
Abstract
Purpose
To compare the clinical and radiographic outcomes of irreducible atlantoaxial dislocation (IAAD) treated with posterior fusion after anterior release and direct posterior reduction of the dislocation.
Methods
Online databases were searched for articles describing IAAD published from 1999 to 2015. Five studies (105 patients) described treatment with posterior fusion after periodontoid tissue release, and five studies (113 patients) described treatment with direct posterior reduction of the dislocation. The primary outcomes in this study were the complete reduction rate, Japanese Orthopedic Association score, perioperative morbidity, perioperative mortality, complications, vascular injury, and infection. Standard meta-analysis techniques were used to compare the outcomes.
Results
Of 319 citations examined, 10 articles involving 218 participants were eligible. Overall, there were no significant differences between the anterior release and posterior fixation (ARPF) group and direct posterior reduction and fixation (DPRF) group in the complete reduction rate, neurologic recovery rate, perioperative morbidity, perioperative mortality, vascular injury, or infection. However, the complication rate in the DPRF group was much lower than that in the ARPF group.
Conclusions
Compared with posterior fusion after anterior release, direct posterior reduction of the dislocation showed no significant differences in terms of the complete reduction rate, neurologic recovery rate, or fusion rate; however, it was a simpler process associated with less surgical trauma and a shorter operation time. Because of the limitations of the small sample in this study, whether direct posterior reduction of the dislocation is more effective and safer than posterior fusion after anterior release remains unclear.
Level of evidence
III.
Graphical abstract
These slides can be retrieved under Electronic Supplementary Material.

Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Atlantoaxial dislocation (AAD) is a potentially fatal disturbance to the normal atlantoaxial joints [1]. The craniovertebral junction can be affected by traumatic, inflammatory, idiopathic, or congenital abnormalities [2,3,4]. In some conditions, dislocation at C1–C2 is a dynamic process, and if timely treatment is not offered, the displacement may become fixed [5]. These dislocations are called irreducible AADs (IAADs); they are irreducible on dynamic X-ray even with skeletal traction under general anesthesia [1, 6]. There is not a clear and universal definition of the IAAD and multiple studies have used different criterion to define it.
Treatment of IAAD has traditionally been approached by transoral ventral decompression, but this is accompanied by high morbidity and mortality rates [7,8,9]. Single-stage anterior release followed by posterior occipitocervical/cervical fusion has been proposed to avoid odontoid resection [6]. Anterior release may be performed by a transoral or retropharyngeal approach [10, 11]. However, the incidence of complications associated with the transoral and retropharyngeal approaches is high, and there are many disadvantages such as increased hospitalization costs and a greater length of stay [12].
Studies involving direct posterior release and reduction of the dislocation for the treatment of IAAD have recently been reported [13,14,15,16,17,18,19]. This posterior-only approach can relieve the anterior compression of the spinal cord and medulla oblongata, while avoiding all risks of the transoral and retropharyngeal approaches.
We systematically reviewed all studies reporting the results of IAAD treatment and performed a meta-analysis to compare the results of series in which posterior fusion after anterior release and direct posterior reduction were performed. Specifically, we assessed the operative time, complete reduction rate, Japanese Orthopedic Association (JOA) score, perioperative morbidity, perioperative mortality, complications, vascular injury, and infection between the two techniques.
Materials and methods
Data source and search
The databases of PubMed, EMBASE, the Cochrane Library, Biological Abstracts, and Science Citation Index were carefully searched. The following keywords were used in both “AND” and “OR” combinations: “Atlantoaxial dislocation,” “Atlantoaxial subluxation,” “Basilar invagination,” “Irreducible,” “Reduction,” “Anterior release,” “Transoral surgery,” “Retropharyngeal anterior release,” “Instrumented fusion,” “Occipitocervical fusion,” and “Distraction.” The search was limited to articles published from 1999 to December 2015 in English. The references were also reviewed to identify additional relevant studies. All studies describing patients treated with one-stage anterior release and posterior fixation and fusion and direct posterior reduction were selected. The inclusion criteria were series of > 10 patients and data available on clinical and/or radiographic outcomes. The exclusion criteria were provision of insufficient information and series involving solely reducible dislocations. Patients who underwent transoral ventral decompression, posterior instrumented spinal fusion without reduction, or transoral atlantoaxial reduction plate fixation were also excluded. No review articles were included in this analysis.
Data extraction
The following information was extracted: data on the publication (name of first author, year of publication), patients (selection criteria, diagnoses, age, sex, length of follow-up), treatment technique (posterior fusion after transoral/retropharyngeal periodontoid tissue release or direct posterior reduction, fixed segment), and clinical outcomes (complete reduction rate, JOA score, neurologic recovery rate, perioperative morbidity, perioperative mortality, complications, vascular injury, infection, blood loss, operation time). The “good decompression” was determined as effective spinal cord decompression induced by the ectopic odontoid process on MRI, and the arachnoid space between the spinal cord and odontoid process could reappear. The follow-up period was ≥ 3 months ARPF.
Statistical analysis
The raw data were entered in Microsoft Excel (Office 2008 for Mac; SSPS Inc., Chicago, IL). Using the number of patients in each study with the available data and percentage of cases for each variable collected, weighted averages were calculated to determine the conglomerate values for all included studies. The Chi-square (χ2) test was used to compare proportions between the anterior release and posterior fixation (ARPF) group and direct posterior reduction and fixation (DPRF) group. All statistics were calculated with SSPS (v.17.0 for Mac; SSPS Inc.). Only mean values are reported for the following variables: age at surgery, estimated blood loss, operative duration, and follow-up duration. Thus, these variables were only semi-quantitatively compared. A fixed-effects model was used if there was no evidence of statistical heterogeneity among the studies. A random-effects model (Der Simonian and Laird) was used otherwise. All P values were two-sided, and a P value of < 0.05 was considered statistically significant. STATA 12.0 (Stata Corp LP, College Station, TX) and Review Manager 5.3 (The Cochrane Collaboration) were used to conduct the data analyses.
Results
Literature review
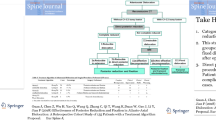
A flow chart showing the procedure for identifying the studies is presented in Fig. 1. In total, 319 articles were identified through the initial literature search, 262 of which were excluded by the title and abstract review because they were deemed not relevant to our study. Fifty-seven studies were reviewed in additional detail, 30 of which were excluded because they were either case reports or provided insufficient information. Seventeen studies were excluded because they dealt with posterior instrumented spinal fusion without reduction. Finally, 10 studies comprising 218 patients were included. Of note, in this analysis, we define the IAAD as abnormities on dynamic X-ray radiographs or failure of reduction during general anesthesia or preoperatively. There were no studies that reported on IAAD and were rejected because authors did not consider the study-defined IAAD in an acceptable format.

The literature search and selection of articles
Baseline characteristics and quality assessment of included studies
In total, 10 studies involving 218 patients were included. One hundred and five patients (48.2%) were treated with ARPF, and 113 patients (51.8%) were treated with DPRF. Their clinical characteristics and surgical outcomes are listed in Tables 1 and 2, respectively. Table 3 summarizes the differences in baseline characteristics and the postoperative outcomes of patients who underwent ARPF (n = 105) and DPRF (n = 113) for treatment of IAAD. No significant differences were found between the two groups in terms of age (P = 0.561), the incidence of os odontoideum (P = 1.000), the incidence of rheumatoid arthritis (P = 1.000), or the performance of occiput (Oc)–C2 fusion (P = 0.124).
We used the Newcastle–Ottawa Quality Assessment Scale to assess the quality of each study. Of the studies, three scored 8 points and one scored 7 points. Hence, the quality of the studies was relatively high (Table 2).
Comparison of ARPF and DPRF groups
The predominant diagnosis for IAAD in both groups was basilar invagination (77.0% in the DPRF group vs. 58.1% in the ARPF group; P < 0.0001). A significantly greater proportion of patients in the ARPF than DPRF group had odontoid fractures (22.9% vs. 7.0%; P = 0.001).
All studies provided JOA scores, complete reduction rates, and solid fusion rates in detail. Overall, there were no significant differences between the ARPF and DPRF groups in the complete reduction rate [80.0% (95% confidence interval (CI) 72.35–87.65%) vs. 84.1% (95% CI 77.32–90.82%); P = 0.482] (Fig. 2), partial reduction rate [20.0% (95% CI 12.35–27.65%) vs. 15.93% (95% CI 9.18–22.68%); P = 0.482] (Fig. 3), neurologic recovery rate [96.6% (95% CI 92.88–100.38%) vs. 96.6% (95% CI 91.78–99.37%); P = 0.100] (Fig. 4), perioperative morbidity [0.0% (95% CI 0.0–0.0%) vs. 0.0% (95% CI 0.0–0.0%); P = NS], perioperative mortality [0.0% (95% CI 0.0–0.0%) vs. 1.77% (95% CI − 0.66 to 4.20%); P = 0.498], solid fusion rate [100% (95% CI 100–100%) vs. 100% (95% CI 100–100%); P = NS], vascular injury [0.0% (95% CI 0.0–0.0%) vs. 1.77% (95% CI − 0.66 to 4.20%); P = 0.498], or infection [0.95% (95% CI − 0.91 to 2.81%) vs. 2.65% (95% CI − 0.31 to –5.62%); P = 0.623]. However, the complication rate in the DPRF group was much lower than that in the ARPF group [3.5% (95% CI 0.13–6.95%) vs. 11.4% (95% CI 5.34–17.51%); P = 0.036], and the rate of good decompression on magnetic resonance imaging (MRI) in the DPRF group was higher than that in the ARPF group [99.1% (95% CI 97.39–100.84%) vs. 92.7% (95% CI 87.05–98.32%); P = 0.043] (Fig. 5).

Forest plots in issues of complete reduction rate. a For ARPF group; b for DPRF group

Forest plots in issues of partial reduction rate. a For ARPF group; b for DPRF group

Forest plots in issues of neurological recovery rate. a For ARPF group; b for DPRF group

Forest plots in issues of the rates of MRI good decompression. a For ARPF group; b for DPRF group
Solid fusion was achieved in all patients in both groups. Moreover, C1–C2 fusion was more commonly performed in the DPRF cohort (53.1% vs. 30.5%; P = 0.001), whereas Oc–C3 fusion was more commonly performed in the ARPF group (25.7% vs. 2.7%; P < 0.001). A greater proportion of patients in the ARPF group had fusions that incorporated the Oc or subaxial regions of the spine.
Perioperative mortality was rare (ARPF, 0.0% vs. DPRF, 1.7%) and occurred with a similar incidence in both groups (P = 0.498). One death in the DPRF group was secondary to vertebral artery injury. The other death was only indirectly related to the surgery in the DPRF group (during surgery, the patient’s blood pressure suddenly fell along with T-wave changes). Unexpected neurological morbidity did not occur in either group. All studies reported the surgery-related complications. The incidence of complications was significantly higher in the ARPF than DPRF group [11.4% (95% CI 5.34–17.51%) vs. 3.5% (95% CI 0.13–6.95%); P = 0.036]. Although reported in some studies, we should note that some postoperative symptoms could not be considered as complication of a transoral procedure. These are unavoidable given the approach, like dysphagia, hoarseness, and nasal phonation. There symptoms were anterior release related. The details of each complication or transoral procedure-related postoperative issues are shown in Table 3.
Data concerning estimated blood loss were reported in 73.5% and 31.0% of patients in the ARPF and DPRF groups, respectively. Blood loss was higher in ARPF than DPRF surgeries (510 vs. 364 mL). Data concerning the operative duration were reported in 23.3 and 31.0% of patients in the ARPF and DPRF groups, respectively. The mean operative duration was longer in ARPF than DPRF surgeries (258 vs. 110 min). Surgical trauma was less severe and manipulation was simper in the DPRF than ARPF group.
The mean follow-up times from operation for both groups were comparable (29.7 vs. 16.49 moths).
Meta-analysis of complete reduction rate, neurologic recovery rate, and complication rate
Figures 2 and 3 show forest plots illustrating the point estimates and 95% CIs for the rates of complete reduction and partial reduction in the ARPF and DPRF groups. The proportion of patients who achieved complete reduction was similar in the DPRF and ARPF groups [80.0% (95% CI 72.35–87.65%) vs. 84.1% (95% CI 77.32–90.82%); P = 0.482]. Q-testing confirmed heterogeneity between the study groups (P < 0.001).
Figure 4 shows a forest plot illustrating the point estimates and 95% CIs for the rates of neurologic recovery in the ARPF and DPRF groups. The estimated rate of clinical neurologic recovery was similar in the DPRF and ARPF groups [96.6% (95% CI 92.88–100.38%) vs. 96.6% (95% CI 91.78–99.37%); P = 0.100] (Fig. 3). Q-testing revealed no significant heterogeneity between the study groups (P < 0.001).
Figure 5 shows a forest plot illustrating the point estimates and 95% CIs for the rates of good decompression on MRI in the ARPF and DPRF groups. The rate of good decompression on MRI was higher in the DPRF than ARPF group [99.1% (95% CI 97.39–100.84%) vs. 92.7% (95% CI 87.05–98.32%); P = 0.043].
Forest plots were not drawn for the complication rates in the ARPF and DPRF groups because the data were limited; there was no mortality, morbidity, or vascular injuries in the ARPF group; and there was no morbidity in the DPRF group. As shown in Table 3, the complication rate was much lower in the DPRF than ARPF group [3.5% (95% CI 0.13–6.95%) vs. 11.4% (95% CI 5.34–17.51%); P = 0.036].
The effects of each single study were evaluated using sensitivity analysis, in which each study was taken out of consideration during the assessment. The outcome of the sensitivity analyses suggested a statistically robust result (Fig. 6).

Sensitivity analyses plots. a For complete reduction rate of ARPF group. b For complete reduction rate of DPRF group. c For partial reduction rate of ARPF group. d For partial reduction rate of DPRF group
Figure 7 shows the funnel plots for certain comparisons involved in this meta-analysis. Because the plots were generally symmetrical, no statistically significant publishing bias was detected.

Funnel plots to evaluate the publishing bias. a For complete reduction rate of ARPF group. b For complete reduction rate of DPRF group. c For partial reduction rate of ARPF group. d For partial reduction rate of DPRF group. e For neurological recovery rate of ARPF group. f For neurological recovery rate of DPRF group
Discussion
This meta-analysis demonstrated that both one-stage anterior release followed by posterior internal fixation and direct posterior release of the facets and reduction of the dislocation are effective in the treatment of IAAD. Both techniques resulted in high complete reduction rates and similarly low morbidity and mortality rates.
AAD has been described as irreducible when dynamic X-rays demonstrate no reduction of the dislocation on full-neck extension or with cervical traction [20]. Some researchers recently proposed a novel classification system in which IAAD is defined as both a failed attempt at reduction using skeletal traction performed under general anesthesia and the presence of muscle paralysis [21]. The traditional treatment procedure for IAAD reported in the literature is posterior fusion after transoral odontoidectomy [7]. However, despite advances in microsurgical techniques, these transoral or transmaxillary decompression approaches have shown a high incidence of mortality, morbidity, and complications such as cerebrospinal fluid leakage, infection, and abscess formation [22, 23]. Wang et al. [6] proposed one-stage anterior transoral release followed by posterior internal fixation. This anterior release procedure could bring down the odontoid and relieve the ventral cord compression with less invasiveness. However, complications associated with the anterior approach are still inevitable.
The transoral route is the gold standard for odontoid resection. Results are satisfying though surgery can be challenging for patients and surgeons due to its invasiveness. A less invasive transnasal approach could also provide a sufficient extent of resection with less collateral damage. The technique of transnasal endoscopic odontoid resection is demonstrated in plenty of modern literatures on endoscopic transnasal odontoid resection followed by posterior fixation, which seems to become one of the standards of care of IAAD in some countries. The transoral-endoscopic or non-endoscopic-approach is one of the most commonly used approaches for the odontoid resection. Gempt et al. demonstrated a case series of three patients undergoing transnasal endoscopic odontoid resection. In their study, a fully endoscopic transnasal odontoid resection was conducted with the use of CT-based neuronavigation. A complete odontoid resection succeeded in all the three patients. Symptoms such as tetraparesis, neck pain, myelopathic gait disturbances, salivary retention, swallowing disturbance, and dysarthria improved in all patients markedly [24]. As such, transnasal endoscopic odontoid resection seems to be a feasible alternative to the transoral technique. However, considering the transoral or transnasal approach unavoidable related issues like dysphagia and sore throat post operatively, recently, the treatment trend has shifted from traditional anterior release/decompression and posterior fusion to direct posterior release and reduction of the dislocation [17,18,19]. After all, theoretically, if the spinal cord could be decompressed effectively and sufficiently, the clinical improvement of symptoms is deserved to be equally satisfying for both these two surgical methods. Goel et al. [14] proposed that irreducible dislocations can be reduced by distraction of the facet joints via the posterior approach. With the introduction of this technique, the differentiation between irreducible and reducible AAD became blurred because many so-called IAADs could be realigned by intraoperative posterior distraction and reduction. Jian et al. [16] proposed that the force exerted on the screws by intraoperative distraction acts directly on the dislocated joint; this force is much larger than that of cervical traction under general anesthesia and is enough to perform the reduction. Although contracted tissues may be present at the front (anterior longitudinal ligament, alar and apical ligaments) [25, 26], the effect of reduction is not resisted. The present study revealed no difference in the complete reduction rates between the ARPF and DPRF groups.
When dynamic X-rays demonstrate no reduction, different intraoperative or preoperative approaches are utilized to attempt reduction via traction. Some researchers have applied preoperative traction over a longer period of time without muscle curarization or general anesthesia to slowly reduce the dislocation; however, this may be a long and painful process [27]. Some surgeons choose to apply skeletal traction with the patient under general anesthesia for rapid reduction before one-stage fixation [6, 28]. However, these procedures are also time-consuming, surgically complex, and technically demanding. Moreover, the intraoperative lateral perspective of the C-arms is always too obscure to distinguish the reduction especially for people with basilar invagination. If the posterior distraction–reduction technique can achieve complete reduction for most IAADs, the classification mode of “irreducible” and “reducible” established based on the consequence of skeletal traction performed under general anesthesia might be inappropriate. The necessity of preoperative or intraoperative traction should be reconsidered.
With the advancements in instrumentation techniques, several posterior distraction–reduction techniques have become available for IAAD. Abumi et al. [13] reported 26 patients with AAD associated with basilar invagination who underwent reduction using a distraction technique between the Oc and C2 pedicle screws. Goel et al. [14] dissected the C1–C2 facet joints and inserted a spacer bilaterally under cervical traction to achieve reduction. Yin et al. [19] reported that reduction occurred when the implanted screws and rods between C1 and C2 acted as a lever system, drawing C1 backward and pushing C2 downward and forward. Suh et al. [18] designed two types of a simple tool to facilitate AAD reduction after individual screw placement. Chandra et al. [15] described a technique involving distraction compression and reduction.
Limitations
This study has several limitations. First, it was limited by the small number of single-center series and its reliance on retrospectively collected data. Moreover, the clinical and demographic data were either missing or could not be disaggregated in some studies. Second, there is no universally adopted definition of irreducible. Various classification systems exist but have not been universally adopted. Some studies of DPRF define irreducible as no reduction of the dislocation on full-neck extension dynamic X-rays or with cervical traction. However, most studies of ARPF define irreducible as a failed attempt at reduction using skeletal traction performed under general anesthesia. Some IAADs treated with DPRF might be reducible under general anesthesia; however, these cases were not excluded, possibly resulting in an overestimation of the true complete reduction rate in the DPRF group of the present analysis. Third, decisions about the treatment of IAAD depend on multiple factors including the etiology of AAD, the orientation of the C1–C2 facets, and the adjacent vertebral malformation, all of which affect the feasibility of treatment. Patient selection and publication bias could not be avoided. Finally, there are no universally adopted criteria with which to assess anatomic reduction or to determine which imaging modality is optimal. The atlantodental interval measured on the mid-sagittal computed tomography scan, the shape of the C1–C2 facet joint, and the cervicomedullary angle may all have impacted the surgical outcomes.
Nevertheless, this meta-analysis serves as the first attempt to compare these two techniques and includes > 200 patients, providing some initial conclusions regarding the safety and efficacy of these two techniques. Randomized, prospective studies with validated outcome measures are required to support our conclusions. The decision of whether to perform ARPF or DPRF for treatment of AAD must be made on an individual basis and should depend on the experience and comfort of the surgeon and the unique anatomic considerations of the patient.
Conclusions
Compared with posterior fusion after anterior release, direct posterior reduction of dislocation showed no significant differences in terms of the complete reduction rate, postoperative JOA score, or fusion rate; however, it was a simpler process that induced less surgical trauma and had a shorter operation time. If posterior distraction–reduction can achieve complete reduction for most IAADs, the classification mode of “irreducible” and “reducible” established based on the consequence of skeletal traction or dynamic X-ray might be inappropriate. The necessity of preoperative or intraoperative traction should be reconsidered. Because of the limitations of the small sample in this study, whether direct posterior reduction of the dislocation is more effective and safer than posterior fusion after anterior release remains unclear.
References
Yang SY et al (2014) A review of the diagnosis and treatment of atlantoaxial dislocations. Glob Spine J 4:197–210
Venkatesan M et al (2012) Traumatic atlantoaxial rotatory subluxation (TAARS) in adults: a report of two cases and literature review. Injury 43:1212–1215
Menezes AH et al (1980) Craniocervical abnormalities. A comprehensive surgical approach. J Neurosurg 53:444–455
Bouchaud-Chabot A, Liote F (2002) Cervical spine involvement in rheumatoid arthritis. A review. Joint Bone Spine 69:141–154
Salunke P et al (2011) Congenital atlantoaxial dislocation: a dynamic process and role of facets in irreducibility. J Neurosurg Spine 15:678–685
Wang C et al (2006) Open reduction of irreducible atlantoaxial dislocation by transoral anterior atlantoaxial release and posterior internal fixation. Spine (Phila Pa 1976) 31:E306–E313
Subin B et al (1995) Transoral anterior decompression and fusion of chronic irreducible atlantoaxial dislocation with spinal cord compression. Spine (Phila Pa 1976) 20:1233–1240
Dickman CA et al (1992) The influence of transoral odontoid resection on stability of the craniovertebral junction. J Neurosurg 77:525–530
Hwang SW et al (2008) C1–C2 arthrodesis after transoral odontoidectomy and suboccipital craniectomy for ventral brain stem compression in Chiari I patients. Eur Spine J 17:1211–1217
Hao D et al (2016) Single-stage anterior release and sequential posterior fusion for irreducible atlantoaxial dislocation. Clin Spine Surg 29:E240–E245
Srivastava SK et al (2016) Single-stage anterior release and posterior instrumented fusion for irreducible atlantoaxial dislocation with basilar invagination. Spine J 16:1–9
Laheri V et al (2015) Anterior transoral atlantoaxial release and posterior instrumented fusion for irreducible congenital basilar invagination. Eur Spine J 24:2977–2985
Abumi K et al (1999) Posterior occipitocervical reconstruction using cervical pedicle screws and plate-rod systems. Spine (Phila Pa 1976) 24:1425–1434
Goel A et al (2005) Reduction of fixed atlantoaxial dislocation in 24 cases: technical note. J Neurosurg Spine 2:505–509
Chandra PS et al (2013) Distraction, compression, and extension reduction of basilar invagination and atlantoaxial dislocation: a novel pilot technique. Neurosurgery 72:1040–1053
Jian FZ et al (2010) Direct posterior reduction and fixation for the treatment of basilar invagination with atlantoaxial dislocation. Neurosurgery 66(678–687):687
Salunke P et al (2015) Technique for direct posterior reduction in irreducible atlantoaxial dislocation: multi-planar realignment of C1–2. Clin Neurol Neurosurg 131:47–53
Suh BG et al (2013) A new technique for reduction of atlantoaxial subluxation using a simple tool during posterior segmental screw fixation: clinical article. J Neurosurg Spine 19:160–166
Yin YH et al (2013) Posterior realignment of irreducible atlantoaxial dislocation with C1–C2 screw and rod system: a technique of direct reduction and fixation. Spine J 13:1864–1871
Greenberg AD (1968) Atlanto-axial dislocations. Brain 91:655–684
Wang S et al (2013) Novel surgical classification and treatment strategy for atlantoaxial dislocations. Spine (Phila Pa 1976) 38:E1348–E1356
Qiuhang Z et al (2013) Transoral endoscopic odontoidectomy to decompress the cervicomedullary junction. Spine (Phila Pa 1976) 38:E901–E906
Dlouhy BJ et al (2015) Evolution of transoral approaches, endoscopic endonasal approaches, and reduction strategies for treatment of craniovertebral junction pathology: a treatment algorithm update. Neurosurg Focus 38:E8
Gempt J et al (2011) Endoscopic transnasal resection of the odontoid: case series and clinical course. Eur Spine J 20:661–666
Radcliff K et al (2012) CT and MRI-based diagnosis of craniocervical dislocations: the role of the occipitoatlantal ligament. Clin Orthop Relat Res 470:1602–1613
Kingdom TT et al (1995) Transoral-transpharyngeal approach to the craniocervical junction. Otolaryngol Head Neck Surg 113:393–400
Nordt JC, Stauffer ES (1981) Sequelae of atlantoaxial stabilization in two patients with Down’s syndrome. Spine (Phila Pa 1976) 6:437–440
Hedequist D et al (2010) Single stage reduction and stabilization of basilar invagination after failed prior fusion surgery in children with Down’s syndrome. Spine (Phila Pa 1976) 35:E128–E133
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Guan, J., Chen, Z., Wu, H. et al. Is anterior release and cervical traction necessary for the treatment of irreducible atlantoaxial dislocation? A systematic review and meta-analysis. Eur Spine J 27, 1234–1248 (2018). https://doi.org/10.1007/s00586-018-5563-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-018-5563-7