
Abstract
Coccygodynia is a pathological condition associated with pain–discomfort all around the bottom end of the spine. The aetiology and the intensity of the symptoms may defer significantly. The effectiveness of the surgical treatment remains obscure. Our purpose, through this systematic review is to evaluate the results of surgical treatment of coccygectomy. Literature retrieval was performed by the use of the PubMed searching engine utilising the terms ‘coccygodynia–coccygectomy’ in the English language from January 1980 to January 2010. Case reports and tumour related case series were excluded as well as articles published in other languages. In total 24 manuscripts were analyzed. Only 2 of them were prospective studies whereas 22 were retrospective case series; five were classified as Level III studies and the remaining as Level IV studies. In total, 671 patients with coccygodynia underwent coccygectomy following failed conservative management. The sex ratio, male/female was 1:4.4. The most popular aetiology for coccygodynia was direct trauma in 270 patients. 504 of the patients reported an excellent/good outcome following the procedure. There were 9 deep and 47 superficial infections. Other complications included two haematomas, six delayed wound healings and nine wound dehiscence. The overall complication rate was 11%. Patients with history of spinal or rectal disorders, as well as idiopathic or with compensation issues, had less predictable outcome than those with history of trauma or childbirth. Coccygectomy can provide pain relief to as high as 85% of the cases. The most common reported complication was wound infection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Coccygodynia was initially described by Simpson [1] as pain–discomfort localised around the bottom end of the spine and usually triggered by prolonged sitting. The aetiology and the intensity of the symptoms may defer significantly. It could be the result of severe trauma, repetitive injury, post childbirth, local tumours, disk degeneration and of idiopathic nature [2–6, 34]. The exact pathophysiologic mechanisms associated with coccygodynia are still obscure, while obesity is considered as a predisposing factor due to the resulting pelvic rotation [2].
Coccygodynia has been shown to be more common in the female population. This has been attributed to specific sex-related anatomic features (slender females have little subcutaneous fat and the coccyx is relatively unpadded; greater sciatic notch being wider, contributes to backward inclination of the sacrum and coccyx, thus increasing the possibility of injury to the area of the coccyx; females have greater inter-ischial tuberosity distance which increases the pressure to the coccyx) [3, 4]. Furthermore, it has been reported that psychological depression, neurosis or hysteria, magnifies the clinical symptoms [5, 6].
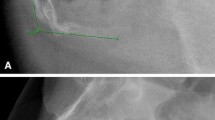
Both clinical signs (pain and abnormal movement on palpation) and radiological features can aid in making the diagnosis. Radiological evaluation is usually performed with lateral sacral radiographs, allowing classification of the shape of the coccyx according to its inclination [7] (Table 1). The use of dynamic X-rays, comparing standing and sitting radiographs has also been found useful [2, 8, 9] (Table 1). MRI and bone scintigraphy can provide valuable information excluding the presence of degenerative spine disease, local tumour pathology or metastatic bone disease.
Treatment options of coccygodynia can be non-operative or operative. Non-operative treatment includes rest, NSAID’s drugs, doughnut-shape cushion usage, physiotherapy, radiotherapy, sacral rhizotomy, epidural injections and local injections with or without coccyx manipulation. In cases of persistent symptoms unresponsive to conservative treatment, coccygectomy is offered as the definitive surgical solution. Two different types of surgical resection have been described (Table 2), with the most popular one being the procedure introduced by Key [10], which differs from that of Gardner [11], as to the direction of the coccyx dissection from the rectum. According to Postacchini and Massobrio [7], the coccyx can be removed either totally or partially with comparable good results. A sub-periosteal resection instead of a total coccygectomy has also been reported as an option [12]. However, the literature regarding the results of surgical treatment is vague. The purpose of this study therefore was to evaluate the results and complications, as well as the patient’s satisfaction following surgical treatment of coccygodynia (coccygectomy).
Materials and methods
Literature retrieval was performed by the use of PubMed searching machine and by using the terms “coccygodynia”, and/or “coccygectomy” as key words. The searching limits included English literature and time period between 1980 and January 2010. Sixty-eight articles were initially identified. Case reports, editorials and tumour-related case series were excluded, as well as case series referring solely to other methods of management and not surgical resection. Series comparing surgical versus injection therapy were included. Further research was made through the articles references. All extracted articles did not meet the selection criteria, as they were published prior to 1980.
Manuscripts selected were analyzed according to the data providing for the number of patients, including age, gender characteristics, the period of pre-exciting symptoms, the aetiology and classification, the type of surgery, the use of antibiotics or drain, the follow-up period and the frequency of perioperative complications.
Statistical analysis of the data was performed using the Statistical Package for the Social Sciences (SPSS), version 16.0 (SPSS, Inc., Chicago, IL, USA).
Continuous variables were expressed as the mean ± standard deviation, and categorical variables were expressed as frequencies and percentages. The Chi-square test was used to evaluate any potential association of the two different surgical procedures with the postoperative outcome and complication rate. Odds ratios (OR) and 95% confidence intervals (CI), were calculated by means of simple logistic regression analysis, as the measure of the above associations. All tests were two tailed and statistical significance was considered for p values <0.05.
Results
In total 24 manuscripts met the inclusion criteria and were analyzed (Tables 3, 4, 5) [13–32]. Only two of them [4, 18] were prospective series, and five were classified as Level III studies [4, 12, 18, 23, 26]. The majority were retrospective uncontrolled case series. In total, the reviewed series included 671 patients with coccygodynia that had coccygectomy as definitive pain management. The range of the mean ages of those series was from 26.4 [12] to 52.8 years [25]. The extremes of the age range were 11 [4, 7, 26] and 76 [4] years.
Gender characteristics were provided on 617 patients [4, 5, 7, 12–32]. The vast majority of the patients were females (511 pts, 82.9%), while males were only 106 in number (17.1%), bringing the male/female ratio to 1/4.4. In three studies, the demographics were presented only on the initial recruited population [4, 22, 23].
The aetiology of the coccygodynia was reported in 457 patients [4, 5, 7, 12, 14–17, 19, 20, 22–29, 31, 32]. The most common cause of coccygodynia was direct trauma, recorded in 270 patients, (59.1%). Not-identifiable causes (idiopathic coccygodynia) were present in 141 cases (30.9%), childbirth in 37 females (8.1%), recent rectal or lumbar spinal surgery or epidural injection in 9 (1.9%).
The classification introduced by Postacchini and Massobrio [7] was used in six papers [7, 16, 23–25, 29]. In total, 153 X-rays were analyzed and according to them, there were 57 type I (37.3%), 48 type II (31.4%), 29 type III (18.9%) and 19 type IV (12.4%) [3, 16, 18, 19, 23]. Grosso and van Dam [16] reported that 4/5 of their patient population was in groups II, III, IV. Some other studies used the subluxation and hypermobile characteristics of the coccyx, presenting some prevalence of the subluxation type over the hypermobile, which was not statistically significant [18, 21, 28].
There were four (1 prospective) comparative studies assessing the efficiency of injections to surgical treatment (coccygectomy) [4, 20, 22, 23]. Their findings showed that injection with manipulation is effective in providing pain relief, but they also suggested that coccygectomy is a valid surgical option for those in whom the conservative management failed.
Prior to coccygectomy, the majority of patients had undergone non-operative treatment modalities for a variable period of time ranging from 3–6 months [3, 15, 22] to 14–15 years [7, 16].
In the majority of the papers the operation performed was well described. Most of the surgeons prefer a surgical exposure similar to the operation introduced by Key [10].
Preoperatively, the surgeons suggested pharmaceutical constipation and/or a low residual diet mainly to prevent any possible contamination of the wound during the operation. For the same reason, a fleet enema was used the day before surgery and intravenous administration of second generation cephalosporin was advisable. The patients had general anaesthesia and were positioned prone with the buttocks separated and secured laterally for facilitating the exposure. A longitudinal incision was performed from the sacrum to the tip of the coccyx (either with knife or electrocautery). Depending on the authors either partial or total coccygectomy was performed. It was advisable to preserve the ligamentous and muscular attachments together with the periosteum. After meticulous haemostasis the buttocks were released and the incision was closed in layers. For the skin either absorbable [12, 20, 32] or non-absorbable sutures [22, 30] were used.
Perioperative use of antibiotics was recorded in all except one study [5]. In six papers [3, 12, 21–23, 29] a second generation cephalosporin was administered for 48 h post-operatively, while the rest of the studies vary significantly as to the type and duration of their chemoprophylaxis.
Maigne et al. [18], Doursounian et al. [21] and Pennekamp et al. [26] have stated clearly the necessity of a drain for avoiding the void space which could compromise the results. On the other hand, several authors [15–17, 23, 27, 28] advocated against the necessity of a drain. It is obvious that one could consider that the usage of drain in close proximity to rectus may be considered as a cause for increased infection rate, but this systematic review could not confirm any direct relation between the usage of drain and rate of infections.
Following surgery laxative or enema together with a low residual diet were often used to facilitate patients post operative management.
Patient follow-up (Table 4) ranged from 4 months [24] to 16 years [15, 26, 27] post surgery, with the vast majority of the studies having a mean follow-up period of more than 2 years. Thus, the recorded results of these coccygectomy series are extending to a mid-term period post surgery.
The complication rates in the reviewed series varied from 0 [30] to 50% [31]. All but three studies were referring to postoperative complications [4, 13, 25]. There were 56 (8.34%) reported wound infections (9 deep and 47 superficial) all treated with antibiotics and one with surgical debridement [5, 7, 12, 14–24, 26–30, 32]. Escherichia coli [12, 26] and Staphylococcus aureus [21] were the most frequently recorded bacteria in those series with reported microbiology results. Moreover, there were 2 (0.3%) haematomas, 9 (1.3%) wounds dehiscence that lead to further surgical management and 6 (0.9%) delayed healings. The overall complication rate was 10.9%.
It was notable that small series [20, 22, 23, 31] had the highest complication rates ranging from 26.7 to 50%. Bayne et al. [5] reported also a large number of complications (10 equal to 20.6%) that was attributed to no antibiotic prescription in contrast to the rest of the authors and protocols.
The clinical outcome of the reviewed series of coccygectomy could be classified into excellent or good (cases of mild occasional discomfort), fair (cases with decreased residual pain) and poor results (cases of persistent or worsening symptoms) (Table 5). This systematic analysis revealed that 504 over 596 patients treated with coccygectomy had excellent or good outcome (84.6%), 46 patients fair (7.7%) and 46 poor outcome (7.7%) [4, 5, 7, 12–32].
Some of the authors [12, 19, 21, 22, 26, 28, 31, 32] used VAS visual analogue scale and the Oswestry disability index [33] for evaluating their results. Perkins et al. [19] and Hodges et al. [22] presented a decrease of VAS from 8.3 to 4.5 and 7.3 to 3.6, respectively. Similarly the reduction of ODI was from 35.6 to 12.5 and 55–36, respectively. Cebesoy et al. [31] also commented that there was a progression of VAS reduction through time from 51.8 pre-operatively to 3.18 at 6 months and 2.94 and 2.76 at 12 and 24 months, respectively.
Perkins et al. [19] recorded just 54% of cases with a good outcome (7/13) which was attributed to a selection bias of that series that included mostly patients with associated lumbar spinal disorders (10/13). Bayne et al. [5] reported 40% fair to poor outcome (19/48) and advocated against the Gardner surgical technique and the non-use of antibiotics.
Key’s surgical exposure was used (stated clearly) in seven studies [12, 19–21, 23, 29, 30] whereas in only one study the Garden’s exposure was used [5]. Statistical analysis of the incidence of complications between the two different techniques revealed a trend toward a higher complication rate in patients treated with the Gardner method (10 of 48 patients; 20.8%) compared with Key’s operation (30 of 232 patients; 12.9%) (χ 2 = 2.028, df = 1, p = 0.154; 95% CI of the difference, −2.4 to 21.8%), but this difference did not reach significance. Overall the risk of complications was increased, by almost 80%, among patients who underwent Gardner’s surgical exposure compared with patients managed with Key’s technique (OR, 1.77; 95% CI, 0.80–3.93).
Patients who underwent Key’s operation were more likely to have experienced better results compared with those who were managed with the Gardner method; the results of Key’s operation were excellent in 203 (87.5%) patients, fair in 11 (4.7%) patients and poor in only 18 (7.8%) patients, while 29 (60.4%), 11 (22.9%) and 8 (16.7%) of the patients who were managed with the Gardner method had excellent, fair and poor results, respectively (χ 2 = 23.641, df = 2, p < 0.001). Patients who underwent Key’s operation were almost five times more likely to experience an excellent result than those who were managed with the Gardner method (OR, 4.59; 95% CI, 2.28–9.21).
Discussion
Coccygodynia is a rare symptom; usually related to repetitive trauma, post childbirth or idiopathic nature and in some occasions could be a referred pain from lumbar spine degeneration [2–6, 34]. The pathophysiologic pathway associated with this condition is yet to be established.
Conservative treatment is usually effective and several studies [4, 20, 22, 23] have shown that local injection of steroids accompanied by coccyx manipulation provides good outcome to as high as 85% of the cases. When non-operative treatment modalities fail, coccygectomy appears to be a valid surgical alternative and represents a treatment option for a minority of the patients as according to Wray, only 23 (19.2%) of the 120 cases with coccygodynia finally underwent operative treatment [4].
In this study, we have attempted to analyse the existing evidence on the safety, efficacy and outcomes of coccygectomy in the non-oncology clinical setting.
The identified series lacked of strength as to their level of evidence. The majority but two [4, 18] were retrospective uncontrolled series [5, 7, 12–17, 19–32]. Five manuscripts were classified as type III evidence based series [4, 12, 18, 23, 26]. Thus, our presented analysis and conclusions inherit these weaknesses, as well as the absence of a comprehensive statistical meta-analysis of the results due to the wide discrepancies on the used methodologies. A certain selection bias can be also attributed to this study as it has excluded series published in other than English languages; it has utilised only the PubMed as a search vehicle and has retrieved manuscripts published during the past 30 years. Furthermore, the coccygectomy outcomes were based on subjective evaluation systems such as the VAS and the ODI [33] with no reported objective findings that could confirm—validate the effectiveness of the operation. Moreover, it was not possible to identify an evaluation system for documenting the relation between post operative findings and clinical outcome.
Despite the above limitations, from the data provided, several useful conclusions regarding coccygectomy can be extracted.
First, the vast majority of the authors [7, 12, 14, 18–21, 23, 24, 26, 28–30, 32] preferred to perform surgical dissection similarly to Key [10], and only Bayne et al. [5] used the Gardner exposure [11]. Statistical analysis revealed that patients who underwent coccygectomy according to Key had five times more chances to have a better outcome (p < 0.001), but that value was not significant.
Second, several authors [15, 20, 24, 28] reported the advantages of performing total coccygectomy compared with partial one, which appears to be associated with an increased incidence of recurrent pain and revision surgery [15]. It is of note though that some authors reported that sup-periosteal resection gives better results and reduce the risk of infection compared with total coccygectomy [12, 26].
Third, it appears that there is a sex domination as coccygodynia usually affects females in the prime of their lives from late 1920s to early 1950s. The reason for this has been attributed to the peculiarities of the female sacral anatomy [3, 4]. With regard to the causation, the most common aetiological factor that was noted in this review was trauma (local injury) in up to 60% of the cases. Kim and Suk [36] reported radiological findings indicating that the intercoccygeal angle had statistically significant difference between traumatic (with a mean angle of 47.9°) and idiopathic group (72.2°). It is worth also mentioning that disorders of the lumbar spine could be a predisposing factor [5, 7, 19, 27]. Finally, while it is a common belief that depression, neurosis or hysteria could magnify coccygodynia’s clinical symptoms [5, 6], none of the articles analysed included any details regarding the psychological state of the patients.
Fourth, the authors believe that before surgical intervention is contemplated, coccygodynia should be investigated thoroughly. Any lower spine or rectal pathology must be recorded and examined appropriately. Neurological examination would assist to exclude any deficit secondary to neural compression. Radiological investigations in the form of CT or MRI would assist in the diagnosis of protruding lower lumbar discs, spinal infection, spinal degeneration and tumours [37]. Similarly, colorectal doctors could exclude the presence of rectal pathologies (rectal tumours or teratomas, proctalgia fugax, levator ani syndrome, Alcock’s canal syndrome and descending perineum syndrome) [38–40] by performing rectal examination accompanied by sigmoidoscopy.
Fifth, as high as 85% of the patients expressed with a positive aspect, the effectiveness of the procedure and their satisfaction with regard to the outcome. While some authors reported that post trauma or childbirth patients had better outcome followed by those with unidentified aetiology [5, 26], Wray and Templeton [13] found an increased failure rate in male patients with trauma or idiopathic aetiology and those who did not successfully complete a trial of conservative management.
Last, the overall complication rate was 10.9% but none of those complications reported was life threatening. The majority were infections that resolved with antibiotic treatment or surgical debridement. Although such complications have been previously reported as rectum prolapsus and rectal injuries following coccygectomy [35], we were not able to confirm them in this systematic review. We were also unable to identify a direct relationship between infection and poor outcome. In addition, it is noteworthy that patients involved in litigation/compensation cases usually exhibited a poor outcome [20].
Conclusion
Summarizing the data presented, coccygectomy appears to be a valid surgical alternative for those patients who failed to respond to conservative management. It seems that the most popular surgical technique introduced by Key [10] with total sub-periosteal coccygeal resection, has a trend of better results and fewer complications. Surgeons must be aware that patients with history of spinal or rectal disorders, or with compensation issues, had less predictable outcome compared with those with a history of trauma or childbirth problems. The patient must be informed that following coccygectomy, wound infection can occur due to the bacterial colonization which may delay wound healing. However, this complication is not usually associated with a poor outcome.
References
Simpson JY (1859) Coccygodynia and diseases and deformities of the coccyx. Med Times Gaz 40:1–7
Maigne JY, Doursounian L, Chatellier G (2000) Causes and mechanisms of common coccygodynia: role of body mass index and coccygeal trauma. Spine (Phila Pa 1976) 25(23):3072–3079
Duncan GA (1937) A painful coccyx. Arc Surg 34:1088–1104
Wray CC, Easom S, Hoskinson J (1991) Coccydynia. Aetiology and treatment. J Bone Joint Surg Br 73(2):335–338
Bayne O, Bateman JE, Cameron HU (1984) The influence of etiology on the results of coccygectomy. Clin Orthop Relat Res 190:266–272
Pyper JB (1957) Excision of the coccyx for coccygodynia; a study of the results in twenty-eight cases. J Bone Joint Surg Br 39-B(4):733–737
Postacchini F, Massobrio M (1983) Idiopathic coccygodynia. J Bone Joint Surg Am 65:123–126
Maigne JY, Tamalet B (1996) Standardized radiologic protocol for the study of common coccygodynia and characteristics of the lesions observed in the sitting position. Clinical elements differentiating luxation, hypermobility, and normal mobility. Spine (Phila Pa 1976) 21(22):2588–2593
Maigne JY, Guedj S, Straus C (1994) Idiopathic coccygodynia. Lateral roentgenograms in the sitting position and coccygeal discography. Spine (Phila Pa 1976) 19(8):930–934
Key JA (1937) Operative treatment of coccygodynia. J Bone Joint Surg Am 19:759–764
Gardner RC (1972) An improved technique of coccygectomy. Clin Orthop 85:143–145
Bilgic S, Kurklu M, Yurttaş Y et al (2009) Coccygectomy with or without periosteal resection. Int Orthop 34(4):537–541
Wray AR, Templeton J (1982) Coccygectomy. A review of thirty-seven cases. Ulster Med J 51(2):121–124
Eng JB, Rymaszewski L, Jepson K (1988) Coccygectomy. J R Coll Surg Edinb 33(4):202–203
Hellberg S, Strange-Vognsen HH (1990) Coccygodynia treated by resection of the coccyx. Acta Orthop Scand 61(5):463–465
Grosso NP, van Dam BE (1995) Total coccygectomy for the relief of coccygodynia: a retrospective review. J Spinal Disord 8(4):328–330
Zayer M (1996) Coccygodynia. Ulster Med J 65(1):58–60
Maigne JY, Lagauche D, Doursounian L (2000) Instability of the coccyx in coccygodynia. J Bone Joint Surg Br 82(7):1038–1041
Perkins R, Schofferman J, Reynolds J (2003) Coccygectomy for severe refractory sacrococcygeal joint pain. J Spinal Disord Tech 16(1):100–103
Ramsey ML, Toohey JS, Neidre A et al (2003) Coccygodynia: treatment. Orthopedics 26(4):403–405
Doursounian L, Maigne JY, Faure F et al (2004) Coccygectomy for instability of the coccyx. Int Orthop 28(3):176–179
Hodges SD, Eck JC, Humphreys SC (2004) A treatment and outcomes analysis of patients with coccydynia. Spine J 4(2):138–140
Wood KB, Mehbod AA (2004) Operative treatment for coccygodynia. J Spinal Disord Tech 17(6):511–515
Karalezli K, Iltar S, Irgit K et al (2004) Coccygectomy in the treatment of coccygodynia. Acta Orthop Belg 70(6):583–585
Feldbrin Z, Singer M, Keynan O et al (2005) Coccygectomy for intractable coccygodynia. Isr Med Assoc J 7(3):160–162
Pennekamp PH, Kraft CN, Stütz A et al (2005) Coccygectomy for coccygodynia: does pathogenesis matter? J Trauma 59(6):1414–1419
Balain B, Eisenstein SM, Alo GO et al (2006) Coccygectomy for coccygodynia: case series and review of literature. Spine (Phila Pa 1976) 31(13):E414–E420
Mouhsine E, Garofalo R, Chevalley F et al (2006) Post-traumatic coccygeal instability. Spine J 6(5):544–549
Capar B, Akpinar N, Kutluay E et al (2007) Coccygectomy in patients with coccygodynia. Acta Orthop Traumatol Turc 41(4):277–280
Sehirlioglu A, Ozturk C, Oguz E et al (2007) Coccygectomy in the surgical treatment of traumatic coccygodynia. Injury 38(2):182–187
Cebesoy O, Guclu B, Kose KC et al (2007) Coccygectomy for coccygodynia: do we really have to wait? Injury 38(10):1183–1188
Traub S, Glaser J, Manino B (2009) Coccygectomy for the treatment of therapy-resistant coccygodynia. J Surg Orthop Adv 18(3):147–149
Fairbank JCT, Couper J, Davies JB et al (1980) The Oswestry low back pain questionnaire. Physiotherapy 66:271–273
Fogel GR, Cunningham PY 3rd, Esses SI (2004) Coccygodynia: evaluation and management. J Am Acad Orthop Surg 12(1):49–54
García FJ, Franco JD, Márquez R et al (1998) Posterior hernia of the rectum after coccygectomy. Eur J Surg 164(10):793–794
Kim NH, Suk KS (1999) Clinical and radiological differences between traumatic and idiopathic coccygodynia. Yonsei Med J 49:215–220
Grassi R, Lombardi G, Reginelli A et al (2007) Coccygeal movement: assessment with dynamic MRI. Eur J Radiol 61(3):473–479
Mazza L, Formento E, Fonda G (2004) Anorectal and perineal pain: new pathophysiological hypothesis. Tech Coloproctol 8(2):77–83
Parks AG, Porter NH, Hardcastle J (1966) The syndrome of the descending perineum. Proc R Soc Med 59(6):477–482
Sinaki M, Merritt JL, Stillwell GK (1977) Tension myalgia of the pelvic floor. Mayo Clin Proc 52(11):717–722
Acknowledgments
Mr. Nikolaos Kanakaris and Mrs. Despoina Kakagia made the appropriate corrections as linguistic personnel.
Conflict of interest
No funds were received in support of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Karadimas, E.J., Trypsiannis, G. & Giannoudis, P.V. Surgical treatment of coccygodynia: an analytic review of the literature. Eur Spine J 20, 698–705 (2011). https://doi.org/10.1007/s00586-010-1617-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-010-1617-1