
Abstract
Purpose
To report the clinical characteristics and surgical outcomes of scoliosis in patients with spinal muscular atrophy (SMA) from Mainland China.
Methods
Nineteen patients were retrospectively analyzed. Demographic, anthropometric and respiratory parameters were collected preoperatively. Surgical program was analyzed. Radiographic data were measured perioperatively. Motor status, ventilation support, sitting ability and respiratory symptoms were evaluated preoperatively and at final follow-up.
Results
Age at surgery was 17.08 (12.83, 20.08) years. More than 40% of patients were diagnosed with low weight. Pulmonary dysfunction was observed in all patients. All patients received posterior spinal fusion (PSF). Sacroiliac fixation with sacral-2 alar iliac technique was used in 16 patients. Major curve correction rate was 54.87 ± 16.14%. Pelvic obliquity correction rate was 63.84 ± 23.70%. T1–T12 height, space-available-for-lung ratio and thoracic transverse diameter were increased (p < 0.001). Percentage of patients capable of sitting independently increased from 26.32% preoperatively to 73.68% at final follow-up. Cumulative scores of sitting-related items in muscular dystrophy spine questionnaire improved from 19.11 ± 5.40 preoperatively to 26.21 ± 5.20 at final follow-up. Total scores of symptomatic domains in St. George’s Respiratory Questionnaire decreased from 4 (2, 12) preoperatively to 1 (0, 3) at final follow-up.
Conclusions
SMA patients in China always present severe scoliosis at late adolescence, accompanied with high proportion of low weight and pulmonary dysfunction. PSF is effective for the correction of scoliosis and pelvic obliquity and the improvement of thoracic morphology. Sitting ability and respiratory symptoms were improved postoperatively.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Spinal muscular atrophy (SMA) is an autosomal recessive motor neuron degenerative disease caused by the deletion or mutation of survival motor neuron 1 (SMN1) [1]. Dysfunction of SMN1 gene brings about insufficient supply of SMN protein, resulting in progressive muscular weakness of both trunk and extremities.
Weakness of axial muscle leads to scoliosis. Scoliosis in SMA is characterized by early onset, rapid progress and concomitant respiratory impairment, making surgical intervention necessary but formidable [2]. Accompanied with scoliosis, various skeletal deformities develop, including thoracic deformities, pelvic obliquity (PO) and hip dysplasia. Scoliosis and PO bring about sitting imbalance. Besides, scoliosis and thoracic abnormalities together exacerbate respiratory compromise. Therefore, treatment of skeletal deformities is critical for controlling scoliosis progression and improving quality of life (QOL) in SMA patients.
Multiple surgical procedures have been introduced for the correction of scoliosis in SMA. Definite spinal fusion for scoliosis correction and spinal stabilization has been used in SMA since decades ago [3]. Nowadays, posterior spinal fusion (PSF) with pedicle screws is a common procedure for spinal correction in skeletally mature SMA patients. For patients with great growth potential, non-fusion devices, such as traditional growing rods (TGR), magnetically controlled growing rods (MCGR) and vertical expandable prosthetic titanium rib (VEPTR), were used [4,5,6]. Attempt to manage PO in SMA with Luque–Galveston technique has been developed since 1980s [7]. The latest spinopelvic fixation technique, sacral-2 alar iliac (S2AI) technique proposed by Sponseller et al. [8] has been adopted rapidly in the past decade. However, up to now there are few studies concerning on the application of S2AI technique in SMA patients. Besides, currently there is no report on the surgical treatment of scoliosis in SMA patients from Mainland China. This study aimed to evaluate surgical outcomes of scoliosis in SMA patients in our institution and to gain further insight into its clinical characteristics and surgical management.
Methods
Population
Approved by institutional review board, medical records of SMA patients receiving scoliosis correction in Peking Union Medical College Hospital between November 2014 and September 2021 were retrospectively reviewed. Inclusive criteria included: (1) genetic confirmed SMA, (2) complete clinical and radiographic data and (3) follow-up for at least 6 months. Surgical indications were: (1) a Cobb angle > 50°, (2) inability to maintain sitting balance and (3) back or flank pain having failure to conservative therapy. All surgical procedures were performed by a senior orthopedic surgeon (J. Shen). Written informed consent was obtained from adult patients or legal guardians.
Clinical evaluation and data acquisition
Genetic analysis and clinical classification were performed by a senior neurologist. Demographics data, including gender, age of scoliosis onset and age at surgery, were collected. Anthropometric parameters, including recumbent length and body weight, were recorded. Body mass index (BMI) was calculated. For adults, BMI < 18.5 kg/m2 was considered as underweight [9]. For adolescents, BMI was compared with growth references for Chinese [10]. A BMI-for-age and gender Z-score (BAZ) < − 1 was defined as low weight in adolescents as this cutoff roughly corresponds with BMI of 18.5 kg/m2 in adults [11]. Preoperative respiratory data, including pulmonary function testing (PFT) parameters and arterial blood gas (ABG) results, were analyzed. Ventilatory support and motor status were recorded preoperatively and at final follow-up. Perioperative data, such as anesthesia and operation time, intensive care unit (ICU) stay, estimated blood loss (EBL), blood transfusion amount, drain time and drainage volume, were collected using our institutional database. Surgical program was analyzed. Perioperative complications were reviewed. Scores for sitting-related items (questions 7, 11, 15, 16, 17, 22, 24, 26 and 27) of the muscular dystrophy spine questionnaire (MDSQ) and symptomatic domain (Part 1) of the St. George’s Respiratory Questionnaire (SGRQ) were obtained before surgery and at final follow-up.
Radiographic measurement
Radiographic imaging was undertaken before surgery and 1 week after surgery. Main curve Cobb angle (MCCA), PO (angle between the horizontal line and inter iliac crest line), kyphosis and thoracic height (T1–T12) were measured on sitting whole spine radiographs. Hemithorax height (HTH) and thoracic transverse diameter (TTD) were measured as previously described [12, 13]. Space-available-for-lung ratio (SALR) was calculated according to Corona and colleagues [12]. Measurements were conducted by 2 senior attending spine surgeons.
Statistical analysis
Measures in normal distribution were presented as mean ± standard deviation (SD). Median (P25, P75) was applied to describe data with a non-normal distribution. Changes from baseline to postoperative assessment were compared by paired t test or Wilcoxon test. Difference between groups was compared by independent samples t test or Mann–Whitney U test. Qualitative data were described as percentages and compared by chi-square test between groups. A P value < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS (version 22.0, IBM).
Results
Demographic and anthropometric data
A total of 20 consecutive patients were identified. One patient was excluded due to lack of historical images. Among the 19 patients enrolled (11 females, 8 males), 14 were classified into type II group; while the remaining 5 into type III group (Table 1). Average age of scoliosis onset was 7.68 ± 3.13 years. Twelve patients were diagnosed with scoliosis before 8 years old. Median age at surgery was 17.08 (12.83, 20.08) years. Preoperative supine length and body weight were 1.52 ± 0.11 m and 42.87 ± 13.29 kg, respectively. Average BMI was 18.47 ± 4.68 kg/m2. Percentage of patients with low weight was 42.11%. No difference concerning above indexes was observed between groups (all P > 0.05).
Pre-operative pulmonary function
One SMA type II patient failed to complete PFT due to maxillofacial deformity. Respiratory compromise was confirmed in all 18 patients completed PFT (Table 1). Average forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) were 1.08 ± 0.55 L and 1.23 ± 0.6 L, respectively. Percentage of predicted value of FEV1 (FEV1%) and that of FVC (FVC%) were 38.57 ± 14.22% and 37.42 ± 14.26%, respectively. Average PaO2 and PaCO2 were 86.82 ± 8.78 mmHg and 38.63 ± 3.04 mmHg, respectively. Average SpO2 was 96.99 ± 0.94%. No difference in PFT and ABG results was observed between groups (all P > 0.05).
Peri-operative information
Perioperative information is shown in Table 2. Preoperative halo traction was recommended for patients with severe and rigid scoliosis; among those 10 patients accepted halo-gravity traction. Anesthesia and operation time were 9.30 ± 1.28 h and 7.62 ± 1.15 h, respectively. EBL was 1500 (1000, 1800) mL. Autotransfusion was applied in all patients with a median amount of 633 (389, 1084) mL. All patients received allogeneic packed red blood cells transfusion perioperatively with an average amount of 1131.58 ± 501.17 mL. Average drain time after surgery was 4.21 ± 0.98 days, with total drainage quantity of 1065.05 ± 367.82 mL. PSF was undertaken in all patients with a median fusion length of 17 (16, 18) segments. Multiple-rod constructs were applied in 17 patients. Sixteen patients received sacropelvic fixation (SPF) with S2AI technique. All patients were transferred to ICU postoperatively. Median length of ICU stay was 24.75 (20.5, 65) hours. Median time till tracheal extubation after surgery was 17 (14.67, 36) hours.
Radiographic outcomes
Single curve was observed in 15 patients (Table 3). Average MCCA was 114.24 ± 25.36° preoperatively and 53.42 ± 22.52° postoperatively (P < 0.05), with a correction rate of 54.60 ± 16.12%. PO improved from 28.9 (22.5, 39.6)° preoperatively to 11.9 (4.2, 20)° postoperatively (P < 0.05), with a correction rate of 63.84 ± 23.70%. Kyphosis decreased from 115.4 (87.8, 133.4)° preoperatively to 39.8 (29.5, 42.3)° postoperatively (P < 0.05). Mean thoracic height increased from 180.01 ± 40.91 to 240.81 ± 30.59 mm (P < 0.05). Besides, TTD increased from 196.64 ± 47.66 to 220.14 ± 46.74 mm after surgery (P < 0.05). Both HTH-concave and HTH-convex increased significantly after surgery (all P < 0.05). SALR was improved from 72.20 ± 13.44% preoperatively to 88.51 ± 7.29% postoperatively (P < 0.05). No difference in preoperative radiographic parameters between groups was observed (all P > 0.05). However, type III group presented a wider TTD but a smaller SALR after surgery compared with type II group (all P < 0.05).
Complications
Complications are summarized in Table 4. No pulmonary infection or failure occurred. Two type II patients underwent epiglottic edema and had delayed tracheal extubation. Delayed healing of wound occurred in 2 type II patients. There was no surgical site infection (SSI) or mechanical complications. Neurological function of all patients remained stable after surgery.
QOL
As shown in Table 5, none of the patients retained ambulation ability before surgery, while all patients were able to drive an electric wheelchair. Percentage of patients capable of sitting independently was increased from 26.32% preoperatively to 73.68% at final follow-up (P < 0.05). Meanwhile, cumulative scores of sitting-related items in MDSQ were increased from 19.11 ± 5.40 to 26.21 ± 5.20 (P < 0.05).
Three patients took noninvasive ventilation (NIV) routinely before surgery, with an average time of 10.33 ± 1.53 h per day. Original scheme of NIV remained unchanged in these 3 patients postoperatively. Cough-assist device (CAD) was applied in 5 patients before surgery. Two patients got rid of the regular use of CAD postoperatively, though no significant change in the percentage of patients with CAD was observed (P > 0.05). Additionally, there was also no significant decrease in the frequency of CAD usage after surgery (P > 0.05). Cumulative scores of symptomatic domains in SGRQ were reduced from 4 (2, 12) preoperatively to 1 (0, 3) at final follow-up (P < 0.05).
Discussion
In this study, surgically treated SMA patients are characterized by high proportion of low weight and ubiquity of pulmonary impairment. Severe scoliosis with PO is found as a common radiographic feature in SMA. Definite PSF effectively ameliorates spinal deformities, PO and thoracic morphology and improves QOL in SMA patients.
The severe curvature presented in this cohort could be due to the relative old age at surgery. As reported, prior treatment with growth-friendly devices achieved better radiographic outcomes than primary spinal fusion [14]. Therefore, efforts should be devoted to appealing for early intervention of spinal deformities in Chinese SMA patients. Given the severe scoliosis in most cases, actual recumbent length could be undervalued, bringing about the overestimation of BMI. Therefore, percentage of patients with low weight might be underestimated. Since severe scoliosis may aggravate dysphagia and gastrointestinal dysfunction, longitudinal nutritional evaluation and reasonable intervention are recommended for SMA patients.
Among the 19 patients included, 17 had a preoperative MCCA exceeding 90°. Considering the severity of deformity and age at surgery, PSF was performed for all the patients. Multi-rod constructs were undertaken in 17 cases for better apical correction and global balance and a correction rate exceeding 50% was achieved for MCCA (Fig. 1). Compared with previous techniques, distal fixation with S2AI screws remarkably reduces the possibility of SSI and implant prominence with non-inferior biomechanical stability [15, 16]. However, the application of S2AI screws could be difficult in SMA patients with complex pelvic and hip situations. For instance, hip subluxation or luxation obviously limits the use of greater trochanter for the direction of S2AI screw insertion. Acetabular dysplasia also restricts the use of “teardrop” to identify the optimal S2AI trajectory. Also, iliac dysplasia is not uncommon in SMA. Iliac deformity leads to insufficient length and narrow diameter of S2AI trajectory and limits the size of screws. As reported by OʼBrien, S2AI screw of 65 mm was biomechanically equivalent to that of 80 mm in length [16]. As for diameter, screws ≥ 8 mm are recommended to reduce the risk of nail breakage [17]. In this cohort, screws with a length of 80 mm and a diameter of 8 mm via S2AI pathway were used in 10 of the 16 patients receiving sacropelvic fixation. The remaining 6 received screws with a length < 65 mm or a diameter < 8 mm owing to iliac dysplasia. These findings indicate the necessity of preoperative evaluation of pelvis development in SMA patients.

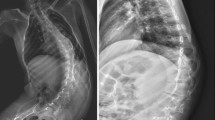
A 20-year-old female with SMA type III treated with posterior spinal fusion from T4 to pelvis. a–b: preoperative radiographs demonstrate a coronal Cobb angle of 132° (T7-L3), kyphosis of 129.6° (T3-L3) and pelvic obliquity of 28.3°. c–d: general observation shows severe kyphoscoliosis and sitting imbalance. e–f: postoperative radiographs demonstrate good surgical outcomes with Cobb angle of 62° (T7-L3), kyphosis of 42.3° (T3-L3) and pelvic obliquity of 11.9°, respectively. g–h: general observation shows an improvement of kyphoscoliosis and global balance
Multiple factors contribute to respiratory compromise in SMA. Despite the relatively intact function of diaphragm in SMA patients, their intercostal muscles are seriously affected [18]. Intercostal muscle weakness leads to parasol rib deformity and bell-shaped chest [19, 20]. Additionally, scoliosis induced by paraspinal muscle weakness may also reduce pulmonary function in a restrictive pattern. In this study, more than 60% patients developed scoliosis before 8 years old, when alveolar multiplication has not been accomplished. Therefore, it is possible that arrested development of alveoli could also be a contributor for pulmonary dysfunction in SMA. Efforts have been devoted to expanding space for lung via surgery to improve pulmonary function in SMA. Regarding spine-based distraction instruments, TGR was reported unable to prevent the progression of rib collapse [21]. Besides, despite the increase in FVC in SMA patients treated with TGR postoperatively, FVC% decreased over time [22]. Whether MCGR improves pulmonary function in SMA also remains controversial. Colombo and colleagues reported a stable FVC and FEV1 after MCGR implantation [23]. However, a reduction in FVC% was observed in SMA patients treated with MCGR or VEPTR [24]. Compared with MCGR or VEPTR only treatment, additional lateral chest wall support (CWS) significantly increases hemithorax width. Nevertheless, a 2-year follow-up indicated a reduction of FVC% in SMA patients with additional CWS, similar to that with MCGR or VEPTR only [24]. As reported by Holt et al., PSF increased HTH-concave without positive impact on SALR. Besides, PSF is supposed to delay the deterioration of pulmonary function despite failing to prevent rib collapse [25]. In this study, improvements were achieved in HTH-concave, HTH-convex and TTD postoperatively. Besides, SALR was increased. Inconsistency between our result and previous report in SALR change may be attributed to the greater preoperative difference between HTH-convex and HTH-concave in our cohort. Also, respiratory symptoms in SMA patients improved postoperatively though remarkable improvement on ventilation support usage had not yet been observed after spinal correction so far.
The classification of SMA is closely related to the severity of manifestations. Although no significant difference was found, average FEV1 and FVC were higher in type III group, reflecting the worse respiratory status in SMA type II patients. Besides, larger amount of EBL, longer lengths of ICU stay and intubation duration and higher incidence of complications were observed in type II group, though there was no statistical difference. These results correspond with the more efforts paid to the perioperative management of SMA type II patients.
A limitation of this study is inadequate follow-up. Accordingly, postoperative assessment of pulmonary function has not been accomplished. Besides, mechanical complication rate may be underestimated. Another limitation is the small sample size. As a result, patients with SMA type I were not included. Small sample size may also lead to data bias.
Conclusion
SMA patients from Mainland China are characterized by relative old age at scoliosis correction, high proportion of low weight and ubiquity of pulmonary dysfunction. PSF with S2AI technique is effective at the correction of severe spinal deformities, pelvic obliquity and thoracic morphology in SMA.
Data availability
The datasets generated during the current study are available from the corresponding author on reasonable request.
References
Lefebvre S, Burglen L, Reboullet S, Clermont O, Burlet P, Viollet L, Benichou B, Cruaud C, Millasseau P, Zeviani M et al (1995) Identification and characterization of a spinal muscular atrophy-determining gene. Cell 80:155–165. https://doi.org/10.1016/0092-8674(95)90460-3
Wijngaarde CA, Brink RC, de Kort FAS, Stam M, Otto LAM, Asselman FL, Bartels B, van Eijk RPA, Sombroek J, Cuppen I, Verhoef M, van den Berg LH, Wadman RI, Castelein RM, van der Pol WL (2019) Natural course of scoliosis and lifetime risk of scoliosis surgery in spinal muscular atrophy. Neurology 93:e149–e158. https://doi.org/10.1212/WNL.0000000000007742
Schwentker EP, Gibson DA (1976) The orthopaedic aspects of spinal muscular atrophy. J Bone Joint Surg Am 58:32–38
Sponseller PD, Yang JS, Thompson GH, McCarthy RE, Emans JB, Skaggs DL, Asher MA, Yazici M, Poe-Kochert C, Kostial P, Akbarnia BA (2009) Pelvic fixation of growing rods: comparison of constructs. Spine 34:1706–1710. https://doi.org/10.1097/BRS.0b013e3181ab240e
Lorenz HM, Badwan B, Hecker MM, Tsaknakis K, Groenefeld K, Braunschweig L, Hell AK (2017) Magnetically controlled devices parallel to the spine in children with spinal muscular atrophy. JB JS Open Access 2:e0036. https://doi.org/10.2106/JBJS.OA.17.00036
Abol Oyoun N, Stuecker R (2014) Bilateral rib-to-pelvis Eiffel Tower VEPTR construct for children with neuromuscular scoliosis: a preliminary report. Spine J 14:1183–1191. https://doi.org/10.1016/j.spinee.2013.07.484
Daher YH, Lonstein JE, Winter RB, Bradford DS (1985) Spinal surgery in spinal muscular atrophy. J Pediatr Orthop 5:391–395. https://doi.org/10.1097/01241398-198507000-00001
Chang TL, Sponseller PD, Kebaish KM, Fishman EK (2009) Low profile pelvic fixation: anatomic parameters for sacral alar-iliac fixation versus traditional iliac fixation. Spine 34:436–440. https://doi.org/10.1097/BRS.0b013e318194128c
Cederholm T, Bosaeus I, Barazzoni R, Bauer J, Van Gossum A, Klek S, Muscaritoli M, Nyulasi I, Ockenga J, Schneider SM, MA de van der Schueren Singer P (2015) Diagnostic criteria for malnutrition: an ESPEN consensus statement. Clin Nutr 34:335–340. https://doi.org/10.1016/j.clnu.2015.03.001
Zong XN, Li H (2013) Construction of a new growth references for China based on urban Chinese children: comparison with the WHO growth standards. PLoS ONE 8:e59569. https://doi.org/10.1371/journal.pone.0059569
Young MF, Nguyen P, Tran LM, Avula R, Menon P (2020) A double edged sword? Improvements in economic conditions over a decade in India led to declines in undernutrition as well as increases in overweight among adolescents and women. J Nutr 150:364–372. https://doi.org/10.1093/jn/nxz251
Corona J, Sanders JO, Luhmann SJ, Diab M, Vitale MG (2012) Reliability of radiographic measures for infantile idiopathic scoliosis. J Bone Joint Surg Am 94:e86. https://doi.org/10.2106/JBJS.K.00311
Obikili EN, Okoye IJ (2006) Transverse thoracic diameter in frontal chest radiographs of an adult Nigerian population. West Afr J Med 25:186–189. https://doi.org/10.4314/wajm.v25i3.28275
Hell AK, Braunschweig L, Tsaknakis K, von Deimling U, Luders KA, Hecker M, Lorenz HM (2020) Children with spinal muscular atrophy with prior growth-friendly spinal implants have better results after definite spinal fusion in comparison to untreated patients. Neurosurgery 87:910–917. https://doi.org/10.1093/neuros/nyaa053
Gao Z, Sun X, Chen C, Teng Z, Xu B, Ma X, Wang Z, Yang Q (2021) Comparative radiological outcomes and complications of sacral-2-alar iliac screw versus iliac screw for sacropelvic fixation. Eur Spine J 30:2257–2270. https://doi.org/10.1007/s00586-021-06864-7
O’Brien JR, Yu W, Kaufman BE, Bucklen B, Salloum K, Khalil S, Gudipally M (2013) Biomechanical evaluation of S2 alar-iliac screws: effect of length and quad-cortical purchase as compared with iliac fixation. Spine 38:E1250-1255. https://doi.org/10.1097/BRS.0b013e31829e17ff
Jain A, Hassanzadeh H, Strike SA, Menga EN, Sponseller PD, Kebaish KM (2015) Pelvic fixation in adult and pediatric spine surgery: historical perspective, indications, and techniques: AAOS exhibit selection. J Bone Joint Surg Am 97:1521–1528. https://doi.org/10.2106/JBJS.O.00576
Perez A, Mulot R, Vardon G, Barois A, Gallego J (1996) Thoracoabdominal pattern of breathing in neuromuscular disorders. Chest 110:454–461. https://doi.org/10.1378/chest.110.2.454
Alhammoud A, Othman Y, El-Hawary R, Mackenzie WG, Howard JJ (2021) The impact of scoliosis surgery on pulmonary function in spinal muscular atrophy: a systematic review. Spine Deform 9:913–921. https://doi.org/10.1007/s43390-021-00302-w
Fauroux B, Griffon L, Amaddeo A, Stremler N, Mazenq J, Khirani S, Baravalle-Einaudi M (2020) Respiratory management of children with spinal muscular atrophy (SMA). Arch Pediatr 27:7S29-27S34. https://doi.org/10.1016/S0929-693X(20)30274-8
McElroy MJ, Shaner AC, Crawford TO, Thompson GH, Kadakia RV, Akbarnia BA, Skaggs DL, Emans JB, Sponseller PD (2011) Growing rods for scoliosis in spinal muscular atrophy: structural effects, complications, and hospital stays. Spine 36:1305–1311. https://doi.org/10.1097/BRS.0b013e3182194937
Lenhart RL, Youlo S, Schroth MK, Noonan KJ, McCarthy J, Mann D, Hetzel S, Sund SA, Halanski MA (2017) Radiographic and respiratory effects of growing rods in children with spinal muscular atrophy. J Pediatr Orthop 37:e500–e504. https://doi.org/10.1097/BPO.0000000000000867
Colombo L, Martini C, Bersanini C, Izzo F, Villafane JH, Berjano P, Lamartina C (2020) Effects of magnetically controlled growing rods surgery on pulmonary function in young subjects with spinal muscular atrophy type 2 and other neuromuscular scoliosis. J Neurosurg Sci 64:253–257. https://doi.org/10.23736/S0390-5616.17.04052-8
Swarup I, MacAlpine EM, Mayer OH, Lark RK, Smith JT, Vitale MG, Flynn JM, Anari JB, Pediatric Spine Study G, Cahill PJ (2021) Impact of growth friendly interventions on spine and pulmonary outcomes of patients with spinal muscular atrophy. Eur Spine J 30:768–774. https://doi.org/10.1007/s00586-020-06564-8
Holt JB, Dolan LA, Weinstein SL (2017) Outcomes of primary posterior spinal fusion for scoliosis in spinal muscular atrophy: clinical, radiographic, and pulmonary outcomes and complications. J Pediatr Orthop 37:e505–e511. https://doi.org/10.1097/BPO.0000000000001049
Acknowledgements
We thank Huanhuan Sha from Jiangsu Cancer Hospital for language editing.
Funding
This study was funded by the National Natural Science Foundation of China (Grant Numbers: 81974354, 81772424).
Author information
Authors and Affiliations
Contributions
WC and JS contributed to conceptualization and project administration; ZW was involved in data curation, formal analysis, visualization and writing—original draft; JS contributed to funding acquisition; YJ was involved in methodology; and EF, YJ, JL and JZ contributed to writing—review and editing.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
Written informed consents for the use of data and pictures were obtained from adult patients or legal guardians.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wang, Z., Feng, E., Jiao, Y. et al. Surgical treatment of spinal deformities in spinal muscular atrophy: a single-center experience from China. Eur Spine J 31, 3089–3097 (2022). https://doi.org/10.1007/s00586-022-07347-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-022-07347-z