
Abstract
Purpose
Chronic low back pain and lumbar spinal stenosis (LSS) seem to deteriorate lumbar muscle function and proprioception but the effect of surgery on them remains unclear. This study evaluates the effect of decompressive surgery on lumbar movement perception and paraspinal and biceps brachii (BB) muscle responses during sudden upper limb loading in LSS.
Methods
Low back and radicular pain intensity (VAS) and Oswestry Disability Index (ODI) were measured together with lumbar proprioception and paraspinal and BB muscle responses prior to and 3 and 24 months after surgery in 30 LSS patients. Lumbar proprioception was assessed by a previously validated motorized trunk rotation unit and muscle responses for sudden upper limb loading by surface EMG.
Results
Lumbar perception threshold improved after surgery during 3-month follow-up (from 4.6° to 3.1°, P = 0.015) but tend to deteriorate again during 24 months (4.0°, P = 0.227). Preparatory paraspinal and BB muscle responses prior to sudden load as well as paraspinal muscle activation latencies after the load remained unchanged.
Conclusion
Impaired lumbar proprioception seems to improve shortly after decompressive surgery but tends to deteriorate again with longer follow-up despite the sustaining favorable clinical outcome. The surgery did not affect either the feed-forward or the feed-back muscle function, which indicates that the abnormal muscle activity in LSS is at least partly irreversible.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
LSS patients have been previously shown to have impaired feed-forward control of the trunk muscles [9]. This controlling mechanism refers to the activity of the central movement control system maintaining postural stability and preparing the trunk to bear a potentially increasing load by activating certain trunk muscles [6]. Adequate movement sensation and muscular control are essential in preventing low back injury and falls, especially among the elderly. Abnormal trunk muscle activation for sudden perturbations has been observed in LBP patients and delayed reflex responses are considered as a risk factor for low back injury [3]. Active physical rehabilitation has been shown to improve trunk muscle activation functions in LBP [13].
Impaired lumbar proprioception has been observed previously in chronic non-specific LBP [16], sciatica [12], and LSS patients [9]. Postoperative rehabilitation after decompressive surgery may improve functional outcome [1], whereas the effect of decompressive surgery on paraspinal muscle responses and lumbar proprioception has not been evaluated previously in patients with LSS.
In this study, we assessed the effect of decompressive surgery on paraspinal and biceps brachii muscle activation during sudden upper limb loading and lumbar movement perception in LSS patients.
Materials and methods
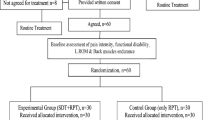
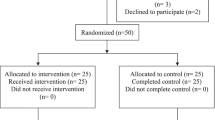
The study included 30 patients with LSS (12 males and 18 females) described previously [9]. Briefly, the patients were recruited from the Departments of Orthopedic Surgery and Neurosurgery of the Kuopio University Hospital, where they were selected for decompression surgery due to lumbar spinal stenosis. All patients had both clinically and radiologically diagnosed LSS. Surgeon, in consensus with patient, made the decision to treat the patient operatively. The patients underwent decompressive surgery performed by an orthopedic surgeon or neurosurgeon. The operations were performed between December 2001 and May 2003. 24 patients were treated with total laminectomy; one lamina in 13 patients, 2 laminas in 10 patients and 3 laminas in 1 patient. Five patients were treated with hemilaminectomy (1 lamina in 4 patients and 2 laminas in 1 patient) and one patient with laminotomy. The most frequently operated levels were L3/4 and L4/L5. Concomitant disc herniation was extirpated in two patients during decompression. One patient had posterolateral fusion in situ with autograft bone after laminectomy L3 and L4. Baseline measurements were done prior to the surgery and follow-up measurements at 3 and 24 months after the surgery. The use of prescribed drugs was registered: 28 patients used either NSAIDs or paracetamol, or both of them. Patients with clinically symptomatic spondylolysis or spondylolisthesis were excluded. The study was approved by the Kuopio University Hospital Research Ethics Board and it was performed according to the Declaration of Helsinki.
Pain intensity was determined by Visual Analog Scale (0–10 VAS). Functional disability was assessed by the Oswestry Disability Index (OSW) [5]. Depressive symptoms were evaluated by using the 21-item Beck Depression Inventory (BDI-21) [2] (Table 1).
Lumbar movement perception
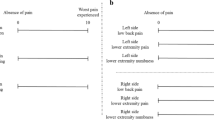
Lumbar proprioception was assessed in an earlier demonstrated trunk rotation measurement unit (DBC International Ltd, Helsinki, Finland) [16], which targeted the rotation on the lumbar/thoracic spine. The test was identical with the previous studies [11]. In the test, the subject was placed in the device in a seated position, ears and eyes covered, while the seat was rotated with an angular velocity of 1o/s and the subject indicated the initiation of the movement by releasing a finger switch. The magnitude of the lumbar rotation was recorded. In addition, the subject was asked to indicate the direction of the movement. The results of five consecutive trials were pooled.
Muscle responses
Paraspinal and biceps brachii muscle responses for unexpected (eyes closed) and expected (eyes open) upper limb loading were measured by a previously described protocol [12]. During the procedure, the subject was standing and holding a box in the hands while a weight of 1.0 kg was suddenly dropped from the height of the subject’s eyes into the box equipped with a marker switch indicating the impact moment. Twelve consecutive measurements were performed in sequences of three trials with eyes open and three with eyes closed in supported (first six) and unsupported (last six) standing positions. Bipolar surface electromyography (EMG) was recorded bilaterally over the paraspinal muscles at L5-S1 levels by a four-channel ME 3000P EMG system (Mega Electronics Ltd, Kuopio, Finland) with disposable Ag/AgCl surface electrodes (Medicotest, Olstykke, Denmark). The electrode placements at paraspinal muscles L5-S1 level were similar with previous study [9]. A pair of 10-cm-long cables connected the electrodes to the preamplifier in each EMG channel. The preamplifier was secured by attaching it to the corresponding reference electrode. A pair of 2.5-m-long cables connected the preamplifier to the amplifier box. The raw EMG signal was recorded at the sampling rate of 2 kHz and band-pass filtered between 7 and 500 Hz with an analog filter, amplified (differential amplifier, CMRR >110 dB, gain 1000, noise <1 V), analog-to-digital converted (12-bit), and stored in a personal computer for later analysis.
The muscle activation onsets and offsets were determined visually from the rectified EMG. The determination was made without reference points to exclude observer bias. The latencies are presented with respect to the trigger in the bottom of the box. In addition, the BB and paraspinal muscle activity levels were obtained from 200 ms duration prior to the impact of the load. The activity level was normalized according to the activity of the first trial. The results from three repeated trials were pooled for statistical analysis.
Statistical analysis
A mixed model analysis was used to analyze the effects of surgery on the short latency responses of paraspinal muscles and preparatory muscle activation and lumbar movement perception with ODI, VAS and BDI. The results in the follow-ups were compared using a mixed model, based on the linearly independent pairwise comparisons among the estimated marginal means. The statistical analyses were performed with SPSS 19.0 software (SPSS, Chicago, IL) and statistical significance was set as P < 0.05.
Results
The threshold to detect rotation decreased in 3-month follow-up after surgery (4.6 ± 2.3 vs. 3.1° ± 1.7°, P = 0.015) but tended to deteriorate again for 2-year follow-up (4.0 ± 2.6, P = 0.227, Fig. 1).

The measurements for the sensation of a change in lumbar position at baseline, 3- and 24-month follow-ups. Five consecutive trials are pooled. Error bars are standard deviations
Paraspinal muscle activation latencies after the unexpected and expected load remained unchanged in 3-month follow-up but for expected load prolonged in 2-year follow-up (P = 0.031). Expectation decreased the paraspinal muscle latencies similarly at baseline and in 3-month follow-up (10.0 ± 2.1 ms and 11.8 ± 2.2 ms, respectively, P < 0.001) and also in 2-year follow-up (6.5 ± 2.2 ms, P < 0.023) Fig. 2.

Paraspinal muscle reflex latencies at baseline, 3- and 24-month follow-ups. Six trials with eyes closed (a) and six trials with eyes open (b), respectively, are pooled for each group. Error bars are standard deviations
At baseline anticipation increased preparatory paraspinal (9 ± 3 %, P < 0.001) (Fig. 3a) and BB (68 ± 18 %, P < 0.001) (Fig. 3b) muscle activity. The surgery did not affect the BB or paraspinal muscle activation in 3-month follow-up, but during 2-year follow-up the preparatory BB activation decreased in unexpected (−22 ± 5 %, P < 0.001) and in expected (−56 ± 13 %, P < 0.001) upper limb loading and the effect of expectation vanished (P < 0.001).

Normalized paraspinal (a and b) and biceps brachii (c and d) activity levels prior to perturbation at baseline, 3- and 24-month follow-ups. Six trials with eyes closed and six trials with eyes open, respectively, are pooled for each group. Error bars are standard deviations
In 3 months after surgery VAS was decreased by 60 ± 4 % (P < 0.001) from baseline and in 2 years it tended to increase (21 ± 3 %, P = 0.711) from the 3-month result. ODI decreased −42 ± 3 % (P < 0.001) in 3 months postoperatively and remained steady at 2 years, 0 ± 3 % (P = 0.001). Only weak insignificant correlations were found between subjective questionnaire data and the degree of lumbar rotation or BB muscle activation. (Table 2A, B)
Discussion
This study shows that lumbar proprioception improved after decompression surgery, but the impaired feed-forward and paraspinal reflex control did not recover after the operation. Also, the threshold to detect lumbar movement remained higher after surgery (about 3°) than among healthy subjects (about 1°) [16]. Moreover, lumbar proprioception seems to deteriorate again in longer follow-up. Upper limb preparatory activation decreased in 2-year follow-up and the effect of expectation disappeared. These findings indicate that the impaired motor control of LSS patients does not automatically recover with 2-year follow-up despite considerable pain and disability relief but rather further deteriorate during the 2-year follow-up.
Lumbar movement perception impairments in LSS have been shown earlier [9, 10], but the effect of decompressive surgery on lumbar movement perception has not been studied before. Current study clarifies the effect of decompressive surgery in a 2-year follow-up time period. The short-term effect of surgery for lumbar movement perception seems to be similar in LSS and disc herniation [11]. In the previous study on disc herniation, the follow-up was restricted to 3 months and importantly we find now that at least in LSS this effect seems to dilute by longer follow-up time. It should be remembered that LSS patients are usually older, degeneration more advanced and symptoms more chronic from those seen in disc herniation. There are several potential explanations for the lumbar movement perception differences seen between the current results in LSS and previous results in chronic low back pain (CLBP) like disruption of local nervous and muscular tissues, which is usually more severe in LSS than CLBP. Also, the patients with LSS have both leg and back pain, while patients with CLBP usually have only back pain.
Previous studies in non-operatively [4] and operatively [4] treated sciatica patients indicated that the recovery of impaired muscle performance was not a matter of course at the 6-month follow-up. The impaired feed-forward and paraspinal reflex control did not recover even at 2 years after the operation in the present study. This suggests the mechanisms may be impaired permanently; second, at least some of the changes in muscle function may be adaptive in nature [4].. Evaluation of the effect of postoperative rehabilitation on postural control would help in clarifying this issue.
In the present study, LSS patients had long paraspinal muscle reflex latencies both in unexpected and expected conditions which remained unchanged after decompressive surgery in a 2-year follow-up. Remaining low back pain alongside with probably irreversibly disrupted spinal muscle control could be the issue. We have seen similar results in anticipated sudden loading between controls and LSS patients [9]. It seems that decompressive surgery has no effect on reflex activation, even though pain and disability scores improve significantly. The effect of rehabilitation procedures should be tested in further studies.
The increased biceps brachii muscle activation prior to load perturbation in expected loading trials is in line with the previous observations seen in similar setting in CLBP patients [10], in LSS [9] and in self-initiated loading [14]. The significant decrease in these activation patterns in follow-up is a novel finding. The preparatory upper limb activation and the increased paraspinal muscle activation refer to the feed-forward mechanism, preparing the trunk for becoming perturbation. The decline in these preparatory muscle activations in LSS patients indicates impaired feed-forward control, which supports the previous findings seen in experimental pain [7] and in chronic LBP patients during sudden upper limb loading [10]. Disturbances in this feed-forward mechanism can alter higher level information processing and thus deteriorating motor control beyond spine. It has also been suggested that during voluntary activation transient experimental muscle pain has a limited effect on central motor pathways [8]. Chronic pain has also been shown to lead to reduction in corticospinal drive to the legs making the patient more vulnerable to physical perturbation [15] and decreased neural drive to the back muscles has been observed during high levels of voluntary contractions [17].
The patients in this study underwent a decompression surgery and represented a specific condition of chronic low back syndrome of LSS. Thus, they were a group of patients suffering considerable pain and disability and enjoying major relief of pain and disability after surgery. The reliability and validity of the methods used in this study have been demonstrated previously [9]. These results increase our knowledge of the extensive changes in sensory motor control of lumbar spine in LSS and have direct impact on planning specific rehabilitation procedures to be tested clinically. However, the differences in paraspinal muscle activation levels and response latencies are rather small and therefore their clinical significance is expected to be rather limited. The limitations of the study include the relatively small sample size. Since the follow-up included measurements only at 3 and 24 months, our results are not able to reveal the pace of changes in proprioception between these time points, which must be considered as a weakness as well. Also, a longer follow-up time than 24 months would have been desirable. Parameters like lumbar lordosis and sagittal balance were not evaluated in this study and would be worthwhile to take into account in the further studies. Also, correlation of lumbar proprioception and reflex control to clinical outcome of these patients seems to be limited and still requires further study including morphology of paraspinal muscles.
In conclusion, the results indicate that after decompressive surgery, lumbar proprioception improves but paraspinal and biceps brachii muscle activation profiles tend to remain unchanged. Moreover, during 2-year follow-up after surgery both lumbar proprioception and muscle activation profiles tended to further deteriorate despite the sustaining favorable clinical outcome. Decompressive surgery does not restrict degeneration or stenotic progress. Stenosis keeps progressing during the 2-year follow-up and this potentially causes new neural tissue problems. This is again proof for degeneration and irreversible local changes in muscles and in muscle control mechanisms. Our results indicate that changes in proprioception and paraspinal muscle activation due to LSS are at least partly irreversible, despite successful clinical outcome of the surgery.
References
McGregor AH, Probyn K, Cro S et al (2013) Rehabilitation following surgery for lumbar spinal stenosis. Cochrane Database Syst Rev 12:CD009644
Beck AT, Ward CH, Mendelson M et al (1961) An inventory for measuring depression. Arch Gen Psychiatry 4:53–63
Cholewicki J, Silfies SP, Shah RA et al (2005) Delayed trunk muscle reflex responses increase the risk of low back injuries. Spine 30:2614–2620
Dubourg G, Rozenberg S, Fautrel B et al (2002) A pilot study on the recovery from paresis after lumbar disc herniation. Spine 27:1426–1431
Fairbank JCT, Couper J, Davies J, O’Brien JP (1980) The Oswestry low back pain disability questionnaire. Physiotherapy 66:271–273
Hodges P, Cresswell A, Thorstensson A (1999) Preparatory trunk motion accompanies rapid upper limb movement. Exp Brain Res 124:69–79
Hodges PW, Moseley GL, Gabrielsson A, Gandevia SC (2003) Experimental muscle pain changes feedforward postural responses of the trunk muscles. Exp Brain Res 151:262–271
Khan SI, McNeil CJ, Gandevia SC, Taylor JL (2011) Effect of experimental muscle pain on maximal voluntary activation of human biceps brachii muscle. J Appl Physiol 111(3):743–750
Kääriäinen T, Leinonen V, Taimela S et al (2013) Lumbar paraspinal and biceps brachii muscle function and movement perception in lumbar spinal stenosis. Eur Spine J 22(4):788–793
Leinonen V, Airaksinen M, Taimela S et al (2007) Low back pain suppresses preparatory and triggered upper limb loading. Spine 32:E150–E155
Leinonen V, Kankaanpää M, Luukkonen M et al (2003) Lumbar paraspinal muscle function, perception of lumbar position and postural control in disc herniation-related back pain. Spine 28:842–848
Leinonen V, Kankaanpaa M, Luukkonen M et al (2001) Disc herniation-related back pain impairs feed-forward control of paraspinal muscles. Spine 26:E367–E372
Luoto S, Taimela S, Hurri H et al (1996) Psychomotor speed and postural control in chronic low-back pain patients: a controlled follow-up study. Spine 21:2621–2627
Moseley GL, Hodges PW, Gandevia SC (2003) External perturbation of the trunk in standing humans differentially activates components of the medial back muscles. J Physiol 547:581–587
Strutton PH, Catley M, McGregor AH, Davey NJ (2003) Corticospinal exicitability in patients with unilateral sciatica. Neurosci Lett 353:33–36
Taimela S, Kankaanpää M, Luoto S (1999) The effect of lumbar fatique on the ability to sense a change in lumbar position—a controlled study in chronic LBP patients and healthy controls. Spine 24:1322–1327
Chiou S, Shih Y, Chou L et al (2014) Impaired neural drive in patients with low back pain. Eur J Spine 18:794–802
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kääriäinen, T., Taimela, S., Aalto, T. et al. The effect of decompressive surgery on lumbar paraspinal and biceps brachii muscle function and movement perception in lumbar spinal stenosis: a 2-year follow-up. Eur Spine J 25, 789–794 (2016). https://doi.org/10.1007/s00586-015-4036-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-4036-5