
Abstract
Purpose
We retrospectively assessed post-EST complications and examined whether combination therapy comprising endoscopic biliary drainage (EBD) plus endoscopic sphincterotomy (EST) as the initial treatment is safe in patients with acute cholangitis due to choledocholithiasis.
Methods
Among the 363 consecutive patients with acute cholangitis due to choledocholithiasis who were treated in our hospital between December 1992 and December 2006, the subjects comprised 127 patients with moderate acute cholangitis for whom EBD and EST were carried out. Factors influencing risk factors for post-EST pancreatitis, hemorrhage and hospitalization were determined by multivariate analysis.
Results
Multivariate analysis revealed that only precut sphincterotomy (PST) was a significant risk factor for post-EST pancreatitis, and the incidence of pancreatitis in patients who underwent PST was significantly higher than that in those who did not (P = 0.041). Only age was a significant risk factor for post-EST hemorrhage, and younger patients were likely to experience hemorrhage after EST (P = 0.021). Total bilirubin and the timing of EST were significant factors associated with hospitalization. Hospitalization in patients who underwent EBD plus EST as the initial treatment (emergency EST) was significantly shorter than that in those who palliatively underwent EST after EBD (elective EST; 11.8 vs. 16.2 days, P = 0.001).
Conclusions
Combination therapy comprising EBD plus EST as the initial treatment for patients with moderate acute cholangitis due to choledocholithiasis was safe and did not prolong the period of hospitalization.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
It is widely recognized that endoscopic biliary drainage (EBD) [1–3] in patients with acute cholangitis is important as the initial treatment. EBD and treatment of the papilla of Vater, which includes endoscopic sphincterotomy (EST) [4] and endoscopic papillary balloon dilation (EPBD) [5], are required for patients with acute cholangitis associated with choledocholithiasis, but these modalities are not yet aggressively applied as the initial treatment since cholangitis has been regarded as a risk factor for post-EST hemorrhage [6]. According to the Tokyo Guidelines for the management of acute cholangitis and cholecystitis, as reported in 2007 [7, 8], biliary drainage should be conducted in patients with moderate or severe cholangitis, and after improvement in the cholangitis is obtained, then palliative treatment for the etiology (i.e. endoscopic treatment, percutaneous treatment or surgery) should be conducted. However, if EBD and EST were to be performed simultaneously as the initial treatment for patients with acute cholangitis, hospitalization could be expected to be shortened and the quality of life of patients would thus improve more rapidly. In this study, we retrospectively assessed whether or not emergency EST is safe and beneficial for patients with moderate acute cholangitis due to choledocholithiasis.
Subjects and methods
From December 1992 to December 2006, a cohort of 363 consecutive patients with acute cholangitis due to choledocholithiasis was examined in the Department of Gastroenterology at Fukuoka University Chikushi Hospital. Among them, 18 were treated by EPBD and 88 were treated by percutaneous transhepatic biliary drainage (PTBD). The remaining 257 patients (122, mild cholangitis; 127, moderate cholangitis; 8, severe cholangitis) were treated by EBD and EST. The subjects of this study comprised the 127 patients with moderate cholangitis; 2 patients who were receiving antiplatelet or anticoagulant therapy were included among those patients. Between December 1992 and December 2003, EBD was conducted as the initial treatment followed by EST approximately 1 week later (elective EST). However, since January 2004, EST has been conducted first, as the initial treatment (emergency EST), followed by EBD. In both the emergency EST and the elective EST groups, the choledocholith was removed approximately 1 week after the EST using a basket catheter and/or a balloon catheter. When the diameter of the choledocholith was 1 cm or more, it was broken into small pieces by a mechanical lithotripter before removal. In principle, the existence of stone remnants was not clarified on the other days after removal by ERCP, and the outcome with regard to improvement of acute cholangitis was that there were no cases of jaundice [2]. EST was carried out by a pull-type sphincterotome [9]. All patients had started receiving systemic administration of protease inhibitors and antibiotics before the procedure [10]. Diazepam was administered for a sedative effect in some patients. There were no patients in a restless state or in shock, but EBD without EST was conducted as the initial treatment in two patients (receiving antiplatelet or anticoagulant therapy) who had a hemorrhagic tendency (elective EST). EBD included endoscopic nasobiliary drainage (ENBD) or endoscopic retrograde biliary drainage (ERBD) [1–3]. For ENBD, a 7F pigtail type nasal biliary drainage tube (PBD-21Z; Olympus Medical Systems Co., Tokyo, Japan) was used. For ERBD, a 7F straight type biliary stent (RX Biliary Stent; Boston Scientific Japan Co., Tokyo, Japan) was used. The high-frequency generators used were PSD-30 (Olympus Medical Systems Co., Tokyo, Japan) or ICC 200 EA INA (AMCO Inc., Tokyo, Japan). The diagnostic criteria for acute cholangitis conformed to the Tokyo Guidelines [11], i.e. Charcot’s triad (fever and/or chills, jaundice, abdominal pain) or two or more items in clinical context (history of biliary disease, fever and/or chills, jaundice, abdominal pain) plus both items in laboratory data (evidence of inflammatory response, abdominal liver function tests) and biliary dilatation or evidence of etiology (stricture, stone, stent, etc.). Severity assessment of acute cholangitis was defined as follows: mild acute cholangitis, corresponding to acute cholangitis which responds to general supportive care and antibiotics; moderate acute cholangitis, corresponding to acute cholangitis that does not respond to general supportive care and antibiotics, and is not accompanied by organ dysfunction; severe acute cholangitis, corresponding to acute cholangitis that is associated with the onset of dysfunction in at least any one of the following organs/system; cardiovascular system, nervous system, respiratory system, kidney, liver, hematological system.
Factors analyzed
-
1.
In both the emergency EST and the elective EST groups, the following factors were analyzed: clinical background [age, gender, the presence/absence of pancreatitis due to choledocholithiasis, diameter (mm) of the common bile duct, diameter (mm) of the choledocholith, number of choledocholiths, WBC (/μl), CRP (mg/dl), total bilirubin (T. Bil; mg/dl), AST (IU/l), ALT (IU/l), ALP (IU/l), r-GTP (IU/l) and platelet count (PLT; ×104/μl) at the time of EST], the presence/absence of receiving antiplatelet or anticoagulant therapy, the presence/absence of post-EST pancreatitis and post-EST hemorrhage, sessions of ERCP, and hospitalization.
-
2.
Factors which were considered to be related to post-EST pancreatitis and hemorrhage included age, gender, presence/absence of pancreatitis due to choledocholithiasis, diameter (mm) of the common bile duct, diameter (mm) of the choledocholith, number of choledocholiths, WBC (/μl), CRP (mg/dl), T. Bil (mg/dl), AST (IU/l), ALT (IU/l), ALP (IU/l), r-GTP (IU/l), and PLT (×104/μl) at the time of EST, the presence/absence of receiving antiplatelet or anticoagulant therapy, the presence/absence of precut sphincterotomy (PST) [6, 12], and the timing of EST (emergency EST versus elective EST).
-
3.
Factors which were considered to be related to hospitalization included age, gender, the presence/absence of pancreatitis due to choledocholithiasis, diameter (mm) of the common bile duct, diameter (mm) of the choledocholith, number of choledocholiths, and WBC (/μl), CRP (mg/dl), T. Bil (mg/dl), AST (IU/l), ALT (IU/l), ALP (IU/l), r-GTP (IU/l), and PLT (×104/μl) on admission, the presence/absence of receiving antiplatelet or anticoagulant therapy, the timing of EST (emergency EST versus elective EST), the presence/absence of PST, the presence/absence of post-EST pancreatitis, and the presence/absence of post-EST hemorrhage.
Post-EST pancreatitis was defined as abdominal pain persisting for at least 24 h after the ERCP and associated with an elevation of serum amylase level to at least three times the upper limit for a normal level at 18 h after EST [12]. Post-EST hemorrhage was defined as the state corresponding to any of the following conditions: (1) appearance of tarry stool; (2) decrease in Hb by 2 mg/dl or more; (3) necessity of blood transfusion; and (4) hemostatic treatments including heat probe [13].
Statistical analysis
In both the emergency EST and the elective EST groups, the χ 2 and Fisher’s exact tests were used for comparison of categorical data. All continuous data values were expressed as mean ± SD. Differences in the mean values were examined by Student’s t test.
The relationship between post-EST pancreatitis or post-EST hemorrhage and age, gender, pancreatitis due to choledocholithiasis, diameter of the common bile duct, diameter of the choledocholith, number of choledocholiths, WBC, CRP, T. Bil, AST, ALT, ALP, r-GTP, PLT, receiving antiplatelet or anticoagulant therapy, PST, and the timing of EST were investigated by univariate analysis using a logistic regression model. Multivariate analysis using a logistic regression model was conducted on the factors that may have affected post-EST pancreatitis (P < 0.25) or post-EST hemorrhage (P < 0.25) according to the findings from univariate analysis using a logistic regression model. A forward selection method was used for variable selection and analyses were conducted by using slentry (P = 0.20) and slstay (P = 0.25).
The relationship between hospitalization and age, gender, pancreatitis due to choledocholithiasis, diameter of the common bile duct, diameter of the choledocholith, number of choledocholiths, WBC, CRP, T. Bil, AST, ALT, ALP, γ-GTP, receiving antiplatelet or anticoagulant therapy, the timing of EST, PST, post-EST hemorrhage, and post-EST pancreatitis were investigated by simple regression analysis. Multivariate analysis using multiple regression analysis was conducted on the factors that may have affected hospitalization (P < 0.25) according to the findings from univariate analysis using simple regression analysis. Statistical significance was defined as a P value <0.05. The software used for the statistical analysis was SPSS 16.0J for Windows.
Results
-
1.
Comparison of clinical backgrounds between the emergency and elective EST groups (Table 1) revealed no significant differences in age, gender, presence/absence of pancreatitis due to choledocholithiasis, diameter of the common bile duct, diameter of the choledocholith, number of choledocholiths, ALP, r-GTP, PLT, presence/absence of receiving antiplatelet or anticoagulant therapy, presence/absence of post-EST pancreatitis, or presence/absence of post-EST hemorrhage. Blood biochemical examination revealed WBC, CRP, T. Bil, AST, ALT and r-GTP to be significantly higher in the emergency group than in the elective EST group, and PLT to be significantly lower in the emergency group than in the elective EST group. Sessions of ERCP were significantly more in the emergency EST group than in elective EST group. Hospitalization was significantly shorter in the emergency EST group than in the elective EST group. None of the three patients with post-EST pancreatitis was in a severe condition, and none of the 11 patients with post-EST hemorrhage required blood transfusion.
Table 1 Comparison of clinical background between an emergency endoscopic sphincterotomy group and elective endoscopic sphincterotomy group, expressed as mean ± SD -
2.
On univariate and multivariate analyses using logistic models of factors related to post-EST pancreatitis, only the presence/absence of PST was a significant factor (P = 0.046). Patients who underwent precut sphincterotomy were more likely to have had post-EST pancreatitis (Tables 2, 3).
Table 2 Univariate analysis for predictive factors associated with post-EST pancreatitis, expressed as mean ± SD Table 3 Multivariate analysis for predictive factors associated with post-EST pancreatitis -
3.
On univariate and multivariate analyses using logistic models of factors related to post-EST hemorrhage, only age was a significant factor (P = 0.023). Younger patients were more likely to have had post-EST hemorrhage (Tables 4, 5).
Table 4 Univariate analysis for predictive factors associated with post-EST hemorrhage, expressed as mean ± SD Table 5 Multivariate analysis for predictive factors associated with post-EST hemorrhage
There were no post-EST complications other than pancreatitis and hemorrhage; cholangitis, cholecystitis and duodenal perforation, etc., did not occur.
-
4.
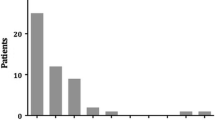
Simple regression analysis of factors related to hospitalization revealed significant differences in the diameter of the choledocholith, T. Bil, and the timing of EST, whereas T. Bil (P < 0.001), and the timing of EST (P = 0.010) were significant independent factors according to multiple regression analysis (Tables 6, 7, 8). In other words, hospitalization was shortened in the emergency EST group and prolonged in patients with elevated T. Bil levels. When the level of T. Bil was 3, 5 and 10 mg/dl, hospitalization was 12.5, 14.1 and 18.1 days, respectively (Fig. 1).
Table 6 Comparison of blood biochemical examination between an emergency endoscopic sphincterotomy group and an elective endoscopic sphincterotomy group on admission, expressed as mean ± SD Table 7 Univariate analysis for predictive factors associated with hospitalization, expressed as mean ± SD Table 8 Multiple regression analysis for factors associated with hospitalization Fig. 1 
Hospitalization and T. Bil. Hospitalization was correlated with total bilirubin (P < 0.001)

Discussion
Sugiyama et al. [1] and Hui et al. [2] have described the addition of EST to EBD as being unnecessary for treatment of acute cholangitis due to choledocholithiasis, for the following reasons: (1) There is no difference in efficacy between drainage with versus drainage without EST; and (2) the addition of EST to EBD leads to complications such as hemorrhage. Hui et al. [2] reported that there was no significant difference between the EBD alone group and the EBD plus EST group regarding the period from admission to improvement of jaundice. The Tokyo Guidelines also recommend elective EST in patients with moderate acute cholangitis, but post-EST complications have not yet been adequately assessed according to the timing of EST. In the present study, the factors affecting post-EST pancreatitis and post-EST hemorrhage by multivariate analysis were PST and age in patients with moderate acute cholangitis due to choledocholithiasis, respectively. At the time of EST, the emergency EST patients were in a worse general condition than the elective EST patients. However, it was shown that emergency EST was safe and did not increase the risk of either post-EST pancreatitis or post-EST hemorrhage. Freeman et al. [6] reported that post-EST complications included pancreatitis (0.4%), hemorrhage (0.5%), cholangitis (0.1%), and duodenal perforation (0.2%). However, no post-EST complications, such as cholangitis, cholecystitis, or duodenal perforation were noted in the present study. There was a significant difference between the emergency EST group and the elective EST group regarding blood biochemical examination on admission. However, emergency EST did not prolong the period of hospitalization.
Conditions assumed to cause post-EST pancreatitis include spasm of Oddi’s muscle due to stimulation by cannulation into the orifice of the papilla of Vater, elevated intraductal pancreatic pressure due to edema of the papilla of Vater, which is caused by excessively turning on the electricity at the time of EST, and trypsin activation, which results from stimulation of pancreatic acinar cells due to turning on the electricity at the time of EST [11]. Freeman et al. [6] have also noted that the incidence of post-EST pancreatitis is significantly higher in those patients for whom bile duct cannulation was time-consuming. PST, which was a significant risk factor for post-EST pancreatitis in the present study, is a technique for incision of the orifice of the papilla of Vater as an adjunct to bile duct cannulation in cases where selective cannulation of the common bile duct has failed. PST has been believed to readily cause pancreatitis, since it results in edema of the orifice of the papilla of Vater [12]. All the subjects of the present study had started to receive drip infusions of protease inhibitors prior to EST for the prevention of pancreatitis. As described above, insertion of a plastic stent into the main pancreatic duct should also be conducted in addition to the administration of protease inhibitors in patients receiving PST, since some reports have also shown that hospitalization is prolonged in those patients with post-EST pancreatitis and, furthermore, that the stenting of pancreatic ducts is useful for preventing post-EST pancreatitis [14–16].
In the present study, T. Bil was also found to be a significant factor that influenced hospitalization, but this was not surprising, since it took several days for jaundice to subside if T. Bil was elevated. There were no reports with respect to a correlation between the period of hospitalization and the interval between emergency EBD and elective EST. In the elective EST group, EBD was conducted as the initial treatment followed by EST approximately one week later, in order to perform EST safely, and the choledocholith was removed approximately one week after the EST. At the time of EST, the emergency EST patients were in a worse general condition than the elective EST patients. However, emergency EST did not increase the risk of post-EST complications. Accordingly, elective EST will be conducted less than one week after EBD in the future. Moreover, the choledocholith will be removed at the time of elective EST.
A large series previously indicated that the overall incidence of post-EST hemorrhage ranges from 2.5 to 5% [12]. The incidence in the present study was 8.8%. The reason for this high incidence was thought to be that all the subjects suffered from moderate acute cholangitis, rather than mild acute cholangitis. Freeman et al. [6] have reported that the risk factors for post-EST hemorrhage on multivariate analysis are the presence of coagulopathy, anticoagulant therapy, cholangitis before the procedure, an endoscopist’s case volume of one or less cases per week, and bleeding during the procedure. In general, the rate of patients with a hemorrhagic tendency is higher among older patients than among younger patients. Accordingly, a higher age is a risk factor for post-EST hemorrhage [17]. However, in the present study EBD without EST was conducted as the initial treatment in two patients with a hemorrhagic tendency, and then elective EST was carried out after amelioration of the hemorrhagic tendency. Consequently, the only risk factor for post-EST hemorrhage was a young age. When the patients were divided into a younger group (45 years old or younger) and an older group (46 years old or older), the accuracy rate of post-EST hemorrhage as predicted by age was 92%. The reason for this may be that arterial sclerosis is less-progressed in young patients than in old patients, and so the blood vessels of the papilla of Vater are abundant in young patients. Although post-EST hemorrhage was not a significant factor that influenced hospitalization, it may be safer if younger patients undergo EBD first, with EST being conducted after the cholangitis has ameliorated.
An emergency EST did not prolong hospitalization, but the most important treatment for acute cholangitis was biliary drainage. In patients who are in a restless state, in shock, or in a poor general condition, including those with receiving antiplatelet or anticoagulant therapy, biliary drainage without EST should be performed within a short time. The incidences of post-EST pancreatitis and hemorrhage are largely dependent upon the skill of the endoscopist, in addition to the factors related to the host. Endoscopists must aim to improve their technique and fully utilize their abilities under an adequate guidance system.
Conclusion
The present study was conducted retrospectively. Whether or not emergency EST in cases of moderate acute cholangitis due to choledocholithiasis will improve the quality of life of patients without increasing the incidence of complications needs to be prospectively assessed in a future study.
References
Sugiyama M, Atomi Y. Treatment of acute cholangitis due to choledocholithiasis in elderly and younger patients. Arch Surg. 1997;132:1129–33.
Hui CK, Lai KC, Yuen MF, Matthew NG, Chan CK, Wayne HU, et al. Does the addition of endoscopic sphincterotomy to stent insertion improve drainage of the bile duct in acute suppurative cholangitis? Gastrointest Endosc. 2003;58:500–4.
Sharma BC, Kumar R, Agarwal N, Sarin SK. Endoscopic biliary drainage by nasobiliary drain or by stent placement in patients with acute cholangitis. Endoscopy. 2005;37:439–43.
Kawai K, Akasaka Y, Murakami K, Tada M, Kohli Y, Nakajima M. Endoscopic sphincterotomy of the ampulla of Vater. Gastrointest Endosc. 1974;20:148–51.
Komatsu Y, Kawabe T, Toda N, Ohashi M, Isayama M, Tateishi K, et al. Endoscopic papillary balloon dilation for the management of common bile duct stones: experience of 226 cases. Endoscopy. 1998;30:12–7.
Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;335:909–18.
Takada T, Kawarada Y, Nimura Y, Yoshida M, Mayumi T, Sekimoto M, et al. Background: Tokyo Guidelines for the management of acute cholangitis and cholecystitis. J Hepatobiliary Pancreas Surg. 2007;14:1–10.
Miura F, Takada T, Kawarada Y, Nimura Y, Wada K, Hirota M, et al. Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines. J Hepatobiliary Pancreas Surg. 2007;14:27–34.
Ikeda S, Tanaka M, Itoh H, Tamura R. A newly devised cutting probe for endoscopic sphincterotomy of the ampulla of Vater. Endoscopy. 1977;9:238–41.
Ueki T, Otani K, Kawamoto K, Shimizu A, Fujimura N, Sakaguchi S, et al. Comparison between ulinastatin and gabexate mesylate for the prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis: a prospective, randomized trial. J Gastroenterol. 2007;42:161–7.
Wada K, Takada T, Kawarada Y, Nimura Y, Miura F, Yoshida M, et al. Diagnostic criteria and severity assessment of acute cholangitis: Tokyo Guidelines. J Hepatobiliary Pancreas Surg. 2007;14:52–8.
Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RCG, Meyers WC, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991;37:383–93.
Sugiyama M, Atomi Y. The benefits of endoscopic nasobiliary drainage without sphincterotomy for acute cholangitis. Am J Gastroenterol. 1998;93:2065–8.
Smithline A, Silverman W, Rogers D, Nisi R, Wiersema M, Jamidar P, et al. Effect of prophylactic main pancreatic duct stenting on the incidence of biliary endoscopic sphincterotomy-induced pancreatitis in high-risk patients. Gastrointest Endosc. 1993;39:652–7.
Fazel A, Quadri A, Catalano MF, Meyerson SM, Geenen JE. Does a pancreatic duct stent prevent post-ERCP pancreatitis? A prospective randomized study. Gastrointest Endosc. 2003;57:291–4.
Sofuni A, Maguchi H, Itoi T, Katanuma A, Hisai H, Niido T, et al. Prophylaxis of post-endoscopic retrograde cholangiopancreatography pancreatitis by an endoscopic pancreatic spontaneous dislodgement stent. Clin Gastroenterol Hepatol. 2007;5:1339–46.
Deans GT, Sedman P, Martin DF, Royston CMS, Leow CK, Thomas WES, et al. Are complications of endoscopic sphincterotomy age related? GUT. 1997;41:545–8.
Acknowledgments
The English used in this manuscript was revised by Miss K. Miller (Royal English Language Centre, Fukuoka, Japan).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ueki, T., Otani, K., Fujimura, N. et al. Comparison between emergency and elective endoscopic sphincterotomy in patients with acute cholangitis due to choledocholithiasis: is emergency endoscopic sphincterotomy safe?. J Gastroenterol 44, 1080–1088 (2009). https://doi.org/10.1007/s00535-009-0100-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-009-0100-4