
Abstract
Background
When distal pancreatectomy is carried out for left-sided pancreatic cancer, splenectomy is usually performed not only for margin-negative resection but also for effective clearance of the splenic hilar lymph nodes (LNs). However, the incidence of splenic hilar LN metastasis in these patients has not been definitively determined.
Methods
From April 2010 to June 2011, in a pilot study, we analyzed the medical records of twelve patients who had undergone radical antegrade modular pancreatosplenectomy. Potential remnant soft tissue around the splenic hilum, which would be left following an extended Warshaw’s procedure, was dissected and sent to a pathologist. Three Japanese medical centers conducted a retrospective survey of splenic hilar lymph node metastasis in left-sided pancreatic cancer to support our study.
Results
In the pilot study, all twelve patients had adenocarcinoma with a median tumor size of 2 cm. Six patients had LN metastasis and a median number of 4 splenic hilar LNs were evaluated; however, no splenic hilar LN metastasis was noted. In the Japanese multicenter survey (n = 85), only four patients had splenic LN metastasis. Small (<3 cm) and proximal (neck/body) left-sided pancreatic cancer might not be associated with splenic hilar LN metastasis (P < 0.05).
Conclusions
In well-selected left-sided pancreatic cancer, the incidence of splenic hilar LN metastasis is low enough that splenectomy-omitting radical distal pancreatectomy would be feasible. The rationale for routine splenectomy should be re-evaluated, and the oncologic effects of the preserved spleen need to be investigated further.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It has been established that splenectomy must be included not only for margin-negative resection but also for effective regional lymph node (LN) clearance when performing a distal pancreatectomy for pancreatic cancer in the body or tail of the pancreas. For example, if the pancreatic cancer is near the splenic hilum, or directly invading the spleen, a splenectomy should be performed because it can facilitate a margin-negative en-bloc resection. Even for a tumor that has developed in the body of the pancreas away from the splenic hilum, a splenectomy has been routinely recommended under the rationale of effective regional LN clearance, especially that of splenic hilar LNs. However, we would like to ask the following questions about this traditional concept. Is the actual incidence of splenic hilar LN metastasis so frequent that we should perform routine splenectomy? If this is not so, and a sound surgical technique for splenectomy-omitting radical distal pancreatectomy does exist, should splenectomy always be included in radical surgery for left-sided pancreatic cancer?
As Crippa et al. [1] referred to distal pancreatectomy as an “extended” distal pancreatectomy when the pancreas was divided at the level of the superior mesenteric vein (SMV)–splenic vein (SV)–portal vein (PV) confluence, we may also designate Warshaw’s procedure [2] (a distal pancreatectomy with segmental resection of both the splenic artery and vein) as an “extended” Warshaw’s procedure [3, 4], when the pancreas is divided at the level of the SMV–SV–PV confluence with the splenic artery and vein securely controlled at the origin of the vessels. If we add a regional lymph node dissection around the common hepatic artery, celiac axis, and superior mesenteric artery to this technique, as is done in radical antegrade modular pancreatosplenectomy (RAMPS), this “modified” extended Warshaw’s procedure is exactly same as that of RAMPS for treating pancreatic cancer, except that splenectomy is omitted. We would like to name this procedure (extended Warshaw’s procedure with regional lymph node dissection) “RAMP (radical antegrade modular pancreatectomy)” because it does not include splenectomy in the concept of RAMPS (RAMPS − splenectomy = RAMP). We hypothesized this splenectomy-omitting radical distal pancreatectomy, RAMP, would be feasible if the incidence of splenic hilar LNs metastasis were not so high, and it might also be applicable to well-selected left-sided pancreatic cancers.
In this study, we present our preliminary data suggesting the potential feasibility of radical oncologic surgery without splenectomy in patients with left-sided pancreatic cancer, derived from our analysis of surgical specimens resected after RAMPS. In addition, we also provide data from three Japanese centers supporting our hypothesis and discuss the feasibility of splenectomy-omitting radical distal pancreatectomy in well-selected left-sided pancreatic cancer.
Patients and methods
Single-center [Severance Hospital (Yonsei University Health System; YUHS)] pilot study
Patients
We prospectively collected the medical records of patients who underwent RAMPS for left-sided pancreatic cancer between April 2010 and June 2011 and analyzed their clinicopathologic characteristics, with special reference to splenic hilar LN metastasis. Patients with pancreatic cancers directly invading the splenic hilum or spleen were excluded from this study.
Surgical specimens
The surgical specimens were trimmed before they were sent for pathologic examination. Potential remnant soft tissue around the splenic hilum, which would be left following the extended Warshaw’s procedure, was dissected and sent for pathologic examination to confirm LN metastasis of splenic hilar LNs in distal pancreatic cancer. The specimen was re-arranged in such a way as if the spleen was left intact to evaluate the feasibility of the procedure without splenectomy (Figs. 1, 2). Our Institutional Review Board Committee approved this study protocol.

Case simulation—pilot study. Specimen retrieved by anterior radical antegrade modular pancreatosplenectomy (RAMPS) (dashed line indicates tumor location) and potential soft tissue left after the modified extended Warshaw procedure (solid line) (a). Soft tissue dissection around the splenic hilum (b, c). Dissected soft tissue was sent for pathologic examination (d)

Rearrangement based on theoretical surgical scheme in left-sided pancreatic cancer (RAMP)—pilot study. The spleen may be saved by performing the modified extended Warshaw’s procedure (RAMP) for left-sided pancreatic cancer. On pathologic examination, potential soft tissue left after RAMP had no lymph node metastasis. The resection margin of the pancreas and tangential margin were all negative in this case
Japanese multicenter survey of splenic hilar lymph node metastasis in left-sided pancreatic cancer
A standardized case report form was requested from three Japanese medical institutions (Kansai Medical University, Nara Medical University, and Nippon Medical School) which agreeed with our present clinical hypothesis. Each center was known to be performing more than 30 pancreatoduodenectomies annually for pancreatic pathology. The clinicopathologic data of the patients who had undergone radical distal pancreatosplenectomy for left-sided pancreatic cancer during the 5-year period from January 2005 to December 2010 were retrospectively investigated. The data for the enrolled patients had to fulfill the following criteria: ductal adenocarcinoma was proven by pathologic examination and mapping of LNs was done before the specimen was sent to the pathologist. By summarizing our preliminary results and the data from the three Japanese centers, we intended to investigate the actual incidence of splenic hilar LN metastasis and to analyze the risk of splenic hilar LN metastasis in left-sided pancreatic cancers.
Statistics
Categorical variables are expressed as frequencies with percentages, and continuous variables as means ± standard deviation (or medians with ranges). The χ2 test (Fisher’s exact test if needed) and Student’s t test were applied for statistical comparisons. P values of less than 0.05 were regarded as indicating significant differences.
Results
Feasibility of RAMP in well-selected left-sided pancreatic body cancer—single-center (YUHS) study
General characteristics of patients
The pathologic examination of resected surgical specimens showed that all twelve patients had pancreatic ductal adenocarcinoma. Six patients were male and six were female. The median age of the patients was 65 years (range, 35–75 years). Ten patients had pancreatic cancer in the body of the pancreas, and two had pancreatic cancer in the tail. Four patients underwent surgery following neoadjuvant chemoradiation therapy. All patients underwent radical surgery based on the concept of anterior RAMPS [5].
Tumor characteristics and frequency of splenic hilar (No. 10) lymph node metastasis
The median tumor size was 2 cm (range, 0.8–4 cm), and the median number of retrieved LNs was 17 (range, 5–29). Four patients underwent RAMPS following neoadjuvant chemoradiation therapy; three of these four patients presented T1 stage cancer and one was shown to have no residual cancer. Six patients were found to have LN metastasis. Soft tissue around the splenic hilum, which would be potentially left intact after the extended Warshaw’s procedure, was evaluated for No. 10 LN metastasis. A median of 4 (range, 1–6) splenic hilar LNs were microscopically examined, and no splenic hilar LN metastasis (0 %) was observed (Table 1).
Feasibility of RAMP in well-selected left-sided pancreatic cancer—Japanese multicenter survey study
General characteristics of patients
Clinicopathologic data of resected left-sided pancreatic cancer were retrospectively collected from a total of 85 patients in the multicenter survey study. Forty-five patients (52.9 %) were male and forty (47.1 %) were female, with a mean age of 67.4 ± 9.0 years. Table 2 lists the pathologic characteristics of the resected left-sided pancreatic cancers. The mean tumor size was 3.1 ± 1.3 cm, and the mean number of retrieved LNs was 20.2 ± 11.7. Thirty-seven patients (43.5 %) were found to have LN metastasis (pN1). A mean of 3.3 ± 5.6 splenic hilar LNs were microscopically evaluated, and 4 patients (4.7 %) were reported to have splenic hilar LN metastasis.
Relationship of splenic lymph node metastasis with clinicopathologic characteristics
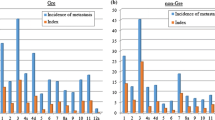
All tumors in the patients with splenic hilar lymph node metastasis were located in the tail of the pancreas near the splenic hilum (range, 0–1.5 cm from the splenic hilum), and most of them required combined adjacent organ resection such as that of the colon, left adrenal gland, and stomach, for margin-negative surgery (Table 3). On analysis of splenic hilar LN metastasis according to tumor location pancreatic cancer near the tail of the pancreas showed a significantly higher incidence of splenic LN metastasis comparing with that in proximal left-sided pancreatic cancer (neck or body, 0 vs. 10.5 %, χ2, Fisher’s exact test, P = 0.029). Patients who only underwent distal pancreatosplenectomy for margin-negative resection (DPS only) showed a relatively lower incidence of splenic hilar LN metastasis in comparison to those who had combined adjacent organ resection with DPS (1.7 vs. 11.1 %, P = 0.092,). Tumor size less than 3 cm was significantly related to a low incidence of splenic hilar LN metastasis (0 vs.10.8 %, P = 0.032, Table 4).
In addition, it was noted that none of the patients with proximal left-sided pancreatic cancers (neck and body) was found to have splenic hilar LN metastasis, even in patients requiring combined adjacent organ resections (12 patients).
Discussion
RAMPS is thought to be a reasonable approach for margin-negative resection and systematic LN dissection in treating left-sided pancreatic cancer [6, 7]. Unlike pancreatic head cancer, there have been no precise studies concerning LN involvement in carcinoma of the body and tail of the pancreas. However, Fujita et al. [8] recently reported that absence of LN metastasis was noted in the No. 10 node group in pancreatic cancers in the body and even those in the tail (absent in 37 No. 10 nodes in body cancers, 31 No. 10 nodes in body-tail cancers, and 40 No. 10 nodes in tail cancers). Interestingly, Nakao et al. [9] also observed a low incidence of LN metastasis in the hilum of the spleen (one out of 30 patients, 3.3 %). In our pilot study metastasis in the No. 10 LN was not found in any instances. In addition, data from the present Japanese multicenter survey showed a low incidence of No. 10 LN metastasis in resected left-sided pancreatic cancers (Tables 2, 3). Regardless of whether there had been combined resection of an adjacent organ, the proximal part of left-sided (neck or body) pancreatic cancer was not accompanied by No. 10 LN metastasis (Table 4). Therefore, we would like to say that the rationale of routine splenectomy for clearing No. 10 LNs in the treatment of left-sided pancreatic cancer may have been based on an overestimation of the incidence of metastasis in No. 10 LNs.
There are several historical lessons about organ-preservation in pancreatic cancer surgery. In the past, we know that many surgeons preferred the conventional pancreatoduodenectomy (PD) in treating pancreatic head cancer because of a fear of incomplete LN dissection around the prepyloric area. However, the oncologic outcome was shown to be similar in both PD and pylorus-preserving pancreaticoduodenectomy (PPPD) [10, 11], and the incidence of peripyloric LN metastasis in pancreatic head cancer was reported to be less than 6 % [12, 13]. Now, PPPD (so-called hemigastrectomy-omitting PD) has been accepted as a safe oncologic modality [14, 15]. In addition, powerful randomized control studies have shown that pancreatic cancer in the head of the pancreas treated with extended LN dissection did not show improved survival outcomes compared with standard procedures [16–18]. Applying these lessons for treating left-sided pancreatic cancer, a mandatory splenectomy for potential LN clearance around the splenic hilum may also not be beneficial, and our present observations and literature review suggestthat splenectomy-omitting radical distal pancreatectomy could be performed with an overall risk of splenic hilar LN metastasis of less than 5 %. However, according to the results of our multicenter survey, if we were to select the proper patients, the actual risk of splenic LN metastasis after RAMP would be nearly null (Table 4).
A significant increase in postoperative morbidity [19] and inferior survival outcomes following splenectomy have been demonstrated in gastric [20] and colon cancers [21]. In 1999, Schwarz et al. [22] demonstrated the detrimental effects of a splenectomy on oncologic outcomes after the resection of pancreatic adenocarcinoma. They concluded that a splenectomy should be avoided in treating exocrine pancreatic cancer at any location, except in cases of tumor proximity or invasion. Although the effects of splenectomy on the antitumor immune system in vivo remain controversial, some experimental evidence suggests that the spleen plays a very important role in the antitumor immune system, and that splenectomy could encourage further hepatic or pulmonary metastasis [23–25].
The present study was basically a retrospective design. Also, the protocols for pathologic assessment of the retrieved LNs and surgical specimens might have been different in each institution. Especially, No. 10 LNs were always retrieved in resected specimens, so it is not clear whether No. 10 LNs were contaminated by some part of No. 11 LNs; it is also not clear whether patients with spleen preserved by means of RAMP will survive without significant spleen-related morbidity. However, our present observations are very provocative and surely should be readdressed in a future prospective trial. We suggest that a future prospective study should confirm the technical feasibility and safety of RAMP; determine the appropriate tumor conditions for RAMP, such as the optimum distance from the tumor edge to the splenic hilum for splenectomy-omitting radical left-sided pancreatectomy; and determine the potential immunologic role of the preserved spleen in treating left-sided pancreatic cancer. If a future study based on our present concept of RAMP could give sound answers to these questions, our goal would be a prospective randomized comparative study of RAMPS and RAMP in well-selected left-sided pancreatic cancers.
In conclusion, under the rationale of potential LN metastasis in the splenic hilar areas in left-sided pancreatic cancer, most patients might undergo an unnecessary splenectomy. Our present study suggests a splenectomy-omitting radical pancreatectomy, RAMP, would be also feasible for treating well-selected left-sided pancreatic cancers because splenic hilar LN metastasis is rare. The role of routine splenectomy in the treatment of left-sided pancreatic cancer needs to be re-evaluated. Splenectomy, instead of being performed as a routine procedure, should be recommended only for patients with direct tumor invasion of the splenic hilum, proximity of the primary cancer to the spleen, and suspicion of splenic hilar LN metastasis on preoperative imaging studies. The oncologic and tumor immunologic effects of preserving the spleen in treating left-sided pancreatic cancer should be fully investigated in future studies.
References
Crippa S, Bassi C, Warshaw AL, Falconi M, Partelli S, Thayer SP, et al. Middle pancreatectomy: indications, short- and long-term operative outcomes. Ann Surg. 2007;246:69–76.
Warshaw AL. Conservation of the spleen with distal pancreatectomy. Arch Surg. 1988;123:550–3.
Kim DH, Kang CM, Hwang HK, Lee WJ, Chi HS. “Extended” distal pancreatectomy with segmental resection of both splenic vessels; extended Warshaw’s procedure. Korean J Hepatobiliary Pancreat Surg. 2010;14:248–53.
Choi SH, Hwang HK, Kang CM, Yoon CI, Lee WJ. Pylorus- and spleen-preserving total pancreatoduodenectomy with resection of both whole splenic vessels: feasibility and laparoscopic application to intraductal papillary mucin-producing tumors of the pancreas. Surg Endosc. 2012;26:2072–7.
Strasberg SM, Linehan DC, Hawkins WG. Radical antegrade modular pancreatosplenectomy procedure for adenocarcinoma of the body and tail of the pancreas: ability to obtain negative tangential margins. J Am Coll Surg. 2007;204:244–9.
Strasberg SM, Drebin JA, Linehan D. Radical antegrade modular pancreatosplenectomy. Surgery. 2003;133:521–7.
Mitchem JB, Hamilton N, Gao F, Hawkins WG, Linehan DC, Strasberg SM. Long-term results of resection of adenocarcinoma of the body and tail of the pancreas using radical antegrade modular pancreatosplenectomy procedure. J Am Coll Surg. 2012;214:46–52.
Fujita T, Nakagohri T, Gotohda N, Takahashi S, Konishi M, Kojima M, et al. Evaluation of the prognostic factors and significance of lymph node status in invasive ductal carcinoma of the body or tail of the pancreas. Pancreas. 2010;39:e48–54.
Nakao A, Harada A, Nonami T, Kaneko T, Nomoto S, Koyama H, et al. Lymph node metastasis in carcinoma of the body and tail of the pancreas. Br J Surg. 1997;84:1090–2.
Seiler CA, Wagner M, Bachmann T, Redaelli CA, Schmied B, Uhl W, et al. Randomized clinical trial of pylorus-preserving duodenopancreatectomy versus classical Whipple resection—long term results. Br J Surg. 2005;92:547–56.
Tran KTC, Smeenk HG, Van Eijck CHJ, Kazemier G, Hop WC, Greve JWG, et al. Pylorus preserving pancreaticoduodenectomy versus standard Whipple procedure: a prospective, randomized, multicenter analysis of 170 patients with pancreatic and periampullary tumors. Ann Surg. 2004;240:738–45.
Gerdes B, Ramaswamy A, Bartsch DK, Rothmund M. Peripyloric lymph node metastasis is a rare condition in carcinoma of the pancreatic head. Pancreas. 2005;31:88–92.
Ogata Y, Hishinuma S. The impact of pylorus-preserving pancreatoduodenectomy on surgical treatment for cancer of the pancreatic head. J Hepato Biliary Pancreat Surg. 2002;9:223–32.
Diener MK, Knaebel HP, Heukaufer C, Antes G, Büchler MW, Seiler CM. A systematic review and meta-analysis of pylorus-preserving versus classical pancreaticoduodenectomy for surgical treatment of periampullary and pancreatic carcinoma. Ann Surg. 2007;245:187–200.
Iqbal N, Lovegrove RE, Tilney HS, Abraham AT, Bhattacharya S, Tekkis PP, et al. A comparison of pancreaticoduodenectomy with pylorus preserving pancreaticoduodenectomy: a meta-analysis of 2822 patients. Eur J Surg Oncol. 2008;34:1237–45.
Farnell MB, Pearson RK, Sarr MG, DiMagno EP, Burgart LJ, Dahl TR, et al. A prospective randomized trial comparing standard pancreatoduodenectomy with pancreatoduodenectomy with extended lymphadenectomy in resectable pancreatic head adenocarcinoma. Surgery. 2005;138:618–28; discussion 28–30.
Pedrazzoli S, DiCarlo V, Dionigi R, Mosca F, Pederzoli P, Pasquali C, et al. Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas: a multicenter, prospective, randomized study. Lymphadenectomy Study Group. Ann Surg. 1998;228:508–17.
Yeo CJ, Cameron JL, Lillemoe KD, Sohn TA, Campbell KA, Sauter PK, et al. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomized controlled trial evaluating survival, morbidity, and mortality. Ann Surg. 2002;236:355–66; discussion 66–8.
Shoup M, Brennan MF, McWhite K, Leung DH, Klimstra D, Conlon KC. The value of splenic preservation with distal pancreatectomy. Arch Surg. 2002;137:164–8.
Griffith JP, Sue-Ling HM, Martin I, Dixon MF, McMahon MJ, Axon AT, et al. Preservation of the spleen improves survival after radical surgery for gastric cancer. Gut. 1995;36:684–90.
Davis CJ, Ilstrup DM, Pemberton JH. Influence of splenectomy on survival rate of patients with colorectal cancer. Am J Surg. 1988;155:173–9.
Schwarz RE, Harrison LE, Conlon KC, Klimstra DS, Brennan MF. The impact of splenectomy on outcomes after resection of pancreatic adenocarcinoma. J Am Coll Surg. 1999;188:516–21.
Higashijima J, Shimada M, Chikakiyo M, Miyatani T, Yoshikawa K, Nishioka M, et al. Effect of splenectomy on antitumor immune system in mice. Anticancer Res. 2009;29:385–93.
Imai S, Nio Y, Shiraishi T, Tsubono M, Morimoto H, Tseng CC, et al. Effects of splenectomy on pulmonary metastasis and growth of SC42 carcinoma transplanted into mouse liver. J Surg Oncol. 1991;47:178–87.
Shiratori Y, Kawase T, Nakata R, Tanaka M, Hikiba Y, Okano K, et al. Effect of splenectomy on hepatic metastasis of colon carcinoma and natural killer activity in the liver. Dig Dis Sci. 1995;40:2398–406.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Kim, S.H., Kang, C.M., Satoi, S. et al. Proposal for splenectomy-omitting radical distal pancreatectomy in well-selected left-sided pancreatic cancer: multicenter survey study. J Hepatobiliary Pancreat Sci 20, 375–381 (2013). https://doi.org/10.1007/s00534-012-0549-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00534-012-0549-z