
Abstract
It is extremely significant to identify sleep stages accurately in the diagnosis of obstructive sleep apnea. In the study, it was aimed at determining sleep and wakefulness using a practical and applicable method. For this purpose , the signal of heart rate variability (HRV) has been derived from photoplethysmography (PPG). Feature extraction has been made from PPG and HRV signals. Afterward, the features, which will represent sleep and wakefulness in the best possible way, have been selected using F-score feature selection method. The selected features were classified with k-nearest neighbors classification algorithm and support vector machines. According to the results of the classification, the classification accuracy rate was found to be 73.36 %, sensivity 0.81, and specificity 0.77. Examining the performance of the classification, classifier kappa value was obtained as 0.59, area under an receiver operating characteristic value as 0.79, tenfold cross-validation as 77.35 %, and F-measurement value as 0.79. According to the results accomplished, it was concluded that PPG and HRV signals could be used for sleep staging process. It is a great advantage that PPG signal can be measured more practically compared to the other sleep staging signals used in the literature. Improving the systems, in which these signals will be used, will make diagnosis methods more practical.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Obstructive sleep apnea (OSA) is a syndrome, which is characterized by decreasing air stream or respiratory standstill and frequently occurs with the decrease in oxygen saturation [1, 2]. OSA diagnosis is made according to the guide concerning the identification of the sleep cases published by American Academia of Sleep Medicine (AASM) and standard measurement methods of respiratory cases occurring during sleep [3]. Diagnosis is made by means of the identification of abnormal respiratory cases occurring during the sleep of the patient. Abnormal respiratory cases refer to the respiratory disordering depending on various reasons or respiratory standstill. OSA diagnosis is made with the devices using Polysomnography (PSG) method [4]. The devices, which use this method, are called PSG devices. PSG is an expensive, time-consuming and special team required but “golden standard” method in diagnosis, which is useful for identifying various diseases concerning sleep in the laboratory environment. A standard PSG device records oral–nasal air stream, blood oxygen saturation, thorax-abdominal respiratory movements and body position with electroencephalogram (EEG), electromyogram, electrooculogram and electrocardiogram (ECG). They are recorded only when the patient stays in a sleep laboratory for a night. The patient is connected to PSG device by a sleep technician, and records are made for the whole night. After the records are completed, they are examined by attending physicians and diagnosed according to the guide published by AASM. The examination is performed in two stages. They are “Sleep Staging” and “Respiratory Scoring” stages.
Sleep staging is a method used for the analysis of the patient’s sleep stage, and it is performed in accordance with the guide published by AASM [3]. EEG, EOG, and Chin EMG records are used for this analysis [3]. The completed records are divided into 30-s pieces. Each divided piece is called epoch. Each epoch is tagged as Wake, Stage 1—N1, Stage 2—N2, Stage 3—N3 or rapid eye movement (REM) according to the characteristic features of EEG, EOG, and Chin EMG signals [3]. After sleep stages are tagged, the epochs of the patient during sleep and wakefulness are divided from each other. The purpose of sleep staging is to identify sleep and wake stages. After these processes are completed, it is proceeded to the respiratory scoring stage.
The purpose of respiratory scoring is to identify abnormal respiratory cases during sleep. Therefore, the sleep stages, which are identified after sleep staging, are processed. No respiratory case is examined in the part of wake [3]. Since OSA disease is a respiratory disorder occurring during sleep. Consequently, only the time the patient spends sleeping is analyzed.
After the process of respiratory scoring, attending physicians prepare a report. As a result of the report, Apnea/Hypopnea Index (AHI) is calculated, and OSA is diagnosed according to AHI. AHI is the value obtained, dividing the total of the numbers of apnea and hypopnea, which occur during sleep, into the sleeping hour.
PSG devices have disadvantages [5, 6]. They are not suitable for use at home. A specialist technician is needed to use devices, and the applications need to be made in hospital or laboratory [5, 6]. Furthermore, the devices entail the use of lots of electrons [5, 6]. At least 7 signals and 14 electrons are needed in order to perform sleep staging and respiratory scoring processes. This necessity restrains the use of the devices without technical knowledge. It is very difficult to use the devices without a specialist technician. Eleven of the electrons used with PSG devices are located in heading. The excess of electrons delays the time of falling asleep of the patient and removes the patient from his/her natural sleep environment. If the patient sleeps in an environment, to which she is not accustomed, it reduces the reliability of the results [6]. The cost of the devices changes approximately between 40,000 and 60,000$. Due to the high cost of the devices and the lack of qualified employees, the number of sleep laboratories around the world is few. Because of these reasons, the patients with a sleep disorder can hardly get an appointment from sleep laboratories after months or even years [5, 6].
Considering the disadvantages of OSA diagnosis time and PSG devices, there is a necessity for a new system design as an alternative to PSG devices. For this purpose, a project is conducted to develop a system that is alternative to PSG devices, has embedded software with apparatus, can be used at home, and can make sleep staging and respiratory scoring.
In this study, as a part of the project conducted; it is aimed to identify sleep stages in the most efficient and practical way. In this manner, it will be provided to make sleep staging process automatically with PSC devices. Furthermore, a new system will be developed, eliminating the deficiencies of PSG devices.
In the study, sleep staging process will be carried out with the heart rate variability (HRV) signal obtained from the signals of photoplethysmography (PPG) and PPG. The state of sleep–wake will be identified with sleep staging process. It is enough to identify the state of sleep–wake for the respiratory scoring process. Therefore, only the state of sleep-wake will be identified with the system of sleep staging developed.
PPG signal is an electrooptic method that gives information about the volume of the blood flows in the test area of the body close to the skin. PPG signal is a newly studied signal in the literature, and it includes extensive information about body [7, 8]. HRV is the analysis of time periods of heart beats. During the course of 24 h, heart rate is set by autonomic nerve system progressively in response to internal and external triggers such as stress, rest and sleep. With the alteration of HRV, sleep quality is used commonly in the diagnosis of the cases such as hypertension relating to OSA, sleep/cardiac arrhythmia relating to OSA [9]. There are many sleep staging studies conducted with HRV in the literature [10–16]. However, the common characteristic of the studies is that HRV signal has been derived from ECG. Obtaining HRV signal from ECG signal is more arduous compared to PPG signal. Consequently, HRV signal, which was used in this study, has been derived from PPG signal.
Sleep staging is made, using EEG, EOG, and Chin EMG. On the other hand, there are studies in the literature, which have been tried to be conducted more practically, using different signals [11–17]. In addition, there is also an automatic sleep staging system in the literature made with HRV signal [10–16]. As HRV signal has been derived from PPG signal, it is considered that there can be a relation between sleep stages and PPG and HRV signals. Two sleep stages were used in the study. These are sleep and wake. It is sufficient to identify whether the patient is asleep or not. For that matter, only two stages were used. Likewise, more stages can also be used in the studies. Nevertheless, the increase in the number of classes reduces the accuracy rate in the classification process.
In a study conducted in 2015, the attempts to make ECG and OSA diagnosis were made [18]. The data in the study were obtained with PSG. The feature extraction was made through 8-h ECG records taken for each patient, and the attempts to identify whether the patient was OSA or not were made. ECG features were made through 8-h records without being divided into epochs. It was identified whether the individuals were OSA or not, but OSA level was not specified. Besides, the time, during which the patient was not in sleep should not have been included in the study. Nevertheless, it was ignored during the study. Additionally, identifying the apneas, it is necessary to examine the parts, in which respiratory standstills occur. In terms of the way the study has been conducted, it basically includes many theoretical failures. It is a superficially conducted study. In this article, the attempts to identify the vital sleep stages properly for OSA diagnosis were made.
The attempts to make ECG and OSA diagnosis with another study conducted in 2015 were made [6]. In the study, ECG signal was divided into 60-s epochs, and the features were extracted. Each epoch divided into 60 s was tagged as apnea or normal. Thereafter, the classification process with the features extracted from ECG was made. After the classification process, the attempts to identify whether 60-s epochs were with apnea or not were made. The study seems to be going well in terms of the problem. However, it is necessary to develop the processes followed. The total respiratory standstills occurred in sleep were calculated during OSA diagnosis. Nevertheless, all of the ECG signals recorded were used in the study. The time, which was not spent sleeping, should have been excluded from the study in order to make a healthy study. Since the apneas, which were not calculated during sleep, may affect the condition of the disease in a different direction. Therefore, it reduces the credibility of the study it has been provided to develop a system for an active sleep staging process to prevent the mistakes.
Since this method is arduous and expensive, cheaper alternatives have been searched. Therefore, the use of polygraphic methods, especially in OSA diagnosis, increases gradually. The devices that use polygraphic methods are called Polygraph devices. Polygraph devices operate, getting a signal like PSG devices. However, these devices do not record the signals of EEG, EOG, and EMG. The attempts to make the processes, which PSG devices make, without using these signals have been made in order to use them practically [19]. Cardiopulmonary sleep studies, which are called polygraphy and do not contain EEG, have been carried out with eight-channel POLY-MESAM (PM) unity classified as III category system by American Sleep Disorders Association—ASDA [20]. Nevertheless, more practical devices which include electroencephalogram (EEG) are needed.
The purpose of this study is to evaluate a novel sleep staging method based on k-nearest neighbors classification algorithm (kNN), support vector machines (SVMs). The diagnosis of sleep stages as the first step of the diagnosis was tried to be identified using the most practical method. The study was carried out according to AASM criteria, using PPG signals. The shortcoming of many studies in the literature is not using AASM criteria for OSA diagnosis [3, 6, 21, 22]. Each writer uses the criteria that she/he has determined. But when the standard values are not taken into account for OSA diagnosis, the scientific validity of results taken must be discussed.
In the study, 46 features from PPG signal and 40 features from HRV signal are extracted. Thereafter, the features extracted from PPG and HRV are classified with the machine learning method, using both raw figure and F-score feature extraction method.
2 Materials and methods
2.1 Signal acquisition
The database used in the study was formed in the Sleep Laboratory of Chest Diseases in Sakarya Hendek Public Hospital. The database was formed from 33-channel data obtained recording 10 people throughout the night with PSG device branded SOMNOscreen Plus. However, the study was performed with PPG signals. PPG signal was taken using the electrode located in the abdominal region. The sample frequency was 128 Hz for PPG signal. While the dates were taken, the patients were provided a laboratory environment in which they could sleep, and the patients slept for almost 7–8 h after PSG device electrodes were connected, and the records were taken.
After the records had been taken, they were examined by attending physicians and, sleep staging and respiratory scoring processes were made. Sleep staging and respiratory scoring processes were performed according to AASM guide [3]. Accordingly, the records were divided into 30-s epochs for sleep staging process, and EEG, EOG, and chin EMG were used. As for respiratory scoring processes, the oronasal thermal sensor was used for air stream control; abdominal and thorax belts were used for ventilatory effort, and pulse oximetry was used for the measurement of oxygen saturation. Having been analyzed by the doctor, the data became processable. The statistical information relating to the data used in the study is given in the table. As it is stated in Table 1, in the study 8452 30-s epochs were used in total; 1479 epochs were tagged “Wake”, 6973 epochs were tagged “Sleep”.
2.2 Signal pre-processing
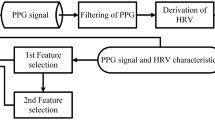
The data collected were subjected to many processes according to the stream diagram in Fig. 1, and the results of the analysis were obtained.

The flow diagram of photoplethysmography and heart rate variability signals process
At the first step, the numerical filter was designed and applied in order to clean artifact and noise occurring due to PPG signal. The filter which bands Chebyshev Type II between 0.1 and 20 Hz to PPG signal and, afterward, moving average filter were applied. The sample PPG signals of the sleep–wake states obtained after filtering process are shown in Fig. 2 during the period of time. According to the figure, it is clear that there is signal alteration between the groups.

Sample photoplethysmography signal
After PPG signal had been cleaned, HRV signal was derived from this signal in order to use PPG signal more effectively. Afterward, feature extraction process from PPG and HRV signals was performed. The extracted features were classified both applying extraction algorithm and through the raw situation. Classification processes were evaluated with performance assessment criteria.
PPG signal and HRV signal derived from PPG signal are shown in Fig. 3. The signals in the figure are 5-s signals. As the sample frequency of PPG signal is \(fs=128\) Hz, the total sample number of signals is \(128\times 5=640\). The local maximum points of PPG signal were identified in order to derive HRV signal. Four local maximum points, \(A_{P1}, A_{P2}, A_{P3}\) and \(A_{P4}\), identified are marked with “\(*\)” in Fig. 3. As the elements of HRV signal calculated using the points, the \(A_{H1}, A_{H2}\) and \(A_{H3}\) values are also shown in Fig. 3. The marked points are the sample numbers that correspond to their marked point in the x-axis. For instance, while the coordinates of the point in which \(A_{P1}\) is located, are 105,79.8726; \(A_{P1}\) is 105. While the coordinates of the point, in which \(A_{P2}\) is located, are 246, 80.5023; \(A_{P2}\) is 246.

Derivation of the HRV signal from the PPG signal
N, as the number of local maximum points of PPG signal and it is \(i=1,2,3\ldots (N-1)\), the coefficients of HRV are calculated as they are in equation 1. The coefficients of HRV signal composed are \(A_{H}\) series. The element number of \(A_{H}\) is \(N-1\). A sample calculation for \(A_{H1}\) is given in equation 1. The processes performed were applied to each 30-s PPG epoch.
2.3 Feature extraction from photoplethysmography and heart rate variability signals
In total 46 feature extractions are performed from PPG signal: 36 features in the time domain and 10 features in the frequency domain, and 40 feature extractions in total are performed from HRV signal: 30 features in the time domain and 10 features in the frequency domain. Since some of the features extracted from PPG and HRV signals were common, common expressions were made in some parts.
How feature extraction process was performed from PPG signal is shown in detail in the stream diagram of Fig. 4. According to the stream diagram, firstly local minimum and local maximum points of PPG signal are identified. The signal is divided into periods according to the local minimum and local maximum points identified. The local minimum points of the signal are accepted as the starting and end points. As the period number of the signal is T and the local minimum number is LOCMIN, the period number of the signal can be calculated as \(T=LOCMIN-1\).

The used flow diagram for feature extraction from PPG signals
The identification of the local minimums and maximums of 30-s PPG signal is shown in Fig. 5. Accordingly, the first period of the signal, which has been divided into periods according to local minimum points, is shown. According to the local minimum number of signal, the period number of 30-s PPG signal can be calculated as \(T=LOCMIN-1=28-1=27\).

Finding the minimum and maximum local points for the photoplethysmography signal and single-period photoplethysmography signal
The 30-s PPG signal is divided into 27 periods in Fig. 5. The first feature extracted from the signal is obtained from 27 periods separately according to the stream diagram in Fig. 4 and being averaged; it is acquired as a feature of 30-s PPG signal. This process has been performed for each feature extraction. To give an example, one of the features extracted from PPG signal is the standard deviation of the signal. Calculating the value of standard deviation, the values of standard deviation are calculated from 27 periods separately and averaging 27 values of standard deviation, the only value of standard deviation relating to epoch is obtained. This process has been repeated for each feature extracted from PPG signal.
A great deal of different feature extraction from PPG signal has been performed in the studies in the literature. Some of the features are calculated according to the type of signal [7]. They are also called as characteristic features. In the study, the total number of feature extraction from PPG signal is 46. The first seven features are the characteristic features of the signal, and they are shown in Fig. 6 with their marks.

Characteristic features of photoplethysmography in time domain
The number one feature is systolic peak value, which is one of the characteristic features of PPG signal. Dicrotic notch is another characteristic feature of PPG signal. However, it is not located in every signal. This situation may cause mistakes in the real-time working systems. Therefore, instead of this feature, the amplitude value is taken when the value of systolic peak is reduced by half. It is the value that uncouples A1 and A2 fields in Fig. 6. The number two feature represents the value of band width in seconds by the time the amplitude of systolic peak is reduced by half. The number three feature is the value of the time in seconds, which goes by from the amplitude of Systolic peak to the point, where systolic peak is reduced by half. The number four feature represents the time, which goes by from the starting of PPG signal to the amplitude of systolic peak. The number five feature is the ratio of A1 and A2 fields to each other. This value is calculated as \(PA=A2/A1\). The number six feature represents the time, which goes by between two systolic peaks. The number seven feature represents the time, which goes by between the starting and ending of PPG signal. All of the calculations are made in seconds.
The number 8–36 features extracted from PPG signal in the time domain and the number 1–30 features extracted from HRV signal in the time domain are given in Table 2 with calculation formulas. The features with “*” mark were calculated with the special codes prepared within MATLAB [23]. They represent the x signal shown in formulas. Some features are shown with “-” in the column of “PPG/HRV Features Number”. For instance, the “Normality Test p” feature is shown with “-” in the “PPG Features Number” column and with “27” in the “HRV Features Number” column. This indication means that this feature is not calculated for PPG Signal but HRV Signal.
The 26–27 numbered HRV features are the features obtained as a consequence of Kolmogorov–Smirnov normality test. Kolmogorov–Smirnov normality test is one of the common test methods that are used in order to test whether distributions are distributed ordinarily or not [24]. P value that is obtained as a result of the test is the statistical probability value. H is the hypothesis value. While \(h=0\) represents \(H_{0}\) hypothesis, \(h=1\) represents \(H_{1}\) hypothesis. In the case it is under the value of \(p<0.05\), it is \(h=1\); and in case it is \(p>0.05\), it is determined as \(h=0\).
PPG 32–33 and HRV 28–29 numbered features are obtained as a result of the sign test. The sign test is the nonparametric equivalent of significance test [24]. It is a system that can be used in the cases in which the stage does not have a distribution normally by the time sampling retreats [24]. This test has been used, since the single-period PPG signal does not show normal distribution. The sign test examines whether median universe is equal to a certain value or not. P value obtained is a statistical probability value. H is hypothesis value. If it is \(h=0\)0, it represents \(H_{0}\) hypothesis, if it is \(h=1\), it represents \(H_{1}\) hypothesis. In the case it is under the value of \(p<0.05\), it is determined as \(h=1\); in case it is \(p>0.05\), it is determined as \(h=0\).
PPG 13–15 and HRV 6–8 numbered features are extracted using Hjort method in Table 2. Hjort parameters are three different parameters that are derived in order to represent an x sign in the time domain. They are Activity, Mobility and Complexity parameters. In the formulas, \(S^2\) represents the variance of the x signal; \(S_{1}^2\), represents the variance of the first derivative of the x signal and \(S_{2}^2\), represents the variance of the second derivative of the x signal.
Insofar, the features of the time domain, which were extracted from PPG and HRV signals, have been explained. Here, the features of the frequency domain extracted from PPG and HRV signals will be explained. Extracting the features of the frequency domain, firstly the lower frequency bands of the signals were extracted. The lower frequency bands of PPG and HRV signals are as shown in Fig. 3 [17, 25]. In the study, PPG signal was divided into three different lower frequency bands; low-frequency band (LF), mid-frequency band (MF) and high-frequency band (HF). PPG signal is represented by PPG, LF band by \(\hbox {PPG}_{\mathrm{LF}}\), MF band by \(\hbox {PPG}_{\mathrm{MF}}\), and HF band by \(\hbox {PPG}_{\mathrm{HF}}\). HRV signal was divided into three different lower frequency bands; very low-frequency band (VLF), low-frequency band (LF) and high-frequency band (HF). HRV signal is represented by HRV, VLF band by \({\hbox {HRV}}_\mathrm{{VLF}}\), LF band by \({\hbox {HRV}}_{\mathrm{LF}}\), and HF band by \({\hbox {HRV}}_{\mathrm{HF}}\).
IIR-Chebyshev Type II band-pass filter design, which has related frequency bandwidth, was made and applied to the signals in order to obtain the lower frequency bands of PPG and HRV signals. After the application, three lower frequency bands were obtained from PPG signal, and three lower frequency bands were obtained from HRV signal. There are eight signals in total including six lower frequency band signals of PPG, HRV and signals. The energies of the signals were calculated to calculate the frequency features. Energy calculation was performed according to the Eq. 2. Here, x is a signal, the energy of which was calculated.
The calculated energies are shown with the following symbols. \(E_{\mathrm{PPG}}\) represents the energy of PPG signal, \(E_{\mathrm{PPG}_{\mathrm{LF}}}\) represents the energy of LF lower frequency band of PPG, \(E_{\mathrm{PPG}_{\mathrm{MF}}}\) represents the energy of MF lower frequency of PPG, \(E_{\mathrm{PPG}_{\mathrm{HF}}}\) represents the energy of HF lower frequency of PPG, \(E_{\mathrm{HRV}}\) represents the energy of HRV signal, \(E_{\mathrm{HRV}_{\mathrm{VLF}}}\) represents the energy of VLF lower frequency band of HRV, \(E_{\mathrm{HRV}_{\mathrm{LF}}}\) represents the energy of LF lower frequency band of HRV and \(E_{\mathrm{HRV}_{\mathrm{HF}}}\) represents the energy of HF lower frequency band of HRV. The calculated features are numbered and shown in Table 6.
2.4 Feature selection using F-score
F-score is a method that identifies the differential features of two classes. How the feature extraction is performed is shown in Fig. 7. The F-score value of each feature in data set is calculated according to Eq. 3 in order to perform this process [26]. The threshold value of F-score is calculated to identify the differential features of two classes. F-score, the threshold value of which is calculated, is the average of F-score values. If the calculated F-score value of a feature is bigger than the threshold value of F-score, the feature is selected as the differential feature of two classes. If F-score value is smaller than the threshold value of F-score, the feature is not selected as the differential feature of two classes. The more F-score value is bigger, the more differential it becomes for the classes. However, the F-score method does not show the coherence between features.

The used flow diagram for Kernel F-score feature selection
\(x_{k,i}\) feature vector in Eq. 3 is \(k=1,2\ldots ,m\) the total element number of classes is m and \(m=n_{+}+n_{-}\) positive(+) and negative(−), and i is the feature number. \(n_{+}\) and \(n_{-}\) represent, respectively, positive(+) the number of samples in class and negative(−) the number of samples in class. \(\bar{x}_i\), \(\bar{x}_i^{(+)}\) and \(\bar{x}_i^{(-)}\) are the values, respectively; i. the average value of the feature, + the average value in class and negative the average value in class. \(x_{k,i}^{(+)}\) i. represents the k. positive samples of i. feature and \(x_{k,i}^{(-)}\) represents the k. negative samples of i. feature.
2.5 Classification stage
In the study, the attempts to classify the data of two different classes (sleep–wake) were made. The purpose of the study is to provide performing the sleep staging processes, which are used in OSA diagnosis, easily in a noninvasive way. The classification process was performed, using the features that were extracted from PPG and HRV signals. The extracted features were classified in two different ways as shown in Fig. 1. Firstly, they were classified without being subjected to any process. Afterward, the F-score feature selection algorithm was applied to the features, and they were classified. Two different classifiers were used in the study. These classifiers are kNN and SVMs.
2.5.1 k-Nearest neighbors classification algorithm
k-Nearest neighbors classification algorithm is one of the controlled learning methods that solve classification problems [27]. Calculating the similarities of the data to be classified with normal behavior data in learning set; the stratification is performed with the average of k-data, which is considered to be the nearest, according to the threshold values identified. Most importantly, each feature of the classes is identified transparently beforehand. The k number of the closest adjacent, threshold value, similarity measurement and the sufficient number of normal behaviors in the learning set affect the management performance. In this study, for all kNN networks, it has been described as \(k=5\).
2.5.2 Support vector machines
SVMs are one of the best among counseling learning algorithms. They were suggested in 1995 by Cortes and Vapnik [28]. SVMs are used effectively not only in classification problems but also in the regression analysis.
Basically, SVMs provide lines that are useful for distinguishing two classes either linearly or nonlinearly. The grouping of data as (a) linear and (b) non linear is given in Fig. 8.

Distinguishing the classes as a linear and b non linear
It is a learning algorithm for the grouping process of SVMs. The purpose of the algorithm is to distinguish the data sets on a hyperplane and to classify the new data with the new error rates [29]. The closest learning data to the hyperplane are called support vector. The support data are shown in Fig. 8. The point, where the distance between the support vectors is maximum, is identified, and a curve is fitted between them. The curve is accepted as a generalized solution that distinguishes the data sets.
2.6 The used performance criteria
Different methods of the performance evaluation were used in order to test the accuracy rates of the systems suggested. These are accuracy rates, sensivity, specificity, kappa value, receiver operating characteristic (ROC), area under an ROC (AUC) and k-fold cross-validation accuracy rates. The performance evaluation criteria are explained in detail in the subtitles.
The number of data used in the study is "Wake” 6973 and "Sleep” 1479. The unbalanced distribution of data element number in data classification process affects the results in a negative way [30, 31]. There are different approaches to remedy this situation. Reducing the element number of the big group, it can be balanced to the small group or it can be approximated to the element number of the big group, deriving the data in the small group [30, 31]. It affects the results in data deriving method in a negative way [30, 31]. Due to this reason, a sample group was formed according to the systematic sample theorem from the big group in the study. In total 1603 (23 %) data were selected from 6973 (100 %) “Wake”-tagged group according to the systematic sample theorem. By this way, the numbers of the elements of the groups were balanced.
Classifying the data in the study, they were classified as two groups; learning data set and test data set. Each set is 50 % of the total data. The statistical information of data sets is given in Table 5.
2.6.1 k-fold cross-validation
The cross-verify operation is used to control the accuracy of systems that have been formed. Using this method, all data are used in the learning and test stages of the system. Performing cross-verify operation, the learning set is divided into k subsets. While \(k-1\) is used for the subset learning operation, the other set is used for the test operation. This operation is repeated for all subsets bias. The cross-verify operation is performed for \(k=10\) value in the study.
2.6.2 Confusion matrix, kappa value, F-measure and receiver operating characteristic
The accuracy rates in the test set, the sensivity and specificity values of the classes were calculated in an attempt to evaluate the performance in the study, and ROC curve was analyzed. AUC value was calculated for ROC curve, and Kappa value was calculated for the classifiers. Additionally, F-measurement was calculated.
Sensivity shows the capability of the test to distinguish patients between real patients. It varies between 0 and 1. The sensivity value of a diagnostic test is required to be 1. The fact that the sensivity value of a test is 1 shows that the test has true-diagnosed all patients. Specificity is the capability to distinguish the healthy in the real healthy. It varies between 0 and 1. It is used in the cases when the disease needs to be verified. The fact that the specificity value of the test is 1 shows that the test has true-diagnosed all of the healthy. Sensivity and specificity parameters were calculated as shown in Eqs. 5 and 6. The accuracy rate in the study was calculated as shown in Eq. 4. TP, TN, FP and FN in Eqs. 4, 5 and 6 are respectively true positives, true negatives, false positives and false negatives.
The model, the F-score of which has been calculated, is used to identify the activity of model. The obtained value is the weighted average of sensivity and specificity. The F-measurement is calculated as shown in Eq. 7. It obtains a value between 0 and 1. 1 points out that the model is perfect, and 0 points out that the model is very bad.
ROC curve and AUC value are used for the performance evaluation of diagnostic tests, which are used in the diagnosis of disease. Analyzing ROC curve, a comparison is performed after different tests of the curves are drawn one on the top of the other. A sample ROC curve is given in Fig. 9. “Class 1” represents the ideal ROC curve. “Class 2” is the ROC curve of a method used for the diagnosis of any disease. ROC curves are required to be close to the ideal for diagnostic procedures.

Sample receiver operating characteristic curve
Kappa value gives information about credibility, remedying “chance conformation” that occurs depending completely on chance. Different limit values are identified in the literature for Kappa value in terms of the degree of conformation [32]. The limit spacing in Table 6 was used in the study.
3 Results
Applying and not applying the F-score feature selection algorithm to the features extracted from PPG and HRV signals; it is classified by means of kNN and SVMs classification algorithms.
The feature numbers, which were selected from the signals after the F-score feature selection algorithm had been applied to PPG and HRV signals, are shown in Table 7. After the features had been selected, the features of the related signal were combined and classified.
The results of the features of PPG signal are shown in Table 8; the results of the features of HRV signal are shown in Table 9; and the results of classification performed with the combination of PPG and HRV signals are shown in Table 10. Two different classification operations of the signal, which are performed before and after feature selection operation, are shown in each table.
ROC curve was calculated for each grid in order to evaluate the performance of the classification processes. As the best grid result is obtained, combining PPG and HRV signals; ROC curve of this group is shown. Related ROC curve is shown in Fig. 10. Four different results of grids are given on the graphic.

ROC curves obtained for photoplethysmography and heart rate variability signals
4 Discussion and conclusions
The purpose of the study is to help diagnose OSA using the most credible method. For this purpose, it is tried to diagnose sleep stages, which is the first step in diagnosis, using the most practical method.
When a new method is developed to perform any process, it is compared with the reference methods. The fact that the similarity is obtained as 80 % as a result of the comparison proves that the new method is applicable [32]. As a consequence of the comparison between the new suggested method for sleep staging and reference method, the accuracy rate was obtained as 79.36 %, which is shown in Table 10, in the study. When the rate is examined separately, it has been shown that the new method is sufficient. However, evaluating the new method with different parameters will increase the credibility of the method. The values of AUC, k(10)-fold and F-measurement, which are shown in Table 10, are approximately 80 %. These parameters improve the credibility of the system.
In the method suggested, the primary purpose is to identify the state of sleep of the patient. The value of sensivity for sleep shown in Table 10 is 0.81. This rate shows the credibility of the method in identifying the state of sleep in a different way. The performance obtained seems to be applicable to the system in terms of the evaluation criteria. However, the kappa value shown in Table 10 is 0.59. Considering this value, it is necessary to improve the system a bit more. The features of PPG and HRV, which will represent sleep, may be extracted in order to improve the system. Moreover, it is also necessary to improve the database. The bigger the data set is in the process of the medical data, the more consistent the results become.
There is a study in literature, in which PPG data were used to identify sleep stages [17]. Nevertheless, it is necessary to improve the study. SVMs classifiers were used for sleep-wake diagnosis in the study, and in the classification, the accuracy rate was calculated as 77 %, sensivity as 0.78, and specificity as 0.72. At first sight, it may be said that the values are good. However, performing classification process; unbalanced distribution was made in data distributing. It has been informed that 25447 (90%) epochs were used for learning, and 2882 (10%) epochs were used for the test in the learning set. Classification changes data distribution and classification performance. The results are not real because the learning data are high, and the test data are low. Additionally, the epoch numbers of sleep and wake are given separately. The confidentiality of the information has reduced the credibility of the study. In this article, all details have been given in order to perform sleep staging process without any confidential information included.
There are lots of studies in the literature, in which sleep staging process has been performed using ECG signal and HRV signal derived from ECG [2, 12–16, 33, 34]. In these studies, the accuracy rate obtained for sleep-wake is approximately 70-80%. As PPG and HRV signals have been used in this article, it is expected that the results will be similar to the studies in the literature. Examining the results, it is clearly seen that the results are close to each other. In this respect, the study coincides with the literature [2, 12–16, 33, 34]. However, the fact that PPG signal can be measured more practically than ECG signal increases the practical applicability of this article.
According to the results obtained, is has been concluded that PPG and HRV signals can be used for sleep staging process. It is an advantage that PPG signal can be measured more practically than the other sleep staging signals used in the literature. Improving of the systems, in which this signal will be used, will improve the diagnosis methods. For instance, at least 3 signals and 10 electrodes are required for sleep staging process in OSA diagnosis. That PPG signal can be used instead of them will reduce the processing load.
Change history
16 July 2024
This article has been retracted. Please see the Retraction Notice for more detail: https://doi.org/10.1007/s00521-024-10067-8
References
Linz D, Linz B, Hohl M, Böhm M (2015) Atrial arrhythmogenesis in obstructive sleep apnea: Therapeutic implications. Sleep Med Rev 26:87–94
Cock VCD, Benard-Serre N, Driss V, Granier M, Charif M, Carlander B, Desplan M, Langenier MC, Cugy D, Bayard S (2015) Supine sleep and obstructive sleep apnea syndrome in Parkinson’s disease. Sleep Med 16(12):1497–1501
Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, Marcus CL, Mehra R, Parthasarathy S, Quan SF, Redline S, Strohl KP, Davidson Ward SL, Tangredi MM (2012) Rules for scoring respiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med (JCSM) 8(5):597–619
Borgström A, Nerfeldt P, Friberg D (2013) Questionnaire OSA-18 has poor validity compared to polysomnography in pediatric obstructive sleep apnea. Int J Pediatric Otorhinolaryngol 77(11):1864–1868
Bruyneel M, Ninane V (2014) Unattended home-based polysomnography for sleep disordered breathing: current concepts and perspectives. Sleep Med Rev 18(4):341–347
Song C, Liu K, Zhang X, Chen L, Xian X (2015) An obstructive sleep apnea detection approach using a discriminative hidden Markov model from ECG signals. IEEE Trans Bio-med Eng
Kavsaoğlu AR, Polat K, Bozkurt MR (2014) A novel feature ranking algorithm for biometric recognition with PPG signals. Comput Biol Med 49:1–14
Kavsaoğlu AR, Polat K, Muthusamy H (2015) Non-invasive prediction of hemoglobin level using machine learning techniques with the PPG signal’s characteristics features. Appl Soft Comput 37:983–991
Kim MS, Cho YC, Seo S-T, Son C-S, Kim Y-N (2012) Comparison of heart rate variability (HRV) and nasal pressure in obstructive sleep apnea (OSA) patients during sleep apnea. Measurement 45(5):993–1000
Hayet W, Slim Y (2012) Sleep–wake stages classification based on heart rate variability. In: 2012 5th international conference on biomedical engineering and informatics. IEEE, pp 996–999
Penzel T, Kantelhardt JW, Becker HF, Peter JH, Bunde A (2003) Detrended fluctuation analysis and spectral analysis of heart rate variability for sleep stage and sleep apnea identification. In: Computers in cardiology, 2003. IEEE, pp 307–310
Roche F, Sforza E, Duverney D, Borderies J-R, Pichot V, Bigaignon O, Ascher G, Barthélémy J-C (2004) Heart rate increment: an electrocardiological approach for the early detection of obstructive sleep apnoea/hypopnoea syndrome. Clin Sci (London, England: 1979) 107(1):105–110
Yilmaz B, Asyali MH, Arikan E, Yetkin S, Ozgen F (2010) Sleep stage and obstructive apneaic epoch classification using single-lead ECG. Biomed Eng Online 9(1):39
Poupard L, Mathieu M, Goldman M, Chouchou F, Roche F (2012) Multi-modal ECG Holter system for sleep-disordered breathing screening: a validation study. Sleep Breath = Schlaf & Atmung 16(3):685–693
Faust O, Acharya UR, NG EYK, Futita H (2016) A review of ECG-based diagnosis support systems for obstructive sleep apnea. J Mech Med Biol 16(01):1640004
Acharya UR, Chua EC-P, Faust O, Lim T-C, Lim LFB (2011) Automated detection of sleep apnea from electrocardiogram signals using nonlinear parameters. Physiol Meas 32(3):287–303
Dehkordi P, Garde A, Karlen W, Wensley D, Ansermino JM, Dumont GA (2014) Sleep stage classification in children using photoplethysmogram pulse rate variability. In: Computing in cardiology conference (CinC). IEEE, pp 297–300
Jezzini A, Ayache M, Elkhansa L, Al Abidin Ibrahim Z (2015) ECG classification for sleep apnea detection. In: 2015 international conference on advances in biomedical engineering (ICABME). IEEE, pp 301–304
Masa JF, Corral J, de Cos JS, Duran-Cantolla J, Cabello M, Hernández-Blasco L, Monasterio C, Alonso A, Chiner E, Aizpuru F, Vázquez-Polo F-J, Zamorano J, Montserrat JM, Garcia-Ledesma E, Pereira R, Cancelo L, Martinez A, Sacristan L, Salord N, Carrera M, Sancho-Chust JN, Negrín MA, Embid C (2013) Effectiveness of three sleep apnea management alternatives. Sleep 36(12):1799–1807
Annakkaya AN, Balbay Ö, Cahit BLGN, Erbafi M, Arbak P (2004) Outcomes of the eight-channel ambulatory recording unit in a sleep laboratory. Eur J Pulmonol 6(1):12–23
Gaurav G, Mohanasankar S, Kumar V Jagadeesh dec (2013) Apnea sensing using photoplethysmography. In: 2013 seventh international conference on sensing technology (ICST). IEEE, pp 285–288
Lazaro J, Gil E, Vergara JM, Laguna P (2012) OSAS detection in children by using PPG amplitude fluctuation decreases and pulse rate variability. Comput Cardiol 2012:185–188
Wallisch ASDP, Lusignan ME, Benayoun MD, Baker TI, Hatsopoulos NG (2014) MATLAB for neuroscientists: an introduction to scientific computing in MATLAB
Ramachandran KM, Chris P (2015) Elsevier, Tsokos. Mathematical Statistics with Applications in R
Shi P, Zhu Y, Allen J, Hu S (2009) Analysis of pulse rate variability derived from photoplethysmography with the combination of lagged Poincaré plots and spectral characteristics. Med Eng Phys 31(7):866–871
Polat K, Güneş S (2009) A new feature selection method on classification of medical datasets: Kernel F-score feature selection. Expert Syst Appl 36(7):10367–10373
Şahan S, Polat K, Kodaz H, Güneş S (2007) A new hybrid method based on fuzzy-artificial immune system and k-nn algorithm for breast cancer diagnosis. Comput Biol Med 37(3):415–423
Cortes C, Vapnik V (1995) Support-vector networks. Mach Learn 20:273–297
Mandhala VN, Sujatha V, Devi BR (2014) Scene classification using support vector machines. In: 2014 IEEE international conference on advanced communications, control and computing technologies. IEEE, pp 1807–1810
Pérez-Godoy MD, Rivera AJ, Carmona CJ, del Jesus MJ (2014) Training algorithms for radial basis function networks to tackle learning processes with imbalanced data-sets. Appl Soft Comput 25:26–39
Rasch D, Teuscher F, Guiard V (2007) How robust are tests for two independent samples? J Stat Plan Inference 137(8):2706–2720
Alpar R (2010) Applied statistic and validation—reliability. Detay Publishing, Ankara
Wang J-S, Shih G-R, Chiang W-C (2012) Sleep stage classification of sleep apnea patients using decision-tree-based support vector machines based on ECG parameters. In: Proceedings of 2012 IEEE-EMBS international conference on biomedical and health informatics. IEEE, pp 285–288
Yu S, Chen X, Wang B, Wang X (2012) Automatic sleep stage classification based on ECG and EEG features for day time short nap evaluation. In: Proceedings of the 10th world congress on intelligent control and automation. IEEE, 4974–4977
Acknowledgments
This research was supported by The Scientific and Technical Research Council of Turkey (TUBITAK) through The Research Support Programs Directorate (ARDEB) with project number of 115E657, and project name of “A New System for Diagnosing Obstructive Sleep Apnea Syndrome by Automatic Sleep Staging Using Photoplethysmography (PPG) Signals and Breathing Scoring” and by The Coordination Unit of Scientific Research Projects of Sakarya University. Produced from the doctoral thesis “Development of A New System for The Diagnosis of Sleep Staging and Sleep Apnea Syndrome” under the consultancy of the authors (Mehmet Recep Bozkurt), this study was supported by the SAU Commission of Scientific Research Projects (Project No: 2014-50-02-022). The ethics committee report numbered 16214662/050.01.04/70 from Sakarya University Deanship of Faculty of Medicine, and the data use permission numbered 94556916/904/151.5815 from T.C. Ministry of Health Turkey Public Hospitals Authority Sakarya Province General Secretariat of Association of Public Hospitals were received to perform the study.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Uçar, M.K., Bozkurt, M.R., Bilgin, C. et al. RETRACTED ARTICLE: Automatic sleep staging in obstructive sleep apnea patients using photoplethysmography, heart rate variability signal and machine learning techniques. Neural Comput & Applic 29, 1–16 (2018). https://doi.org/10.1007/s00521-016-2365-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00521-016-2365-x