related in adolescent scoliosis? J Turk Spinal Surg 24:111–116
Asher M, Min Lai S, Burton D, Manna B (2003) The reliability and concurrent validity of the scoliosis research society-22 patient questionnaire for idiopathic scoliosis. Spine (Phila Pa 1976) 28(1):63–69. https://doi.org/10.1097/00007632-200301010-00015
Alanay A, Cil A, Berk H, Acaroglu RE, Yazici M, Akcali O, Kosay C, Genc Y, Surat A (2005) Reliability and validity of adapted Turkish Version of Scoliosis Research Society-22 (SRS-22) questionnaire. Spine (Phila Pa 1976) 30(21):2464–2468. https://doi.org/10.1097/01.brs.0000184366.71761.84
Danielsson AJ, Hasserius R, Ohlin A, Nachemson AL (2010) Health-related quality of life in untreated versus brace-treated patients with adolescent idiopathic scoliosis: a long-term follow-up. Spine (Phila Pa 1976) 35(2):199–205. https://doi.org/10.1097/BRS.0b013e3181c89f4a
Baldus C, Bridwell KH, Harrast J, Edwards C 2nd, Glassman S, Horton W, Lenke LG, Lowe T, Mardjetko S, Ondra S, Schwab F, Shaffrey C (2008) Age-gender matched comparison of SRS instrument scores between adult deformity and normal adults: are all SRS domains disease specific? Spine (Phila Pa 1976) 33(20):2214–2218. https://doi.org/10.1097/BRS.0b013e31817c0466
Bridwell KH, Cats-Baril W, Harrast J, Berven S, Glassman S, Farcy JP, Horton WC, Lenke LG, Baldus C, Radake T (2005) The validity of the SRS-22 instrument in an adult spinal deformity population compared with the Oswestry and SF-12: a study of response distribution, concurrent validity, internal consistency, and reliability. Spine (Phila Pa 1976) 30(4):455–461. https://doi.org/10.1097/01.brs.0000153393.82368.6b
Bridwell KH, Berven S, Glassman S, Hamill C, Horton WC 3rd, Lenke LG, Schwab F, Baldus C, Shainline M (2007) Is the SRS-22 instrument responsive to change in adult scoliosis patients having primary spinal deformity surgery? Spine (Phila Pa 1976) 32(20):2220–2205. https://doi.org/10.1097/BRS.0b013e31814cf120
Ascani E, Bartolozzi P, Logroscino CA, Marchetti PG, Ponte A, Savini R, Travaglini F, Binazzi R, Di Silvestre M (1986) Natural history of untreated idiopathic scoliosis after skeletal maturity. Spine (Phila Pa 1976) 11(8):784–789. https://doi.org/10.1097/00007632-198610000-00007.
Berven S, Deviren V, Demir-Deviren S, Hu SS, Bradford DS (2003) Studies in the modified Scoliosis Research Society Outcomes Instrument in adults: validation, reliability, and discriminatory capacity. Spine (Phila Pa 1976) 28(18):2164–2169; discussion 2169. https://doi.org/10.1097/01.BRS.0000084666.53553.D6
De La Rocha A, McClung A, Sucato DJ (2014) Increased body mass index negatively affects patient satisfaction after a posterior fusion and instrumentation for adolescent idiopathic scoliosis. Spine Deform 2(3):208–213. https://doi.org/10.1016/j.jspd.2013.12.005
Lonner BS, Toombs CS, Husain QM, Sponseller P, Shufflebarger H, Shah SA, Samdani AF, Betz RR, Cahill PJ, Yaszay B, Newton PO (2015) Body mass index in adolescent spinal deformity: comparison of Scheuermann’s Kyphosis, adolescent idiopathic scoliosis, and normal controls. Spine Deform 3(4):318–326. https://doi.org/10.1016/j.jspd.2015.02.004
Pérez-Prieto D, Sánchez-Soler JF, Martínez-Llorens J, Mojal S, Bagó J, Cáceres E, Ramírez M (2015) Poor outcomes and satisfaction in adolescent idiopathic scoliosis surgery: the relevance of the body mass index and self-image. Eur Spine J 24(2):276–280. https://doi.org/10.1007/s00586-014-3486-5
Smith JS, Shaffrey CI, Glassman SD, Carreon LY, Schwab FJ, Lafage V, Arlet V, Fu KM, Bridwell KH (2013) Spinal deformity study group. Clinical and radiographic parameters that distinguish between the best and worst outcomes of scoliosis surgery for adults. Eur Spine J 22(2):402–410. https://doi.org/10.1007/s00586-012-2547-x
Kieser DC, Wyatt MC, Boissiere L, Hayashi K, Cawley DT, Yilgor C, Larrieu D, Fujishiro T, Alanay A, Acaroglu E, Kleinstueck F, Pellisé F, Perez-Grueso FJS, Bourghli A, Vital JM, Gille O, Obeid I; European Spine Study Group (2019) The effect of increasing body mass index on the pain and function of patients with adult spinal deformity. J Spine Surg 5(4):535–540. https://doi.org/10.21037/jss.2019.11.12
Heuch I, Heuch I, Hagen K, Zwart JA (2013) Body mass index as a risk factor for developing chronic low back pain: a followup in the Nord-Trøndelag Health Study. Spine (Phila Pa 1976) 38:133–139. https://doi.org/10.1097/BRS.0b013e3182647af2
Li J, Tseng C, Yuan Y, Jiang D, Qian Z, Hu Z, Zhu Z, Qiu Y, Liu Z (2021) Determining the association between the radiographic parameters and the SRS-22 scores in Chinese female patients with adolescent idiopathic scoliosis: does curve pattern matter? Br J Neurosurg 25:1–7. https://doi.org/10.1080/02688697.2021.1875396
Fortin C, Grunstein E, Labelle H, Parent S, Ehrmann Feldman D (2016) Trunk imbalance in adolescent idiopathic scoliosis. Spine J 16(6):687–693. https://doi.org/10.1016/j.spinee.2016.02.033
Ward WT, Friel NA, Kenkre TS, Brooks MM, Londino JA, Roach JW (2017) SRS-22r scores in nonoperated adolescent idiopathic scoliosis patients with curves greater than forty degrees. Spine (Phila Pa 1976) 42(16):1233–1240. https://doi.org/10.1097/BRS.0000000000002004
Misterska E, Glowacki M, Latuszewska J, Adamczyk K (2013) Perception of stress level, trunk appearance, body function and mental health in females with adolescent idiopathic scoliosis treated conservatively: a longitudinal analysis. Qual Life Res 22(7):1633–1645. https://doi.org/10.1007/s11136-012-0316-2
Matamalas A, Bagó J, D’Agata E, Pellisé F (2016) Does patient perception of shoulder balance correlate with clinical balance? Eur Spine J 25(11):3560–3567. https://doi.org/10.1007/s00586-015-3971-5
Ono T, Bastrom TP, Newton PO (2012) Defining 2 components of shoulder imbalance: clavicle tilt and trapezial prominence. Spine (Phila Pa 1976) 37(24):E1511–E1516. https://doi.org/10.1097/BRS.0b013e31826e2bbb
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by OE and UY. The first draft of the manuscript was written by OE and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Erşen, Ö., Yüzügüldü, U., Başak, A.M. et al. Effect of clinical and radiological parameters on the quality of life in adult patients with untreated adolescent idiopathic scoliosis: a cross-sectional study. Eur Spine J 32, 1196–1203 (2023). https://doi.org/10.1007/s00586-023-07571-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07571-1