
Abstract
Background
Although recent reports indicate that K-ras mutation status is a biomarker that acts as a prognostic factor, only a few analyses of K-ras mutation subtypes have been published. In addition, there are no reports that analyze overall survival and prognostic factors according to K-ras mutation status and subtypes in only unresectable pancreatic cancer (PC) determined from tissues obtained by endoscopic ultrasound-guided fine-needle aspiration.
Methods
We retrospectively analyzed 242 patients who were diagnosed as having unresectable PC with available histological diagnosis. Clinical data collected included sex, age, Eastern Cooperative Oncology Group performance status, carbohydrate antigen (CA) 19-9, primary tumor location, stage (local or metastatic) according to TNM staging, first-line chemotherapy, K-ras mutation status and subtypes (G12D, G12V, and G12R), and overall survival. We analyzed the negative prognostic factors for reduced overall survival in unresectable PC patients using these data.
Results
From multivariate analysis, CA19-9 ≥1000 U/ml (hazard ratio [HR] 1.78, 95 % confidence interval [CI] 1.28–2.46, P < 0.01), metastatic stage (HR 2.26, 95 % CI 1.58–3.24, P < 0.01), and mutant-K-ras (HR 1.76, 95 % CI 1.03–3.01, P = 0.04) were negative prognostic factors, indicating a reduced survival. Among the patients who had K-ras mutation subtypes, CA19-9 ≥1000 U/ml (HR 1.65, 95 % CI 1.12–2.37, P < 0.01), metastatic stage (HR 2.12, 95 % CI 1.44–3.14, P < 0.01), and the presence of the G12D or G12R mutations (HR 1.60, 95 % CI 1.11–2.28) were negative prognostic factors for overall survival.
Conclusions
K-ras mutation status and subtypes may be associated with survival duration in pancreatic cancer patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prognosis of pancreatic cancer (PC) is one of the poorest among all malignancies. The 5-year survival rate among all patients with PC is <3.5 % [1, 2]. Because PC has such a poor prognosis, it would be advantageous to accurately predict treatment outcomes to prevent over-treating patients who would have little benefit from chemotherapy. The prognostic factors for unresectable pancreatic adenocarcinoma include serum carbohydrate antigen 19-9 (CA19-9), TNM staging, C-reactive protein, and baseline Karnofsky performance status (PS) [3–5]. Genetic abnormalities have been identified in PC patients, and K-ras mutations are found in approximately 90 % of PC patients [6, 7]. K-ras mutations have been examined as a possible prognostic factor for PC. Although recent reports indicate that K-ras mutation status is a biomarker that acts as a prognostic factor [8–10], only a few analyses of K-ras mutation subtypes have been published [11, 12]. These reports might include some false-negative cases, because the frequency of K-ras mutations was relatively low compared with previously reported frequencies [6, 7]. In addition, there have been no previously published analyses of the possible association between the prognosis of unresectable PC patients and the K-ras mutation subtype determined from tissues obtained by endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA).
We previously detected K-ras mutations in 266 (87 %) of 307 PC patients from tissues obtained by EUS-FNA [13]. This percentage is similar to previously published rates of K-ras mutations [6, 7]; therefore, the data from our K-ras analysis appear to be reliable.
The aim of the present study was to use data from our previous study to retrospectively determine whether K-ras mutation subtypes are prognostic factors in PC.
Methods
Patient selection
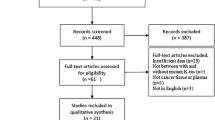
The Institutional Review Board at Aichi Cancer Center Hospital approved this study of K-ras mutation status in 394 consecutive patients who underwent EUS-FNA of pancreatic masses between March 2004 and September 2009. We retrospectively included 242 patients with histologically diagnosed PC, who were deemed unresectable. Patients who underwent surgical resection were excluded. In addition, patients whose EUS-FNA results were negative for malignancy and K-ras mutation were excluded because of the possibility of false-negative results.
All patients provided written informed consent to all procedures associated with the study.
Clinical data
The clinical data collected included sex, age, Eastern Cooperative Oncology Group (ECOG) performance status (PS), CA19-9, primary tumor location, stage (local or metastatic) according to TNM staging, first-line chemotherapy, K-ras mutation and subtypes, and overall survival (OS). The primary endpoint of this study was OS. Because the G12D, G12V, and G12R subtypes comprised almost all of the K-ras mutations, we focused on these three subtypes in this study.
EUS-FNA technique
We imaged the pancreas at 7.5-MHz frequency using a convex linear-array echoendoscope (GF-UGT240; Olympus Optical, Tokyo, Japan) connected to an ultrasound device (SSD5500; Aloka, Tokyo, Japan) and a 22-gauge needle (NA-10J or NA-11J-KB, Olympus Optical; or an EchoTip-Ultra Needle; Cook Medical, Limerick, Ireland), as previously described [14, 15]. The aspirated material was separated for cytopathological evaluation, cell-block preparation, and K-ras mutation analysis. The aspirated material was immediately evaluated (Diff Quick Staining, Baxter, Miami, FL, USA) by a cytopathologist and/or cytotechnologist for rapid diagnosis. Material was directly fixed in 10 % formalin in a standard specimen bottle, centrifuged, and then embedded in paraffin for cell-block analysis. Sections were visualized by hematoxylin and eosin (HE) staining, as well as immunohistochemical staining if necessary.
Analysis of K-ras mutations
The genetic analysis was performed with material obtained from EUS-FNA (either fresh specimens or paraffin-embedded tissues). Total RNA was extracted from the fresh specimens, and mutational analysis was performed using reverse transcription polymerase chain reaction (RT-PCR)-coupled direct sequencing methods, as described previously [16]. When the direct sequencing displayed no mutational signal although the cytological diagnosis was atypical cells, suspicious of adenocarcinoma, we further investigated K-ras mutation, using the corresponding cell-block slides, by performing a Cycleave PCR assay (TAKARA, Co., Ltd., Ohtsu, Japan) [17]. This assay is highly sensitive and can detect as little as 5 % tumor cells mixed with normal tissues.
Statistical analysis
Continuous variables were expressed as median values. Incidences and concordance between groups were compared using the χ 2 test, Mann–Whitney U-test, and Kruskal–Wallis test where appropriate. OS was measured from the day that PC was histologically diagnosed by EUS-FNA to the time of death or last follow-up examination. Survival rates were calculated using the Kaplan–Meier method [18]. The stratified log-rank test was used to compare survival curves, and censored data were taken into account [19]. Both univariate and multivariate analyses were used to examine potential prognostic factors. The Cox proportional hazards model was used to determine the most significant variables contributing to survival [20]. Differences with a P value of less than 0.05 were considered statistically significant. All analyses were performed with SPSS version 11.0 (SPSS, Chicago, IL, USA) statistical software.
Results
Patient characteristics
The patient characteristics according to K-ras mutation status in 242 patients with unresectable PC are shown in Table 1. Among the 242 patients, 214 (88.4 %) patients had mutant K-ras, and 28 (11.6 %) patients had wild-type K-ras. Among the 214 patients with K-ras mutations, the most common subtypes were G12D (92 patients; 42.9 %), G12V (85 patients; 39.7 %), and G12R (17 patients; 7.9 %). Less common K-ras mutations were in codon 13 (n = 1) or codon 61 (n = 5), while 10 patients had unknown K-ras mutations. There were no significant differences between the sex distribution or median ages of the patients with different mutation subtypes, or between patients with mutant and wild-type K-ras genes. Sixteen patients had a PS of ≥2 (6.6 %) and 226 had a PS of <2 (93.4 %). CA19-9 levels, primary tumor location, and tumor stage (local or metastatic) were not related to the different mutation subtypes, or to the presence of mutant or wild-type-K-ras genes. A total of 86 % of patients with the wild-type-K-ras gene, and 80 % of patients with the mutant K-ras gene were treated with gemcitabine (GEM). Patients who were not treated with GEM received titanium silicate (TS)-1, a combination of 5-fluorouracil and radiation, or no therapy. There were no significant differences in the treatment modalities among the different mutation subtype groups, or between the mutant and wild-type-K-ras gene groups.
Survival according to K-ras mutation and subtypes
Overall survival was examined with Kaplan–Meier plots and log-rank tests, as shown in Figs. 1 and 2. The median OS was 261 days for the entire group of PC patients. When analyzed by K-ras mutation status, the median OS was significantly longer in the wild-type group (479 days) than in the mutant group (255 days; P = 0.03). Moreover, the median OS values were significantly different (P < 0.01) among the patients who had the three most common K-ras mutations: G12D (242 days), G12 V (338 days), and G12R (204 days). Patients who had the G12 V mutation had a significantly longer OS than patients with G12D (P = 0.01) or G12R (P < 0.01). There was no statistically significant difference between the OS of the G12D and G12R subgroups (P = 0.13).

Overall survival (OS) in all patients was examined with Kaplan–Meier plots and log-rank tests. The median OS was significantly longer in the wild-type group (479 days) than in the mutant group (255 days; P = 0.03)

Overall survival (OS) in patients who had the K-ras mutation subtypes, G12D, G12V, and G12R was examined with Kaplan–Meier plots and log-rank tests. Patients who had the G12V mutation had a significantly longer OS than patients with G12D (P = 0.01) or G12R (P < 0.01)
Univariate and multivariate analyses
The results of univariate and multivariate analyses are listed in Table 2 (according to wild-type vs mutant) and Table 3 (according to K-ras mutation subtype). Univariate analysis revealed that the negative prognostic factors for OS were PS ≥2 (hazard ratio [HR] 2.58, 95 % confidence interval [CI] 1.46–4.55, P < 0.01), CA19-9 ≥1000 U/ml (HR 1.95, 95 % CI 1.42–2.69, P < 0.01), and metastatic stage (HR 2.44, 95 % CI 1.72–3.45, P < 0.01). Patients with a mutant K-ras gene had a shorter survival than patients with the wild-type gene (HR 1.78, 95 % CI 1.08–2.95, P = 0.03). Interestingly, patients with the G12D or G12R mutation had a shorter survival than patients with the G12V mutation (HR 1.72, 95 % CI 1.22–2.43, P < 0.01).
The multivariate analysis performed according to K-ras mutation revealed that CA19-9 ≥1000 U/ml (HR 1.78, 95 % CI 1.28–2.46, P < 0.01) and metastatic stage (HR 2.26, 95 % CI 1.58–3.24, P < 0.01) were negative prognostic factors for OS. In addition, the presence of a mutant K-ras gene (HR 1.76, 95 % CI 1.03–3.01, P = 0.04) was a negative prognostic factor for OS. According to the K-ras mutation subtype, CA19-9 ≥1000 U/ml (HR 1.65, 95 % CI 1.12–2.37, P < 0.01) and metastatic stage (HR 2.12, 95 % CI 1.44–3.14, P < 0.01) were also negative prognostic factors for OS. Regarding K-ras mutation subtypes, G12D and G12R (HR 1.60, 95 % CI 1.11–2.28) were negative prognostic factors for OS.
Discussion
Various genetic abnormalities in K-ras, p53, p16, and DPC4 have been demonstrated in PC [6, 7, 21–23]. K-ras is the most common mutationally activated human oncoprotein, and K-ras mutations account for 90 % of the mutations in PC. In advanced colon cancer, K-ras mutation status and subtypes are extremely useful in predicting the therapeutic efficacy of chemotherapy and identifying patients with poor prognosis [24]. Therefore, we used our previously collected data on the incidence and subtypes of K-ras mutation in PC [13] to clarify the relationship between K-ras mutations and clinicopathological features. There were no significant differences in the treatment modalities used for the patients with wild-type and those with mutant K-ras. In addition, in patients thought to have a high response rate to chemotherapy based on tumor markers and diagnostic imaging data, the wild-type gene was present in 29 % and the mutant type in 14 %. Divided by subtype, G12D was present in 10 %, G12V in 21 %, and G12R in 6 %. These data suggest that patients with wild-type K-ras or G12V have better response rates to chemotherapy. It should be noted, however, that these data were only retrospective, and prospective analysis conforming strictly to Response Evaluation Criteria in Solid Tumors (RECIST) [25] is required.
Compared with previous studies [8–12], the present study included the largest number of patients, and, to the best of our knowledge, it is the first study to analyze OS and prognostic factors according to K-ras mutation status and subtypes in only unresectable PC using EUS-FNA materials. However, the present study does have several limitations, such as the retrospective design and patient selection bias.
In univariate analyses, PS, CA19-9, stage, and K-ras mutation and subtypes were indentified as significant predictors of poor prognosis. In addition, these factors had independent prognostic value in a multivariate analysis without PS. Although various factors other than K-ras are also important for prognostication, K-ras mutation analysis may be particularly useful for predicting prognosis in PC patients with local-stage, PS 0, or low serum levels of CA19-9. Patients without K-ras mutation survived significantly longer than patients with K-ras mutation. Among the patients with K-ras mutations, patients with the G12V mutation had a significantly longer OS as compared with the patients with the G12D or G12R mutations. These results are consistent with the results of previous studies [6, 7, 11, 26]. The frequency of K-ras mutation in our cohort was very similar to previously reported frequencies, and the distribution of K-ras mutation subtypes was also similar to distributions in other studies. The most common alteration in codon 12 of K-ras was G12D, followed by G12V and then G12R. Moreover, our results for OS by mutation subtype and the presence or absence of K-ras mutation were similar to previously reported results [9–12]. Immervoll et al. [12] previously suggested that mutation subtype could be associated with survival. In their study of resected PC patients, patients with the G12V mutation had a longer median survival period (23.5 months) than patients with G12D (9.5 months), who lived longer than patients with G12R (7.5 months). Likewise, Kawesha et al. [11] also demonstrated a longer median survival period in patients with G12V (12.5 months) than than in those with G12D (8.7 months) or G12R (6.7 months). In a study of colorectal cancer patients, Span et al. [27] demonstrated that patients with G12D and G12R tended to have a worse prognosis than patients with G12V.
However, in the RASCAL project, which analyzed 2271 colorectal cancer patients from 22 groups in 13 countries, G12V was associated with a greater risk of relapse and death than other mutations [28]. Studies of lung carcinoma have also concluded that patients with the G12V mutation have a poorer prognosis than patients with G12D [29, 30]. These results are supported by sound experimental evidence. The basal GTPase activity of the G12V mutant is one-quarter that of the G12D mutant and one-tenth that of wild-type K-ras [31, 32]. In addition, Al-Mulla and Mackenzie [33] found that Rat-1 cells containing G12V mutant K-ras were significantly more invasive in vitro than clones containing the G12D mutation or wild-type K-ras. The G12V-expressing cells had a greater ability to invade Matrigel than cells expressing the G12D mutant or wild-type K-ras. However, although they also pointed out that the biological effects of G12V, G12D, and wild-type K-ras cannot be assumed to be the same, mutant K-ras and wild-type K-ras have been associated with different degrees of biological aggression in the abovementioned basic experiments, which may also be reflected in prognosis in PC patients.
In conclusion, we analyzed prognostic factors including K-ras mutation status and subtypes in PC patients. This study is the largest of its kind yet to be published; also, this is the first analysis of unresectable PC performed with tissue obtained by EUS-FNA. Differences in the survival of PC patients cannot be completely explained on the basis of K-ras mutation status and subtype. However, according to our study, the K-ras mutation status and specific subtypes may be important factors associated with survival in PC patients. Our results need to be validated by future prospective studies with the analysis of more prognostic factors and more detailed oncogene analyses.
References
Gudjonsson B. Cancer of the pancreas: 50 years of surgery. Cancer. 1987;60:2284–303.
Warshaw AL. Fernandez del Castillo C. Pancreatic carcinoma. N Engl J Med. 1992;326:455–65.
Krishnan S, Rana V, Janjan NA, Abbruzzese JL, Gould MS, Das P, et al. Prognostic factors in patients with unresectable locally advanced pancreatic adenocarcinoma treated with chemoradiation. Cancer. 2006;107:2589–96.
Koom WS, Seong J, Kim YB, Pyun HO, Song SY. CA19-9 as a predictor for response and survival in advanced pancreatic cancer patients treated with chemoradiotherapy. Int J Radiat Oncol Biol Phys. 2009;73:1148–54.
Sawaki A, Kanemitsu Y, Mizuno N, Takahashi K, Nakamura T, Ioka T, et al. Practical prognosis index for patients with metastatic pancreatic cancer treated with gemcitabine. J Gastroenterol Hepatol. 2008;23:1292–7.
Almoguera C, Shibata D, Forrester K, Martin J, Arnheim N, Perucho M. Most human carcinomas of the exocrine pancreas contain mutant c-K-ras genes. Cell. 1988;53:549–54.
Tada M, Omata M, Ohto M. Clinical application of ras gene mutation for diagnosis of pancreatic adenocarcinoma. Gastroenterology. 1991;100:233–8.
Kullmann F, Hartmann A, Stohr R, Messmann H, Dollinger MM, Trojan J, et al. KRAS mutation in metastatic pancreatic ductal adenocarcinoma: results of a multicenter phase II study evaluating efficacy of cetuximab plus gemcitabine/oxaliplatin (GEMOXCET) in first-line therapy. Oncology. 2011;81:3–8.
Lee J, Jang KT, Ki CS, Lim T, Park YS, Lim HY, et al. Impact of epidermal growth factor receptor (EGFR) kinase mutations, EGFR gene amplifications, and KRAS mutations on survival of pancreatic adenocarcinoma. Cancer. 2007;109:1561–9.
Chen H, Tu H, Meng ZQ, Chen Z, Wang P, Liu LM. K-ras mutational status predicts poor prognosis in unresectable pancreatic cancer. Eur J Surg Oncol. 2010;36:657–62.
Kawesha A, Ghaneh P, Andren-Sandberg A, Ograed D, Skar R, Dawiskiba S, et al. K-ras oncogene subtype mutations are associated with survival but not expression of p53, p16(INK4A), p21(WAF-1), cyclin D1, erbB-2 and erbB-3 in resected pancreatic ductal adenocarcinoma. Int J Cancer. 2000;89:469–74.
Immervoll H, Hoem D, Kuqarajh K, Steine SJ, Molven A. Molecular analysis of the EGFR-RAS-RAF pathway in pancreatic ductal adenocarcinomas: lack of mutations in the BRAF and EGFR genes. Virchows Arch. 2006;448:788–96.
Ogura T, Yamao K, Sawaki A, Mizuno M, Hara K, et al. Clinical impact of K-ras mutation analysis in Endoscopic ultrasound-guided fine needle aspiration specimens from pancreatic masses. Gastrointest Endosc. 2012;75:769–74.
Chang KJ, Nguyen P, Erickson RA, Durbin TE, Katz KD. The clinical utility of endoscopic ultrasound-guided fine needle aspiration in the diagnosis and staging of pancreatic carcinoma. Gastrointest Endosc. 1997;45:387–93.
Yamao K, Sawaki A, Mizuno N, Shimizu Y, Yatabe Y, Koshikawa T. Endoscopic ultrasound-guided fine-needle aspiration biopsy (EUS-FNAB): past, present, and future. J Gastroenterol. 2005;40:1013–23.
Yatabe Y, Koqa T, Mitsudomi T, Takahashi T. CK20 expression, CDX2 expression, K-ras mutation, and goblet cell morphology in a subset of lung adenocarcinomas. J Pathol. 2004;203:645–52.
Yatabe Y, Hida T, Horio Y, Kosaka T, Takahashi T, Mitudomi T. A rapid, sensitive assay to detect EGFR mutation in small biopsy specimens from lung cancer. J Mol Diagn. 2006;8:335–41.
Kaplan E, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:1413–7.
Mantel N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep. 1966;50:163–70.
Cox DR. Regression models and life-tables. J R Stat Soc B. 1984;34:588–91.
Rozenblum E, Shutte M, Goggins M, Hahn SA, Panzer S, Zahurak M, et al. Tumor-suppressive pathways in pancreatic carcinoma. Cancer Res. 1997;57:1731–4.
Hiyama E, Kodama T, Shinbara K, Iwao T, Itho M, Hiyama K, et al. Telomerase activity is deleted in pancreatic cancer but not in benign tumors. Cancer Res. 1997;57:326–31.
Koorstra JBM, Hustinx SR, Offerhaus GJA, Maitra A. Pancreatic carcinogenesis. Pancreatology. 2008;8:110–25.
Karapetis CS, Khambata-Ford S, Jonker DJ, O’Callaghan CJ, Tu D, Tebutt NC, et al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer. N Engl J Med. 2008;359:1757–65.
Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors: European Organization for Research and Treatment of Cancer, National Cancer Institute of United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92:205–16.
Hruban RH, Goggins M, Parsons J, Kem SE. Progression model for pancreatic cancer. Clin Cancer Res. 2000;6:2969–72.
Span M, Moerkerek PT, De Goeij AF, Arends JW. A detailed analysis of K-ras point mutations in relation to tumor progression and survival in colorectal cancer patients. Int J Cancer. 1996;69:241–5.
Andreyev NJH, Norman AR, Cunningham D, Oates J, Dix BR, Dix BR, Iacopetta BJ, et al. Kirsten ras mutations in patients with colorectal cancer: the multicenter ‘RASCAL’ study. Br J Cancer. 2001;85:692–6.
Vega J, Iniesta P, Caldes T, Sanchez A, Lopez J, Dejuan C, et al. Association of K-ras codon 12 transversions with short survival in non-small cell lung cancer. Int J Oncol. 1996;9:1307–11.
Keohavong P, Demichele MAA, Melacrions AC, Landreneau RJ, Weyant RJ, Siegfried JM. Detection of K-ras mutations in lung carcinomas-relationship to prognosis. Clin Cancer Res. 1999;2:411–8.
John J, Frech M, Wittinghofer A. Biochemical properties of Ha-ras encoded p21 mutants and mechanism of the autophosphorylation resection. J Biol Chem. 1998;263:792–9.
Krengle U, Schlichting L, Scherer A, Schumann R, Frech M, John J, et al. Three-dimensional structures of H-ras p21 mutants: molecular basis for their inability to function as signal switch molecules. J Biol Chem. 1989;264:86–92.
Al-Mulla F, Mackenzie EM. Differences in in vitro invasive capacity induced by differences in Ki-Ras protein mutations. J Pathol. 2001;195:549–56.
Conflict of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ogura, T., Yamao, K., Hara, K. et al. Prognostic value of K-ras mutation status and subtypes in endoscopic ultrasound-guided fine-needle aspiration specimens from patients with unresectable pancreatic cancer. J Gastroenterol 48, 640–646 (2013). https://doi.org/10.1007/s00535-012-0664-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-012-0664-2