
Abstract
The objective of this study is to evaluate the efficacy of corticosteroids in patients with radicular pain due to lumbar disc herniation or lumbar spinal stenosis through a prospective randomised, double blind controlled trial, and whether there was an effect on subsequent interventions such as additional root blocks or surgery. Peri-radicular infiltration of corticosteroids has previously been shown to offer no additional benefit in patients with sciatica compared to local anaesthetic alone. It is not known if the response to peri-radicular infiltration is less marked in certain subgroups of patients such as those with radicular pain due to lumbar spinal stenosis. Previous studies have suggested that peri-radicular infiltration of corticosteroids may obviate the need for subsequent interventions and we therefore further investigated this in the current study. We randomised 150 patients to receive a single injection with either bupivacaine alone or bupivacaine and methylprednisolone. Patients were assessed at 6 weeks and 3 months after the injection using standard outcome measures including Oswestry Disability Index (ODI), visual analogue score for leg pain and patient’s subjective assessment of outcome. At 1-year follow-up, we looked at the outcome in terms of the need for subsequent interventions such as additional root blocks or surgery. At 3-month follow-up, there was no statistically significant difference in the standard outcome measures between the two injection groups. At a minimum 1-year post injection, there was no difference in the need for subsequent interventions in either group. Patients with lumbar spinal stenosis had a less marked reduction in the ODI at 3 months with a mean change of 3.3 points when compared with 15 points for patients with lumbar disc herniation. In conclusion, peri-radicular infiltration of corticosteroids for sciatica does not provide any additional benefit when compared to local anaesthetic injection alone. Corticosteroids do not obviate the need for subsequent interventions such as additional root blocks or surgery.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sciatic pain is a common cause of disability in the adult population. It is most often caused by lumbar disc herniation and presents as pain radiating from the back into the leg usually in a dermatomal pattern corresponding to the compressed nerve root. The majority of patients with sciatic pain improve over time with conservative treatment [23, 24]. There are, however, a subgroup of patients who fail to respond to such conservative treatment. Peri-radicular infiltration of local anaesthetic with or without steroid has previously been shown to be of some benefit in this group of patients [7–9, 11, 16, 19, 21]. There is also evidence that along with compression of the nerve root, there is a strong inflammatory reaction to the herniated nucleus pulposus and therefore peri-radicular infiltration of corticosteroids would seem like a reasonable treatment option [13–15]. Another common cause of sciatic pain is lumbar foraminal stenosis causing compression of a particular nerve root. There is some evidence that outcomes of peri-radicular infiltration in patients with foraminal stenosis are intermediate compared with those observed for herniated discs [18].
The lack of efficacy of steroids in peri-radicular infiltration for radicular pain has previously been demonstrated by our initial study [11], but there is a possibility that there may be some benefit in a subgroup of patients. The purpose of this study was to investigate whether corticosteroids have any benefit in specific subgroups of patients with radicular pain, namely those with a diagnosis of disc herniation or foraminal stenosis. We also looked at the 1 year results to see if there is any effect of steroids on additional procedures such as additional peri-radicular infiltration or surgery.
Materials and methods
Patients were recruited from a specialist spine clinic from November 2001 to June 2005. One hundred and fifty patients with unilateral leg pain and MRI confirmed nerve root compression, due to either lumbar disc herniation or foraminal stenosis were included. The inclusion and exclusion criteria are listed in Table 1 below. All patients had completed at least 6 weeks of conservative treatment with analgesia and physical therapy with no apparent benefit. Patients enrolled into the trial agreed not to alter their oral analgesic medication during the follow-up period and did not have any additional treatments such as physiotherapy during the trial. The trial was given ethical approval by the Leicestershire Local Research Ethics committee (LREC; Ref No: 5087). At trial enrolment, an information sheet describing the trial was given to the patients and informed consent was obtained from all patients prior to trial entry. Patients then completed a standard spine assessment questionnaire, including 100 mm visual analogue score (VAS) for back and leg pain, Oswestry Disability Index (ODI) [4, 17] and low back outcome score (LBOS) [5, 6]. Psychological testing involved use of the modified somatic perception questionnaire and the modified zung depression score (MZD). Subjective outcome was also assessed at each follow-up visit. A 10% reduction in the ODI was considered to be a clinically significant change and a 20 mm change in the VAS was also considered clinically significant. Patients were assessed at enrolment and subsequently at 6 weeks, 12 weeks and finally at 1 year after the procedure. At 1-year follow-up, the outcome was assessed in terms of the need for surgery or further root blocks. The need for further intervention was based on significant residual leg pain.
Treatment procedure
The patients were randomised to receive either 2 ml of 0.25% bupivacaine alone or 2 ml of 0.25% bupivacaine and 40 mg of methylprednisolone (depomedrone). The randomisation was generated from a table of random numbers. To ensure that the treatment agents were concealed from the surgeon performing the procedure the syringe with the treatment agents was wrapped with opaque tape. The peri-radicular infiltration was performed in a clean air theatre as a day case procedure. The same senior surgeon performed all of the procedures. The patients were prone on the operating table and a spinal needle was used to approach the nerve root under fluoroscopic guidance. Once a satisfactory position of the needle was confirmed on both antero-posterior and lateral projections, Niopam 300 contrast medium was injected to confirm a satisfactory neurogram. The treatment agent was then injected slowly around the nerve root.
Statistical analysis
A sample size of 150 patients was calculated to be sufficient to detect a 10% difference on the ODI between the patients in the subgroups, i.e. those with lumbar disc herniation and those with foraminal stenosis allowing for an alpha error of 0.05. An independent samples t test was used to examine the differences in the outcome measures between the two groups. Multiple regression analysis was used to determine if the MSP, MZD, age or duration of radicular pain had any effect on outcome. A χ 2 test was used to determine if there was any difference in the rates of surgery or further root blocks in either the bupivacaine only or bupivacaine and steroid group. The data was analysed using SPSS statistical software version 11.5 (SPSS Inc., Chicago, IL, USA).
Results
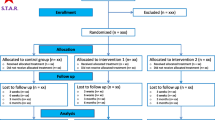
A total of 150 patients were recruited into the trial. There were 76 patients who received bupivacaine alone and 74 patients who received bupivacaine and steroid. Three patients were excluded from the trial due to blinding failures after the treatment agents leaked during administration. A further five patients were listed for surgery prior to 3 months follow-up. One patient had no improvement at 6 weeks follow-up and had a repeat root block at that stage. Therefore at 6 weeks follow-up, data was available for 141 patients (94%). Sixteen patients did not attend for review at the 3 month follow-up. Complete data at 3 months was therefore available for 124 patients (83%). At a minimum of 1 year follow-up two patients had died and data was available for 129 patients (86%). There were no complications of the procedure reported by any of the patients. The mean change in ODI was 10.7 points in the bupivacaine only group and 9.3 points in the bupivacaine and steroid group. This difference was not statistically significant (P = 0.69). Both groups had a mean of at least 20 mm change in the VAS for leg pain. Subgroup analysis revealed that there was a greater reduction in the ODI in patients with lumbar disc herniation, with a mean change of 15.0 points (SD 20.7) when compared with only 3.3 points (SD 14.6) in patients with spinal stenosis. There was a mean change in the VAS of 26 mm (SD 31) in the disc prolapse group when compared with 21 mm (SD 28) in the spinal stenosis group. The results are summarised in Tables 2, 3, 4, 5, 6, 7, 8, 9 below. There was a minimum of 10 points change in the ODI in 54% of patients in the disc prolapse group and 44% of patients in the spinal stenosis group. There was a minimum of 20 mm change in the VAS in 58% of patients with a disc prolapse and 52% of patients with spinal stenosis as the underlying diagnosis. When looking at subjective outcome, 54% of patients reported an excellent or good outcome in the disc prolapse group and 42% of patients reported an excellent or good outcome in the spinal stenosis group (Table 6, Fig. 1 below).

Graph comparing the subjective outcome between the disc prolapse and spinal stenosis groups
The results for the change in ODI, VAS for leg pain and LBOS are shown in Table 4 below. Independent samples t tests confirmed that there was no statistically significant difference in the results between the two groups.
Table 5 shows the mean change in outcome scores between the four subgroups in the trial. One-way analysis of variance did show that there was a statistically significant difference for the change in ODI, which just achieved significance, but post hoc analysis did not reveal any significant difference among the four subgroups.
At a minimum follow-up of 1 year, median 20 months (12–31 months), data regarding outcome was available for 129 patients. χ 2 analysis did not reveal any statistically significant difference in the rates of further intervention in the form of surgery or further root blocks in either group of patients (Tables 7, 8).
The duration of symptoms was the only independent variable to correlate with a less favourable outcome at 3 months using the ODI as the dependent variable as shown in Table 9 above. Age at injection, modified somatic perception and MZD have no predictive value on the outcome at 3 months.
Discussion
Our study has demonstrated that peri-radicular infiltration of corticosteroids does not seem to produce any additional benefit compared to local anaesthetic alone in patients with sciatica, confirming the results of our previous study. In addition, subgroup analysis suggests that there is no statistically significant difference in the outcome between those with a diagnosis of lumbar disc herniation and foraminal stenosis. The belief that corticosteroids may reduce the inflammatory component of nerve root compression has led to their widespread use in both epidural injections and peri-radicular infiltration. A lack of efficacy of steroids was first observed in a randomised controlled trial by Cuckler et al. [3] who demonstrated that epidural steroids did not produce any additional benefit compared to local anaesthetic alone. This study also found that there was no significant difference in outcome among patients with a diagnosis of lumbar disc herniation or lumbar spinal stenosis. The exact mechanism of action of corticosteroids in radicular pain is unknown, but it is known that along with mechanical compression of nerve roots, sciatica is caused by ectopic firing of nerve roots mediated by various chemical mediators. These include prostaglandin E2, a chemical mediator of inflammation, which provoked the ectopic firing of nerve roots in a canine model used in one study [10]. Triamcinalone acetonide, a steroid was shown in this study to suppress the ectopic firing of nerve roots induced by prostaglandin E2, suggesting that steroids may be useful in alleviating the chemical irritation of nerve roots and hence radicular pain.
It has been suggested by Karpinnen et al. [7] that peri-radicular infiltration of corticosteroids produces a short-term benefit in terms of improvement in leg pain. This randomised study found that leg pain improved at 2 weeks by 45% in the steroid group when compared with 24% in the saline group, but at 3, 6 months and 1 year after the injection there was no treatment effect of steroids over saline. In fact, this study found that there was a rebound deterioration at 3 and 6 months in the steroid group. The authors carried out a further study [1] on the same population to evaluate this and found that peri-radicular corticosteroid did not negatively affect the spontaneous resorption of herniated nucleus pulposus as demonstrated by serial MRI scanning. In our study, we found that at 6 and 12 weeks there was ongoing improvement in both the ODI and LBOS (Table 4). The VAS for leg pain also improved from 18.6 mm at 6 weeks to 22.6 mm at 12 weeks in the bupivacaine only group. There was a slight deterioration in the VAS for leg pain in the bupivacaine + steroid group from 26.1 mm at 6 weeks to 24.5 mm at 12 weeks. This would indicate that overall the initial improvement in the outcome measures at 6 weeks is maintained at the 3 month follow-up.
Our study did show a trend towards a more marked improvement in patients with an underlying diagnosis of lumbar disc herniation as opposed to spinal stenosis. The mean ODI improved by 15 points in the disc herniation group, compared to only 3.3 points in the spinal stenosis group. However, when looking at the subjective outcome, 21% patients in the spinal stenosis group reported an excellent outcome when compared with only 14% of patients in the disc prolapse group. This may be due to the expectation of patients in the disc prolapse group, which may have been higher than those in the spinal stenosis group. When we analysed the subgroups of patients based on the underlying diagnosis and injection content (Table 5), we found that the ODI improved by only 1.5 points in patients with spinal stenosis receiving bupivacaine and steroid and 13.6 points in patients with a disc prolapse receiving the same injection. This result was statistically significant, but there were only 23 patients in the spinal stenosis group when compared with 42 patients in the disc prolapse group, making it difficult to draw any firm conclusions from this. There is also the possibility of a type 1 error occurring due to the effect of multiple subgroup analyses performed as reported recently by Wang et al. [22]. When looking at the outcome in terms of VAS for leg pain (Table 5), we found that the differences between the groups were less marked, in fact there was a significant improvement in all groups ranging from 19.1 (spinal stenosis group receiving bupivacaine + steroid) to 27.4 mm (disc prolapse group receiving bupivacaine + steroid). This would indicate that peri-radicular infiltration does produce good pain relief in patients with radicular pain irrespective of the underlying diagnosis. Other studies have suggested that the effects of peri-radicular infiltration of steroids are less marked in patients with lumbar spinal stenosis. It has been suggested that this may be attributable to the multifactorial origin of stenosis symptoms, which may develop from impaired venous flow, restricted neural glide, inflammation or structural root injury [18]. In a study by Ng et al. [12], it was reported that patients with a diagnosis of spinal stenosis had a moderate response to root blocks when compared with patients with lumbar disc herniation, although 37% of patients in the spinal stenosis group had a 10% reduction in the ODI at 3 months post injection. This would concur with our findings of 44% of patients with spinal stenosis achieving a 10% reduction in the ODI.
A recent systematic review of conservative treatments for radicular pain found that when comparing epidural corticosteroid injection to no treatment there was no difference in overall improvement in the short term and no difference regarding return to work at intermediate follow-up [8]. There is also evidence to suggest that targeting a selected nerve root for injection under fluoroscopic guidance may result in better pain relief. This was confirmed by a study by Thomas et al. [20] who found that transforaminal epidural corticosteroid injection with radioscopic control provided better pain relief (VAS) and improvement in disability compared to epidural corticosteroid without radioscopic control.
Our study has also shown that at a minimum of 1-year follow-up, there is no difference in the rates of further interventions in either group of patients. This is contrary to a study by Riew et al. [16], which concluded that selective nerve root injections of corticosteroids are significantly more effective than those of bupivacaine alone in obviating the need for operative intervention. They found that 67% of patients receiving local anaesthetic alone needed operative intervention when compared with 29% of patients receiving local anaesthetic and corticosteroid. In our study, the overall rate of surgery was 18%, which is much lower than that reported by Riew et al. In our study, in the bupivacaine only group the rate of surgery was 22% when compared with 14% in the bupivacaine and steroid group. χ 2 analysis showed that this difference was not statistically significant (P = 0.38).
A study by Carette et al. [2] also found that epidural corticosteroids only provided short-term benefit in patients with sciatica due to a prolapsed disc. This study compared epidural corticosteroids with placebo (saline) injection and at 6 weeks found that the improvement in leg pain was greater in the epidural corticosteroid group. At 3 months, there was no significant difference in outcome between the groups. At 1-year follow-up the rate of surgery was also similar in both groups (25.8% in the corticosteroid group vs. 24.8% in the placebo group). This would concur with our findings that corticosteroids do not provide any long-term benefit in terms of the need for operative intervention.
Conclusion
Peri-radicular infiltration of corticosteroids for sciatica does not provide any additional benefit when compared with local anaesthetic injection alone. The procedure is effective in terms of pain relief in patients with a diagnosis of a prolapsed disc as well as patients with foraminal stenosis, but there seems to be a less marked response in the latter group. Peri-radicular infiltration is also effective in terms of the need for further intervention in the form of surgery with only 18% of patients requiring surgery at a minimum of 1 year after the injection. There is no additional benefit in the addition of steroid to obviate the need for further root blocks or surgery.
References
Autio RA, Karpinnen J, Kurunlahti M (2004) Effect of periradicular methylprednisolone on spontaneous resorption of intervertebral disc herniations. Spine 29(15):1601–1607. doi:10.1097/01.BRS.0000132511.46818.67
Carette S, Leclaire R, Marcoux S et al (1997) Epidural corticosteroid injections for sciatica due to herniated nucleus pulposus. N Engl J Med 336(23):1634–1640. doi:10.1056/NEJM199706053362303
Cuckler JM, Bernini PA, Wiesel SW et al (1985) The use of epidural steroids in the treatment of lumbar radicular pain. A prospective, randomised, double-blind study. J Bone Joint Surg Am 67-A(1):63–66
Fairbank J, Couper J, Davies JB et al (1980) The Oswestry low back pain disability questionnaire. Physiotherapy 66:271–273
Greenough CG, Fraser RD (1992) Assessment of outcome in patients with low back pain. Spine 17:36–41. doi:10.1097/00007632-199201000-00006
Holt AE, Shaw NJ, Shetty A, Greenough CG (2002) The reliability of the low back outcome score for back pain. Spine 27(2):206–210
Karpinnen J, Malmivaara A, Kurunlahti M (2001) Periradicular infiltration for sciatica. A randomised controlled trial. Spine 26(9):1059–1067. doi:10.1097/00007632-200105010-00015
Luijsterburg PAJ, Verhagen AP, Ostelo RWJG et al (2007) Effectiveness of conservative treatments for the lumbosacral radicular syndrome: a systematic review. Eur Spine J 16:881–899. doi:10.1007/s00586-007-0367-1
Lutz GE, Vad VB, Wisneski RJ (1998) Fluoroscopic transforaminal epidural steroids, an outcome study. Arch Phys Med Rehabil 79:1362–1366. doi:10.1016/S0003-9993(98)90228-3
Muramoto T, Atsuta Y, Iwahara T (1997) The action of prostaglandin E2 and triamcinolone acetonide on the firing activity of lumbar nerve roots. Int Orthop 21(3):172–175. doi:10.1007/s002640050144
Ng L, Chaudhary N, Sell P (2005) The efficacy of corticosteroids in periradicular infiltration for chronic radicular pain. A randomised, double-blind, controlled trial. Spine 30(8):857–862. doi:10.1097/01.brs.0000158878.93445.a0
Ng L, Sell P (2004) Predictive value of the duration of sciatica for lumbar discectomy, a prospective cohort study. J Bone Joint Surg Br 86-B(4):546–549
Olmarker K, Blomquist J, Stromberg J et al (1995) Inflammatogenic properties of nucleus pulposus. Spine 20:665–669. doi:10.1097/00007632-199503150-00006
Olmarker K, Byrod G, Cornefjord M et al (1994) Effects of methylprednisolone on nucleus pulposus-induced nerve root injury. Spine 19:1803–1808. doi:10.1097/00007632-199408150-00003
Olmarker K, Rydevik B, Nordborg C (1993) Autologous nucleus pulposus induces neurophysiologic and histologic changes in porcine cauda equine nerve roots. Spine 18:1425–1432
Riew DK, Yin Y, Gilula L et al (2000) The effect of nerve root injections on the need for operative treatment of lumbar radicular pain: a prospective, randomised, controlled, double-blind study. J Bone Joint Surg Am 82-A(11):1589–1593
Roland M, Fairbank J (2000) The Roland-Morris Disability Questionnaire and the Oswestry Disability Questionnaire. Spine 25(24):3115–3124. doi:10.1097/00007632-200012150-00006
Slipman CW, Chow DW (2002) Therapeutic spinal corticosteroid injections for the management of radiculopathies. Phys Med Rehabil Clin N Am 13(3):697–711
Tajima T, Fuukawa K, Kuramochi E (1980) Selective lumbosacral radiculopathy and block. Spine 5:68–77. doi:10.1097/00007632-198001000-00013
Thomas E, Cyteval C, Abiad L et al (2003) Efficacy of transforaminal versus interspinous corticosteroid injection in discal radiuculagia—a prospective, randomised, double-blind study. Clin Rheumatol 22:299–304. doi:10.1007/s10067-003-0736-z
Vad VB, Bhat AL, Lutz GE et al (2002) Transforaminal epidural steroid injections in lumbosacral radiculopathy: a prospective randomised study. Spine 27:11–16. doi:10.1097/00007632-200201010-00005
Wang R, Lagakos SW, Ware JH (2007) Statistics in medicine—reporting of subgroup analyses in clinical trials. N Engl J Med 357(21):2189–2194. doi:10.1056/NEJMsr077003
Weber H (1994) The natural history of disc herniation and the influence of intervention. Spine 19:2234–2238
Weber H, Holme I, Amlie E (1993) The natural cause of acute sciatica with nerve root symptoms in a double-blind placebo controlled trial evaluating the effect of piroxicam. Spine 18:1433–1438. doi:10.1097/00007632-199312000-00021
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tafazal, S., Ng, L., Chaudhary, N. et al. Corticosteroids in peri-radicular infiltration for radicular pain: a randomised double blind controlled trial. One year results and subgroup analysis. Eur Spine J 18, 1220–1225 (2009). https://doi.org/10.1007/s00586-009-1000-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-009-1000-2