
Abstract
Background
Patients with branch duct type intraductal papillary mucinous neoplasm (BD-IPMN) without invasion usually show favorable prognosis. However, the prognosis becomes poor when the IPMN lesions give rise to invasive carcinoma cells. In addition, recent studies have revealed that BD-IPMN is frequently complicated by common type pancreatic ductal carcinoma. Thus, the prognosis of BD-IPMN depends on the occurrence of these two types of invasive carcinoma. However, little is known about the risk factors for the development of these invasive carcinomas in BD-IPMN. This study aims to identify the factors which predict the development of invasive carcinoma in BD-IPMN.
Methods
Invasive pancreatic carcinoma associating with BD-IPMN was classified as invasive IPMN group (invasive carcinoma derived directly from IPMN lesions) and concomitant group (common type of invasive carcinoma concomitant with BD-IPMN). The relation between the incidence of each type of invasive carcinoma in BD-IPMN and the clinicopathological parameters was retrospectively analyzed.
Results
There were 12 patients with invasive IPMN and 7 patients with concomitant cancer in 159 patients with BD-IPMN. Diameter of dilated branch (P < 0.001) or main pancreatic duct (MPD) (P = 0.001), size of mural nodule (P < 0.001), serum CEA level (P < 0.001) and serum CA19-9 level (P < 0.001) were factors associated significantly with invasive IPMN by univariate analysis. Among these factors, mural nodule with size larger than 6.5 mm [odds ratio 14.86 (95% CI 1.37–60.45); P = 0.02] and serum carcinoembryonic antigen (CEA) level over 5 ng/ml [odds ratio 6.91 (95% CI 1.17–54.13); P = 0.03] were found to be the factors independently associated with invasive IPMN. On the other hand, both univariate and multivariate analyses revealed that elevated carbohydrate antigen 19-9 (CA 19-9) levels were associated with the occurrence of concomitant ductal carcinoma in BD-IPMN [odds ratio 10.31 (95% CI 1.77–81.51); P = 0.01].
Conclusions
Our results suggested that careful imaging study of the entire pancreas in addition to tumor lesions and measurement of serum CEA and CA19-9 would be required to find out the development of the two types of invasive carcinoma in BD-IPMN.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Intraductal papillary mucinous neoplasms (IPMN) represent a particular type of pancreatic cystic neoplasm first described by Ohhashi et al. in Japan in 1982. It was introduced as a “new” type of mucinous neoplasm of the pancreas arising from pancreatic ducts showing prominent duct ectasia and grossly visible mucin excretion from the orifice of the papilla Vater [1]. Since then, such neoplasms have been reported with increasing frequency and in 1996 the World Health Organization (WHO) established criteria to classify IPMN and defined it as intraductal mucin-producing neoplasms showing tall, columnar, mucin-containing epithelium with or without papillary projections [2].
IPMNs are classified into main duct IPMN (MD-IPMN) and branch duct IPMN (BD-IPMN) based on the location of main tumor which can be detected by imaging studies or histological examinations. MD-IPMN is considered to be malignant because about 70% (57–92%) of them are cancer, of which two-thirds are invasive ones [3–11]. Therefore, international consensus guideline recommends surgical resection for all MD-IPMN. On the other hand, only 6–46% of BD-IPMN are reported to be cancer, suggesting low malignant potential compared with MD-IPMN [3–10]. The international consensus guideline suggests that presence of more than one of the following is an indication for surgical resection: (1) cyst-related symptoms, (2) the caliber of the main pancreatic duct diameter larger than 6 mm, (3) cyst size larger than 30 mm, (4) presence of intramural nodules, or cytological demonstration of suspicious/positive malignancy for cyst fluid [12]. Although, these criteria could identify all patients with malignant BD-IPMN, the specificity was low (23%), so that more than 70% of BD-IPMN patients would undergo pancreatic resection in spite of the benign nature of the lesion.
Noninvasive BD-IPMN including carcinoma in situ exhibited favorable prognosis after surgery and 5-year survival rate was reported to be 77–100% [3–11]. In contrast, 5-year survival rate of patients after resection of invasive IPMN ranged widely from 0 to 62% according to reported series [10, 13–19]. Invasive IPMN is generally considered to develop through the adenoma–carcinoma sequence since various grades of cell atypia ranging from hyperplasia to invasive carcinoma can be observed even in the same tumor [20–22]. However, it is unknown whether all IPMN have potential for invasion because invasive IPMN is detected only in 17–43% of all IPMN lesions [4, 10, 13, 15, 23, 24]. In addition, recent studies revealed that complication of BD-IPMN by common type invasive pancreatic cancer is not infrequent [25–27]. Therefore, the prognosis of BD-IPMN would be influenced greatly by the occurrence of these two types of invasive carcinoma. However, little is known concerning the relation between the occurrence of these types of invasive carcinoma and clinicopathological parameters. In the present study, we carried out a retrospective study to find out the factors predicting the progression of invasive carcinoma derived from IPMN and the development of common type pancreatic carcinoma in BD-IPMN patients.
Method
Patients
A total of 159 patients with BD-IPMN were studied among patients attending at the Tohoku University Hospital during the period from December 1995 to September 2007. Medical records were retrospectively reviewed and data including age, sex, clinical presentation, last date of patients visit, and contact information were collected. The BD-IPMN patients were followed-up by imaging studies at least once a year. The diameter of branch duct and main duct, and the size of mural nodule in branch duct were measured by endoscopic ultrasonography (EUS). Follow-up visits and/or imaging studies on the patients who had not come to our hospital longer than a year after their last visit were scheduled by phone.
Definition
The diagnosis of IPMN was made when a pancreatic cyst with size larger than 1 cm was found to communicate with the main pancreatic duct by EUS and one or more additional imaging studies including computed tomography (CT), magnet resonance imaging (MRI), and endoscopic retrograde cholangiopancreatography (ERCP). The type of tumor was classified based on the findings of the EUS and/or ERCP by two endoscopists (A.K. and K.S.): MD-IPMN was defined as a tumor predominantly located in the diffusely or segmentally dilated main pancreatic duct; BD-IPMN was defined as a mucin-producing tumor showing cystic dilatation of the pancreatic duct branches. A mixed type tumor which had spread to both the main pancreatic duct and its branches was categorized as either MD- or BD-IPMN based on the predominant location of the main tumor. The development of invasive carcinoma was diagnosed by imaging studies including CT and EUS, or by histological examination when surgical resection or biopsy from invasive lesion was performed. The type of invasive carcinoma was considered to be invasive carcinoma derived from BD-IPMN (invasive IPMN group) when the invasive solid mass extended continuously from IPMN (Fig. 1), while it was considered to be common type pancreatic carcinoma developed in BD-IPMN (concomitant cancer group) when the invasive solid mass was located separately from the IPMN (Figs. 2, 3).

A representative case of invasive IPMN group. a Computed tomography (CT) showed a papillary protrusion in the dilated branch of the pancreas (arrow). b Endoscopic ultrasonography (EUS) demonstrated a low echoic tumor derived continuously from IPMN lesion (arrowhead) in the head of the pancreas (arrow). c Magnetic resonance cholangiography (MRCP) exhibited cystic dilatation of branch duct with multiple areas of low intensity (arrow). The areas of low intensity in cystic branch represented mural nodules. d Histological examination revealed that papillary tumor (IPMN lesion, arrowhead) was accompanied by infiltrating component of well-differentiated adenocarcinoma (arrow)

A representative case of concomitant cancer group. CT exhibited cystic lesion (arrow in a) and abnormal attenuating area (arrow in b) in the head and tail of pancreas, respectively. EUS showed a dilated branch in the head (arrow in c) and low echoic tumor (arrow in d) in the tail of the pancreas. e Microphotograph of tumor in the pancreatic tail demonstrated poorly differentiated adenocarcinoma and no IPMN was found adjacent to invasive component

Management of IPMN patients in this study
Statistical analysis
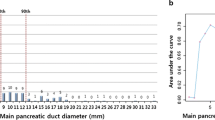
Comparisons of nominal data were conducted by the χ 2 test, and continuous variables were compared by Mann–Whitney U test between subgroups. The optimal cutoff levels for EUS findings (diameter of cystic branch and MPD, and size of nodule) to differentiate noninvasive from invasive tumors were determined by receiver operating characteristic (ROC) curves and identified the point which showed equal sensitivity and specificity on the curve. Sensitivity and specificity were also calculated. Multivariate analysis was performed by multiple logistic regression analysis by using JMP 7.0.1 statistical software (SAS Institute Inc., Cary, NC). Results are presented as mean ± standard error and differences were considered to be significant when the P value was less than 0.05.
Results
Clinical characteristics of IPMN
The biography and outcome of 159 BD-IPMN patients are shown in Table 1 and Fig. 1, respectively. The patients were 96 male and 63 female and their average age was 68.8 ± 10.7 years. The mean observation period for all patients was 1590 ± 1432.3 days. Although surgical resection was recommended to the patients according to the international consensus guideline for IPMN described above they were followed up conservatively if they refused the surgery for various reasons such as advanced age and concomitant diseases. Of 159 patients, 115 were followed without operation and 44 patients underwent surgical resection. Of 44 patients with resection, 28 patients had histologically malignant tumors including 4 invasive IPMN and 3 concomitant ductal carcinoma, while 16 patients turned out to have benign tumors. Of 3 cases with concomitant ductal carcinoma, 2 cases had IPMN and ductal carcinoma synchronously, and 1 case developed ductal carcinoma 2 years after the resection of IPMN. All the IPMN complicated by pancreatic cancer were benign tumors. Among 115 patients followed up, 12 patients developed invasive pancreatic carcinoma, 8 were invasive IPMN and 4 were concomitant pancreatic cancer, and all died of invasive pancreatic carcinoma. As shown in Tables 2 and 3, 8 cases of invasive IPMN were histologically confirmed as cancer by biopsy or cytology. On the other hand, the other 4 invasive IPMN cases were diagnosed as so without histological confirmation because CT and EUS findings were compatible with typical invasive IPMN as shown in Figs. 1 and 2. The IPMN patients after occurrence of invasion showed very poor survival as shown in Tables 2 and 3.
Predictive factors for invasive BD-IPMN and concomitant pancreatic cancer
To find out the predictive factors, we investigated the correlation between clinicopathological parameters and the incidence of invasive IPMN. As shown in Table 4, univariate analysis clarified the significant factors associated with invasive IPMN, these being diameter of dilated branch (P < 0.001) or MPD (P = 0.001), size of mural nodule (P < 0.001), serum CEA level (P < 0.001), and serum CA19-9 level (P < 0.001). By multivariate analysis, mural nodule with size of larger than 6.5 mm [odds ratio 14.86 (95% CI 1.37–60.45); P = 0.02] and serum CEA level higher than 5 ng/ml [odds ratio 6.91 (95% CI 1.17–54.13); P = 0.03] were found to be independently associated with invasive IPMN (Table 5).
We next examined the correlation of clinicopathological factors with the occurrence of concomitant pancreatic cancer in BD-IPMN. Univariate analysis revealed significant association of serum CA19-9 level (P < 0.001) and serum CEA level (P = 0.006) with the event of concomitant pancreatic cancer in BD-IPMN (P < 0.001) (Table 6). Elevated CA19-9 level (>37 IU/ml) still demonstrated the significant relation even if examined by multivariate analysis [odds ratio 10.31 (95% CI 1.77–81.51); P = 0.01]. Consequently, elevated CA19-9 level (>37 IU/ml) was identified as an independent predictive factor for the development of ductal pancreatic carcinoma in BD-IPMN (Table 7).
Discussion
IPMN has been thought to have malignant potential because of its broad histological spectrum, ranging from adenoma to invasive carcinoma in the same tumor [2]. According to several reports, noninvasive IPMN such as adenoma, borderline neoplasms, and carcinoma in situ recur infrequently if they are removed completely, and 5-year survival rate is favorable regardless of the degree of epithelial dysplasia in the tumor [28–31]. Conversely, prognosis becomes poor when the tumor extends to the stage of invasive IPMN [3, 4, 14]. Therefore, it is important to predict invasion rather than histological grade of malignancy for the decision of treatment for IPMN. However, only a few studies have been reported concerning the factors for the prediction of invasive BD-IPMN so far. Sugiyama et al. [9] analyzed 32 cases of BD-IPMN and demonstrated the association of jaundice with invasive BD-IPMN. On the other hand, Schmidt et al. [32] reported from the analysis of 14 invasive tumors out of 103 BD-IPMN that the presence of mural nodule showed tendency to predict invasion (P = 0.06) when univariate analysis was performed, while atypical cytopathology was a sole independent predictive factor for invasion by multivariate analysis. Interestingly, both studies showed that the presence of mural nodule was an independent factor predictive for invasion when main duct and branch duct type IPMN were investigated together. In addition, Ogawa et al. [33] examined CT findings of 61 IPMNs (41 noninvasive and 20 invasive tumors) and reported that mural nodule of larger than 3.7 mm within a cystic branch duct was associated with the incidence of invasive IPMN by univariate analysis. Consistent with these results, we also demonstrated that the size of mural nodule was related to invasiveness of IPMN by univariate analysis and mural nodule of larger than 6.5 mm was an independent predictor of the invasiveness of BD-IPMN by multivariate analysis, suggesting the importance of the size of mural nodule for predicting the development of invasive BD-IPMN. This hypothesis is further supported by the recent report by Tanno et al. [34] on the natural history (median 61 months) of 82 patients with BD-IPMN without mural nodule. They demonstrated that BD-IPMN without mural nodule remained unchanged in size and shape during long-term follow-up, indicating that such IPMN lesions will not progress into invasive IPMN.
In the present study, we also found significant association of MPD and branch duct diameter with the incidence of invasive IPMN by univariate analysis, although the significance disappeared when multivariate analysis was performed. The parameters have been shown to be associated with the malignant nature of BD-IPMN by a number of studies [6, 9, 19], indicating that they reflect, at least in part, biological aggressiveness of IPMN. Although further studies would be required to clarify whether these findings would truly correlate with invasive BD-IPMN, the measurement of the diameter of MPD and/or cystic branch might be helpful to predict malignancy and/or invasion of IPMN patient clinically because these parameters can be easily determined by US or CT while validation of mural nodule in cystic branch requires EUS.
There have been several reports showing synchronous or metachronous occurrence of ductal carcinoma and IPMN. Yamaguchi et al. [25] detected ductal carcinoma of the pancreas in 7 of 76 patients (9%) with IPMN. The IPMNs were all BD-IPMN with an average size of 30 mm and with adenoma showing moderate dysplasia. Tada et al. [26] found development of 5 ductal carcinoma during follow-up of 197 patients with cystic lesions including 80 BD-IPMN for average period of 3.8 years. Uehara et al. [27] found development of ductal carcinoma (8%) in 5 cases of 60 BD-IPMN with nodule less than 10 mm during follow-up for average 87 months. In the current study, we found 7 cases of concomitant ductal carcinoma (4.4%) in 159 cases of BD-IPMN. Of these cases, 4 (3.4%) were detected during follow-up (average 53 months) of 115 BD-IPMN. The frequency of concomitant pancreatic carcinoma in our series of BD-IPMN was similar to those of previous studies, suggesting that BD-IPMN itself may be a risk factor for ductal pancreatic carcinoma and may be a precancerous condition that cannot be demonstrated by imaging studies. However, little is known about the risk factors for development of ductal carcinomas in BD-IPMN other than one report studying the risk factor for concomitant pancreatic cancer in IPMN. Uehara et al. analyzed the occurrence of ductal carcinoma in subgroups of patients with BD-IPMN and revealed that patients older than 70 developed ductal carcinoma significantly more frequently than those under 69, but other factors such as MPD diameter and size of branch duct or mural nodule did not have significant association with development of ductal carcinoma. In the current study, we also found no correlation between the image findings such as the diameter of MPD or branch duct or the size of mural nodule and the occurrence of concomitant ductal carcinoma, suggesting that imaging studies for IPMN lesions cannot give signs for development of ductal carcinoma. Therefore, we have to follow up the patients with BD-IPMN carefully, especially those aged 70 or older, to detect development of pancreatic carcinoma at an early stage.
On the other hand, we clarified that elevated serum CA19-9 was an independent predictive factor for the development of ductal carcinoma in BD-IPMN by multivariate analysis. In addition, serum CEA level showed a tendency toward correlation with the development of ductal carcinoma (P = 0.006) by univariate analysis, indicating the importance to check serum CEA level in addition to CA19-9 for early detection of the concomitant pancreatic cancer in BD-IPMN. In addition, elevated CEA level was identified as the independent factor which showed correlation with invasive BD-IPMN by multivariate analysis. It is reported that the expression of CEA is frequently observed in invasive IPMN (87.5%) and common type pancreatic carcinoma (93.3%) while it is seen infrequently (11.1%) in noninvasive IPMN, indicating that the expression of CEA is characteristics common to both type of invasive pancreatic carcinomas. Altogether, these findings suggested that examination of serum CEA and CA19-9 may be helpful to predict the occurrence of both types of invasive pancreatic carcinoma in BD-IPMN.
In the current study, we clearly revealed the factors that predicts invasion of BD-IPMN. However, previous studies discussed above and our present result indicate that invasive cancer associated with IPMN shows a poor prognosis. Therefore, the best timing of operation for BD-IPMN patients is when the IPMN has progressed to a carcinoma in situ. The international consensus guideline suggests that presence of more than one of the following is indication for resection of BD-IPMN: cyst-related symptom, cysts greater than 30 mm in size, intramural nodules, or dilatation of main pancreatic duct greater than 6 mm [12]. This indication could identify all patients with malignancy; however, its specificity for malignancy was low (23–30%) [35, 36]. Although several researchers have attempted to differentiate malignant from benign IPMN by using several factors, it is impossible to pick up the malignant cases completely. Moreover, it is very difficult to detect only the carcinoma in situ cases at this time. Collectively, further studies would be required to find the best operative timings for BD-IPMN patients by various approaches in addition to detect the predictive factors for invasiveness of BD-IPMN.
In summary, we studied 159 cases of BD-IPMN and revealed that size of mural nodule in branch duct (≥6.5 mm) and elevated serum CEA level (>5 ng/ml) are independent predictive factors for the occurrence of invasion, while elevated CA19-9 level (>37 IU/ml) is a predictor of concomitant pancreatic carcinoma in BD-IPMN, respectively. Based upon our results, careful follow-up by imaging study of the pancreas and measurement of serum CEA and CA19-9 is important to find the development of invasive carcinoma in BD-IPMN.
Abbreviations
- IPMN:
-
Intraductal papillary mucinous neoplasms
- BD-IPMN:
-
Branch duct type intraductal papillary mucinous neoplasms
- CEA:
-
Carcinoembryonic antigen
- CA19-9:
-
Carbohydrate antigen 19-9
- EUS:
-
Endoscopic ultrasonography
- CT:
-
Computed tomography
- MRI:
-
Magnet resonance imaging
- ERCP:
-
Endoscopic retrograde cholangiopancreatography
- MPD:
-
Main pancreatic duct
References
Ohhashi K, Murakami Y, Maruyama M, Takekoshi T, Ohta H, Ohhashi I. Four cases of mucus-secreting pancreatic cancer (in Japanese). Prog Dig Endosc. 1982;20:348–51.
Kloppel G, Solicia E, Longbecker D. Histological classification of tumors of the exocrine pancreas. New York, NY: Springer Verlag; 1996.
Kobari M, Egawa S, Shibuya K, Shimamura H, Sunamura M, Takeda K, et al. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: Differences in clinical characteristics and surgical management. Arch Surg. 1999;134:1131–6.
Terris B, Ponsot P, Paye F, Hammel P, Sauvanet A, Molas G, et al. Intraductal papillary mucinous tumors of the pancreas confined to secondary ducts show less aggressive pathologic features as compared with those involving the main pancreatic duct. Am J Surg Pathol. 2000;24:1372–7.
Doi R, Fujimoto K, Wada M, Imamura M. Surgical management of intraductal papillary mucinous tumor of the pancreas. Surgery. 2002;132:80–5.
Matsumoto T, Aramaki M, Yada K, Hirano S, Himeno Y, Shibata K, et al. Optimal management of the branch duct type intraductal papillary mucinous neoplasms of the pancreas. J Clin Gastroenterol. 2003;36:261–5.
Choi BS, Kim TK, Kim AY, Kim KW, Park SW, Kim PN, et al. Differential diagnosis of benign and malignant intraductal papillary mucinous tumors of the pancreas: MR cholangiopancreatography and MR angiography. Korean J Radiol. 2003;4:157–62.
Kitagawa Y, Unger TA, Taylor S, Kozarek RA, Traverso LW. Mucus is a predictor of better prognosis and survival in patients with intraductal papillary mucinous tumor of the pancreas. J Gastrointest Surg. 2003;7:12–8 (discussion 18–19).
Sugiyama M, Izumisato Y, Abe N, Masaki T, Mori T, Atomi Y. Predictive factors for malignancy in intraductal papillary-mucinous tumours of the pancreas. Br J Surg. 2003;90:1244–9.
Sohn TA, Yeo CJ, Cameron JL, Hruban RH, Fukushima N, Campbell KA, et al. Intraductal papillary mucinous neoplasms of the pancreas: an updated experience. Ann Surg. 2004;239:788–97 (discussion 797–789).
Salvia R, Fernandez-del Castillo C, Bassi C, Thayer SP, Falconi M, Mantovani W, et al. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg. 2004;239:678–85 (discussion 685–677).
Tanaka M, Chari S, Adsay V, et al. International consensus guideline for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006;6:17–32.
Yamao K, Ohashi K, Nakamura T, Suzuki T, Shimizu Y, Nakamura Y, et al. The prognosis of intraductal papillary mucinous tumors of the pancreas. Hepatogastroenterology. 2000;47:1129–34.
Sohn TA, Yeo CJ, Cameron JL, Iacobuzio-Donahue CA, Hruban RH, Lillemoe KD. Intraductal papillary mucinous neoplasms of the pancreas: an increasingly recognized clinicopathologic entity. Ann Surg. 2001;234:313–21 (discussion 321–312).
Raimondo M, Tachibana I, Urrutia R, Burgart LJ, DiMagno EP. Invasive cancer and survival of intraductal papillary mucinous tumors of the pancreas. Am J Gastroenterol. 2002;97:2553–8.
Chari ST, Yadav D, Smyrk TC, DiMagno EP, Miller LJ, Raimondo M, et al. Study of recurrence after surgical resection of intraductal papillary mucinous neoplasm of the pancreas. Gastroenterology. 2002;123:1500–7.
Maire F, Hammel P, Terris B, Paye F, Scoazec JY, Cellier C, et al. Prognosis of malignant intraductal papillary mucinous tumours of the pancreas after surgical resection. Comparison with pancreatic ductal adenocarcinoma. Gut. 2002;51:717–22.
Nakagohri T, Konishi M, Inoue K, Tanizawa Y, Kinoshita T. Invasive carcinoma derived from intraductal papillary mucinous carcinoma of the pancreas. Hepatogastroenterology. 2004;51:1480–3.
Suzuki Y, Atomi Y, Sugiyama M, Isaji S, Inui K, Kimura W, et al. Cystic neoplasm of the pancreas: a japanese multiinstitutional study of intraductal papillary mucinous tumor and mucinous cystic tumor. Pancreas. 2004;28:241–6.
Z’Graggen K, Rivera JA, Compton CC, Pins M, Werner J, Fernandez-del Castillo C, et al. Prevalence of activating K-ras mutations in the evolutionary stages of neoplasia in intraductal papillary mucinous tumors of the pancreas. Ann Surg. 1997;226:491–8 (discussion 498–500).
Longnecker DS. Observations on the etiology and pathogenesis of intraductal papillary-mucinous neoplasms of the pancreas. Hepatogastroenterology. 1998;45:1973–80.
Yamaguchi K, Ogawa Y, Chijiiwa K, Tanaka M. Mucin-hypersecreting tumors of the pancreas: assessing the grade of malignancy preoperatively. Am J Surg. 1996;171:427–31.
Cellier C, Cuillerier E, Palazzo L, Rickaert F, Flejou JF, Napoleon B, et al. Intraductal papillary and mucinous tumors of the pancreas: accuracy of preoperative computed tomography, endoscopic retrograde pancreatography and endoscopic ultrasonography, and long-term outcome in a large surgical series. Gastrointest Endosc. 1998;47:42–9.
Kimura W, Sasahira N, Yoshikawa T, Muto T, Makuuchi M. Duct-ectatic type of mucin producing tumor of the pancreas—new concept of pancreatic neoplasia. Hepatogastroenterology. 1996;43:692–709.
Yamaguchi K, Ohuchida J, Ohtsuka T, Nakano K, Tanaka M. Intraductal papillary-mucinous tumor of the pancreas concomitant with ductal carcinoma of the pancreas. Pancreatology. 2002;2:484–90.
Tada M, Kawabe T, Arizumi M, Togawa O, Matsubara S, Yamamoto N, et al. Pancreatic cancer in patients with pancreatic cystic lesions: a prospective study in 197 patients. Clin Gastroenterol Hepatol. 2006;4:1265–70.
Uehara H, Nakaizumi A, Ishikawa O, Iishi H, Tatsumi K, Takakura R, et al. Development of ductal carcinoma of the pancreas during follow-up of branch duct intraductal papillary mucinous neoplasm of the pancreas. Gut. 2008;57:1561–5.
Sessa F, Solcia E, Capella C, Bonato M, Scarpa A, Zamboni G, et al. Intraductal papillary-mucinous tumours represent a distinct group of pancreatic neoplasms: An investigation of tumour cell differentiation and K-ras, p53 and c-erbB-2 abnormalities in 26 patients. Virchows Arch. 1994;425:357–67.
Yamada M, Kozuka S, Yamao K, Nakazawa S, Naitoh Y, Tsukamoto Y. Mucin-producing tumor of the pancreas. Cancer. 1991;68:159–68.
Nagai E, Ueki T, Chijiiwa K, Tanaka M, Tsuneyoshi M. Intraductal papillary mucinous neoplasms of the pancreas associated with so-called “Mucinous ductal ectasia”. Histochemical and immunohistochemical analysis of 29 cases. Am J Surg Pathol. 1995;19:576–89.
Milchgrub S, Campuzano M, Casillas J, Albores-Saavedra J. Intraductal carcinoma of the pancreas. Cancer. 1992;69:651–6.
Schmidt CM, White PB, Waters JA, Yiannoutsos CT, Cummings OW, Baker M, et al. Intraductal papillary mucinous neoplasms: predictors of malignant and invasive pathology. Ann Surg. 2007;246:644–51 (discussion 651–644).
Ogawa H, Itoh S, Ikeda M, Suzuki K, Naganawa S. Intraductal papillary mucinous neoplasm of the pancreas: assessment of the likelihood of invasiveness with multisection CT. Radiology. 2008;248:876–86.
Tanno S, Nakano Y, Nishikawa T, Nakamura K, Sasajima J, Minoguchi M, et al. Natural history of branch duct intraductal papillary-mucinous neoplasms of the pancreas without mural nodules: long-term follow-up results. Gut. 2008;57:339–43.
Tang RS, Weinberg B, Dawson DW, et al. Evaluation of the guideline for management of pancreatic branch-duct intraductal papillary mucinous neoplasm. Clin Gastroenterol Hepatol. 2008;6:815–9.
Pelaez-Luna M, Chari ST, Smyrk TC, et al. Do consensus indicaions for resection in branch duct intraductal papillary mucinous neoplasm. Am J Gastroenterol. 2007;102:1759–64.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kanno, A., Satoh, K., Hirota, M. et al. Prediction of invasive carcinoma in branch type intraductal papillary mucinous neoplasms of the pancreas. J Gastroenterol 45, 952–959 (2010). https://doi.org/10.1007/s00535-010-0238-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-010-0238-0