
Abstract
Purpose
This study investigated side-to-side gait asymmetry in subjects with adolescent idiopathic scoliosis.
Methods
There were 20 adolescents with idiopathic scoliosis and 20 age-matched control subjects, who participated in the study. To minimize confounding effects, we recruited patients with similar spinal curvature for the scoliosis group, and all participants are right hand dominant. The participants were instructed to ambulate on a 10 m walkway while barefoot. There were two force plates in the middle of the walkway. The ground reaction force (GRF) and angular displacements of six segments (foot, shank, thigh, pelvis, trunk, and head) were measured during one gait cycle based on the right and left lower extremities. To remove the positional information in the kinematic data, the derivative of angular displacement in each segment was calculated. To evaluate the side-to-side gait symmetry, we calculated the cross-correlation of each bilateral gait parameter.
Results
In the kinematics, the scoliosis group demonstrated asymmetrical gait in the frontal and transverse planes compared to the control group. In the GRF data, the scoliosis group demonstrated asymmetrical gait in the medial–lateral (M/L) direction compared to the control group.
Conclusions
These results indicated that the scoliosis group produced an asymmetrical rotation pattern of the segments bilaterally in the frontal and transverse planes, resulting in asymmetrical GRF patterns in the M/L direction. This asymmetrical gait may be produced by changes in global postural control during gait and not simply by changes in control of only one or two specific segments.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adolescent idiopathic scoliosis (AIS) is a three-dimensional deformity of the spine and has been reported to be prevalent in 1–3 % of the population aged 10–16 years [1]. Several studies have shown that AIS alters the connective structure of the spine, leading to changes in mobility and balance [2–4]. Since the trunk assists in the maintenance of body balance [5], a presence of spinal deformity would alter the center of mass (COM) during gait, leading to the development of a pathological gait pattern.
It has been reported that gait patterns differed between patients with scoliosis and their healthy peers. Such differences include decreased step length [6–8] and reduced range of motion (ROM) in the upper and lower extremities (LE) [6], but one study showed no difference [9]. It has also been reported that the gait pattern is symmetrical in healthy populations [10–13], but marked differences have been found between affected and unaffected limbs in pathological gait [14, 15]. A limited number of studies have evaluated side-to-side asymmetry of gait in AIS. One study showed asymmetry of trunk rotation in the transverse plane. During gait, the trunk rotated asymmetrically to the line of progression, which showed a torsion offset with minimum torsion at right heel contact and maximum torsion at left heel contact, producing ground reaction force (GRF) asymmetry of free rotational moment around the vertical axis [16]. In GRF studies conducted to evaluate gait asymmetry in AIS, patients with scoliosis showed asymmetrical gait in the vertical [17], anterior–posterior (A/P) [18], and medial–lateral (M/L) [19] directions. These studies adopted the peak angle of the joint [16] or the peak force [11, 18] at a certain time to compute symmetry index. However, spatial–temporal information is an important factor to understand human gait control [20]. Thus, in our study, correlation coefficient (CC) was adopted to evaluate gait asymmetry.
The aim of the present study was to investigate the side-to-side gait asymmetry in subjects with AIS. It was hypothesized that the scoliosis group would show asymmetrical patterns in kinematics and GRF compared to the control group, especially in the M/L direction. To minimize confounding effects, subjects with a similar spinal curvature (right thoracic and left lumbar scoliosis with double curves, the left convex on the lumbar spine or the right convex on the thoracic spine, in posterior view) were recruited for the scoliosis group and compared with an age-matched control group. As mentioned above, the torsion offset has been found in AIS during gait. Thus, we calculated the derivative of angular displacement in each segment to remove positional information and used this value for calculating the side-to-side gait asymmetry.
Methods
Subjects
There were 20 adolescents with idiopathic scoliosis (gender: 2 male and 18 female, age: 14.9 ± 1.0 years, height: 161.6 ± 6.6 cm, weight: 59.2 ± 7.6 kg) in the scoliosis group and 20 age-matched healthy adolescents (gender: 5 male and 15 female, age: 14.4 ± 1.0 years, height: 160.9 ± 5.7 cm, weight: 53.3 ± 9.8 kg) in the control group, who participated in the study.
The subjects were recruited from a middle school closely located to the Motion Analysis Lab. Before the experiment, a medical examination by interview was performed to evaluate pain or discomfort of the spine, hip, knee and ankle joints. Also, a morphological examination was performed to evaluate shoulder imbalance, pelvis tilting, and hip and knee contractures. If a subject reported any history of disease, discomfort on the spine, hip, knee and/or ankle joints within the past 3 months, morphological problems (such as abnormal ROM), and/or neurological abnormalities, the subject was excluded from our study. After the medical and morphological examinations, the screening test on scoliosis was performed using Adam’s forward bending test. If the subject showed a positive sign for the test, then whole spine radiography was examined to confirm the diagnosis. The subjects in the scoliosis group were selected from those who were diagnosed as having idiopathic scoliosis in the past month, and who did not receive any treatment or undergo surgery prior to and during the study.
The Cobb’s angle of each subject in the scoliosis group is presented in Table 1. To prevent the confounding effect of the spinal curve on the gait asymmetry, we recruited subjects with scoliosis who showed a similar type of spinal deformity. Also, we recruited all subjects who were right limb dominant to prevent a confounding effect of handedness on gait asymmetry. Thus, all subjects in both groups were right handed based on the functional characteristics of handedness as determined by the Edinburgh handedness questionnaire [21]. Each subject received information regarding the purpose and methods of the study and signed a copy of the consent form approved by the Institutional Review Board of Korea University.
Procedure
Prior to the main experiment, each subject’s height and weight were measured. Each subject presented at the Motion Analysis Lab for a familiarization session which comprised of at least five trials of walking naturally along a 10 m walkway at a comfortable speed while barefoot. There were two force plates (Bertec FP4060) in the middle of the walkway.
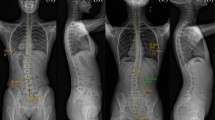
The subjects were not given information about the location of the force plates to maintain natural gait. A trial was excluded from the data collection, if the vertical and A/P GRF patterns did not match with a normal gait pattern. If the subjects stepped on the edge of the force plate, they were instructed to change the start position. The subjects performed several trials until five trials of the gait data showing a normal GRF pattern were successfully collected. The GRF of the two LE was collected in each trial (Fig. 1).

Illustration of one gait cycle for the right leg (a–c) and for the left leg (b–d). The angular displacements of the segments were calculated based on these gait cycles. The experimenter controlled the start position so that each subject always touched the first force platform with his/her right heel and the second force platform with his/her left heel
The GRF was collected in three axes (x axis: the M/L force, y axis: the A/P force, z axis: the vertical force) with the sampling rate at 1,200 Hz. To capture kinematic data, reflective markers were attached to the subject’s body following the Helen Hayes model that we adopted in a previous study [22]. Six digital cameras captured the motion of each marker three-dimensionally (Motion Analysis Corporation, Santa Rosa, CA, USA) with the sampling rate at 60 Hz.
Data analysis
To calculate gait parameters in kinematics, the three-dimensional movement data of the markers were filtered with low-pass at 6 Hz using a fourth-order, zero lag, Butterworth filter. All parameters were normalized to a percentage (%) of the gait cycle. The angular displacements of each segment (foot, shank, thigh, pelvis, trunk, and head) were calculated (Fig. 2), and the derivative of the angular displacement of the segments were then calculated to remove position information. To evaluate the side-to-side gait asymmetry, the CC was calculated using the derivative of the angular displacement of the two sides in each group. We also measured gait speed, cadence, stride length, step length, and stance and swing times (Table 2).

Definition of angular displacement of the segments in the sagittal plane. θ ft = angular displacement of the foot (foot rotation relative to the ankle), θ sh = angular displacement of the shank (shank rotation relative to the knee), θ th = angular displacement of the thigh (thigh rotation relative to the hip), θ pe = angular displacement of the pelvis (pelvic rotation relative to the global coordinate at the hip), θ tr = angular displacement of the trunk (trunk rotation relative to the sacrum), and θ hd = angular displacement of the head (head rotation relative to the first thoracic spine level)
The GRF data of the right and left LE in each axis were selected and filtered with low-pass at 15 Hz using a fourth-order, zero lag, Butterworth filter. The data were then normalized to the body weight of each subject. Also, the time was normalized to % of the stance time.
To assess the side-to-side gait asymmetry, the CC between pairs of data was calculated with the following formula: \( {\text{CC}} = \Upsigma {\text{R}}_{i} {\text{L}}_{i} /\left( {(\Upsigma {\text{R}}_{i}^{ 2} )^{ 1/ 2} (\Upsigma {\text{L}}_{i}^{ 2} )^{ 1/ 2} } \right) \), where R i and L i are the ith values of the left and right LE data, and i = 1,2, …, 100 in this study. The two profiles are exactly the same shape when the CC is 1 [23].
Statistics
Statistical analyses were performed using SPSS 16 (SPSS, Chicago, IL). Normality was assessed for each dependent variable by using Kolmogorov–Smirnov test. For comparing the CC of the kinematics between the two groups, a mixed repeated ANOVA was performed in each plane with the factors of Segment (6 levels: foot, shank, thigh, pelvis, trunk, and head) and Group (2 levels: scoliosis and control groups). A t test was also used to compare the gait parameters and CC of the GRF between the two groups or between the right and left LE in each group. The significance level was set at P < 0.05.
Results
During gait, the control and scoliosis groups demonstrated similar walking speeds (control: 112.0 ± 2.2 cm/s, scoliosis: 115.0 ± 2.6 cm/s), stride lengths (control: 119 ± 1.9 cm, scoliosis: 124 ± 2.4 cm), and cadences (control: 111.4 ± 1.3 steps/min, scoliosis: 109.4 ± 1.7 steps/min) (Table 2a). However, each group demonstrated different gait parameters in the comparison of bilateral LE. Similar step lengths for bilateral LE were found in the control group, while different step lengths were found in the scoliosis group (Table 2b). Also, in the relative time of the stance and swing phases (i.e., % of a gait cycle), the control group showed a similar duration between the two LE in each phase while the scoliosis group showed a longer stance (or a shorter swing) time during the right LE than during the left LE (Table 2b).
CC of the kinematic parameters
The CC of the kinematic parameters is presented in Table 2c. In the coronal plane, the scoliosis group demonstrated less CC than the control group (P = 0.019). Also, the thigh and pelvis showed a greater CC, and the foot and shank showed a smaller CC compared to the other segments. These results were confirmed by a mixed repeated ANOVA showing main effects of Group and Segment, but no interaction.
In the sagittal plane, the two groups showed a similar CC (P = 0.122). The thigh and shank showed a greater CC, and the pelvis and head showed a smaller CC compared to the other segments. These results were confirmed by a mixed repeated ANOVA showing a main effect of Segment.
In the transverse plane, the scoliosis group demonstrated a smaller CC than the control group (P = 0.010); the pelvis and trunk showed a greater CC, and the foot, shank, and thigh showed a smaller CC compared to the other segments (P < 0.001). These results were confirmed by a mixed repeated ANOVA showing main effects of Group and Segment, but no interaction.
CC of ground reaction force
The scoliosis group showed a smaller CC than the scoliosis group in the M/L direction, but the two groups showed similar CC in the other directions (Table 3).
Discussion
The aim of this study was to investigate the side-to-side gait asymmetry present in subjects with AIS. To evaluate gait asymmetry, we three-dimensionally computed the CC of the rotation pattern of each segment and the CC of GRF pattern and then compared the CC between the scoliosis and control groups.
Our study demonstrated that the scoliosis group showed an asymmetrical rotation of segments in the frontal and transverse planes compared to the control group. Mahaudens and co-workers [6] found an absence of side-to-side asymmetry for all kinematic parameters in AIS, although scoliotic patients reduced their ROM of the pelvis, hip, and shoulder in the frontal plane and ROM of the knee in the sagittal plane. Also, Kramers-de Quavain and co-workers [16] reported that scoliotic patients showed no side-to-side asymmetry, except for an asymmetrical torsion offset to the line of progression. Consistently, our results showed no difference in CC between the two groups in each segment (i.e., we did not observe the interaction of Group by Segment in the ANOVA). However, we observed that the scoliosis group showed a smaller CC than the control group in the frontal and transverse planes.
We observed that the asymmetry was due to a combination of all segments, but not due to one or two specific segments. This may indicate a global phenomenon characterized by bilateral disturbances. Spinal deformity in AIS produces translational and angular asymmetry of the vertebrae of the rib cage and back surface, thereby resulting in an asymmetrical load on the spine [24]. This could alter segmental position and lead to alteration of the body COM position during gait. Meanwhile, in our study, the scoliosis and control groups showed a higher symmetry of the rotational pattern in the pelvis and thigh in the frontal plane, in the shank and thigh in the sagittal plane, and in the pelvis and trunk in the transverse plane (Table 2). This meant that the scoliosis group utilized the same control strategy of each segment as the control group. Thus, the asymmetrical gait shown in AIS may be due to changes in global postural control strategies, and these changes may be due to changes in the sensory [8] and/or somatosensory systems [25–27].
Our study measured some time–distance gait parameters, such as gait speed, cadence, and stride length, and showed that the scoliosis group did not show any differences in these gait parameters compared to the control group. These findings are consistent with those of Chen and co-workers [9]. In contrast, reduction of step length [6, 7] and decreased cadence [19] were found in other studies. These contradictory results might be due to the difference in severity of spinal deformity of the subjects among the studies [28]. For example, most scoliotic patients showed mild deformity (i.e., below 30° in Cobb’s angle) in our study, while the patients in the study of Mahaudens and co-workers [6] showed mild to severe deformity (i.e., one patient group showed Cobb’s angle above 40°). Although the scoliosis and control groups in our study showed similar mean values in the gait parameters, the scoliosis group showed an asymmetrical gait pattern for step length and duration of gait phase, i.e., longer step length and longer stance phase (shorter swing phase) in the right LE.
Some studies showed a positive correlation between spinal deformity and angular displacement in the pelvis during gait in subjects with AIS [19, 28, 29]. These studies generally adopted angular displacement of segments in the comparison of scoliotic patients and healthy controls. However, previous studies dealing with gait asymmetry adopted segmental maximum and minimum peaks in each side [11, 16, 18]. Our study adopted a different calculation method from the one used in these previous studies since temporal information is also important in understanding human motor control in addition to force or angle in a certain time [20]. Thus, CC was adopted to calculate the side-to-side gait asymmetry. Also, our study adopted the derivative of segmental angles instead of the angular displacement of segments because we were interested in the rotation pattern of segments regardless of the difference in bilateral segment position in AIS. These methodological differences might result in asymmetrical gait in the global aspects as shown in our results.
From the kinematic results in our study, we expected that the kinematic asymmetry in the frontal and transverse planes could lead to an asymmetrical GRF, especially in the M/L direction. As expected and consistent with the findings of Giakas and co-workers and Kramers-de Quavain and co-workers, the GRF results showed that the scoliosis group demonstrated an asymmetrical gait compared to the control group in the M/L direction, although the data analysis was different among our study and the other two studies. Besides this, the gait asymmetry in AIS can be expected from the findings of standing balance control studies, which reported that subjects with AIS showed less balance control than healthy controls during upright standing posture, especially in the M/L direction [9, 30]. The directional differences shown in these studies may be due to methodological differences and/or differences in severity of spinal deformity of the scoliotic patients, but further studies are needed.
In conclusion, our study clearly demonstrated that the scoliosis group showed asymmetrical gait in kinematics and GRF. In the kinematics, gait asymmetry was found in the frontal and transverse planes during combined rotation of all segments. In GRF, gait asymmetry was found in the M/L direction. This asymmetrical gait demonstrated by subjects with AIS may be due to changes in global postural control strategies caused by spinal deformity.
References
Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA (2008) Adolescent idiopathic scoliosis. Lancet 371:1527–1537
Danielsson AJ, Romberg K, Nachemson AL (2006) Spinal range of motion, muscle endurance, and back pain and function at least 20 years after fusion or brace treatment for adolescent idiopathic scoliosis: a case-control study. Spine (Phila Pa 1976) 31:275–283
Lenke LG, Engsberg JR, Ross SA, Reitenbach A, Blanke K, Bridwell KH (2001) Prospective dynamic functional evaluation of gait and spinal balance following spinal fusion in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 26:E330–E337
Schwender JD, Denis F (2000) Coronal plane imbalance in adolescent idiopathic scoliosis with left lumbar curves exceeding 40 degrees: the role of the lumbosacral hemicurve. Spine (Phila Pa 1976) 25:2358–2363
Thorstensson A, Nilsson J, Carlson H, Zomlefer MR (1984) Trunk movements in human locomotion. Acta Physiol Scand 121:9–22
Mahaudens P, Banse X, Mousny M, Detrembleur C (2009) Gait in adolescent idiopathic scoliosis: kinematics and electromyographic analysis. Eur Spine J 18:512–521
Mahaudens P, Thonnard JL, Detrembleur C (2005) Influence of structural pelvic disorders during standing and walking in adolescents with idiopathic scoliosis. Spine J 5:427–433
Mallau S, Bollini G, Jouve JL, Assaiante C (2007) Locomotor skills and balance strategies in adolescents idiopathic scoliosis. Spine (Phila Pa 1976) 32:E14–E22
Chen PQ, Wang JL, Tsuang YH, Liao TL, Huang PI, Hang YS (1998) The postural stability control and gait pattern of idiopathic scoliosis adolescents. Clin Biomech (Bristol, Avon) 13:S52–S58
Giakas G, Baltzopoulos V (1997) Time and frequency domain analysis of ground reaction forces during walking: an investigation of variability and symmetry. Gait Posture 5:189–197
Herzog W, Nigg BM, Read LJ, Olsson E (1989) Asymmetries in ground reaction force patterns in normal human gait. Med Sci Sports Exerc 21:110–114
Hannah RE, Morrison JB, Chapman AE (1984) Kinematic symmetry of the lower limbs. Arch Phys Med Rehabil 65:155–158
Chou LS, Song SM, Draganich LF (1995) Predicting the kinematics and kinetics of gait based on the optimum trajectory of the swing limb. J Biomech 28:377–385
Hesse S, Reiter F, Jahnke M, Dawson M, Sarkodie-Gyan T, Mauritz KH (1997) Asymmetry of gait initiation in hemiparetic stroke subjects. Arch Phys Med Rehabil 78:719–724
Wall JC, Turnbull GI (1986) Gait asymmetries in residual hemiplegia. Arch Phys Med Rehabil 67:550–553
Kramers-de Quervain IA, Muller R, Stacoff A, Grob D, Stussi E (2004) Gait analysis in patients with idiopathic scoliosis. Eur Spine J 13:449–456
Schizas CG, Kramers-de Quervain IA, Stussi E, Grob D (1998) Gait asymmetries in patients with idiopathic scoliosis using vertical forces measurement only. Eur Spine J 7:95–98
Chockalingam N, Dangerfield PH, Rahmatalla A, el Ahmed N, Cochrane T (2004) Assessment of ground reaction force during scoliotic gait. Eur Spine J 13:750–754
Giakas G, Baltzopoulos V, Dangerfield PH, Dorgan JC, Dalmira S (1996) Comparison of gait patterns between healthy and scoliotic patients using time and frequency domain analysis of ground reaction forces. Spine (Phila Pa 1976) 21:2235–2242
Grasso R, Bianchi L, Lacquaniti F (1998) Motor patterns for human gait: backward versus forward locomotion. J Neurophysiol 80:1868–1885
Oldfield RC (1971) The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 9:97–113
Sung PS, Yoon B, Lee DC (2010) Lumbar spine stability for subjects with and without low back pain during one-leg standing test. Spine (Phila Pa 1976) 35:E753–E760
Wren TA, Do KP, Rethlefsen SA, Healy B (2006) Cross-correlation as a method for comparing dynamic electromyography signals during gait. J Biomech 39:2714–2718
Stokes IA (1997) Analysis of symmetry of vertebral body loading consequent to lateral spinal curvature. Spine (Phila Pa 1976) 22:2495–2503
Guo X, Chau WW, Hui-Chan CW, Cheung CS, Tsang WW, Cheng JC (2006) Balance control in adolescents with idiopathic scoliosis and disturbed somatosensory function. Spine (Phila Pa 1976) 31:E437–E440
Simoneau M, Mercier P, Blouin J, Allard P, Teasdale N (2006) Altered sensory-weighting mechanisms is observed in adolescents with idiopathic scoliosis. BMC Neurosci 7:68
Lao ML, Chow DH, Guo X, Cheng JC, Holmes AD (2008) Impaired dynamic balance control in adolescents with idiopathic scoliosis and abnormal somatosensory evoked potentials. J Pediatr Orthop 28:846–849
Syczewska M, Graff K, Kalinowska M, Szczerbik E, Domaniecki J (2012) Influence of the structural deformity of the spine on the gait pathology in scoliotic patients. Gait Posture 35:209–213
Legaye J, Duval-Beaupere G, Hecquet J, Marty C (1998) Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J 7:99–103
Zabjek KF, Leroux MA, Coillard C, Rivard CH, Prince F (2005) Evaluation of segmental postural characteristics during quiet standing in control and idiopathic scoliosis patients. Clin Biomech (Bristol, Avon) 20:483–490
Acknowledgments
This work was supported by the Institute of Health Science Grant at Korea University and the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology (2010-0003015). Part of this study was also supported by the Korea Healthcare Technology R&D project (A110416).
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yang, J.H., Suh, SW., Sung, P.S. et al. Asymmetrical gait in adolescents with idiopathic scoliosis. Eur Spine J 22, 2407–2413 (2013). https://doi.org/10.1007/s00586-013-2845-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-013-2845-y