
Abstract
Purpose
To systematically review evidence regarding the benefits of Internet-based psycho-educational interventions among cancer patients.
Methods
We performed a systematic review with meta-analysis and qualitative evidence synthesis. Systematic searches for published studies in English or Chinese identified eligible randomized and clinical controlled trials. The following databases were searched: Medline, Embase, CINAHL, PsycINFO, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), Proquest Digital Dissertations, Foreign Medical Retrieval System, China National Knowledge Infrastructure, China Science and Technology Journal Database, China Wanfang Database, and Taiwanese Airiti Library. We also searched the gray literature and reviewed reference lists from relevant articles. Studies were scored for quality using the Cochrane Risk of Bias Tool.
Results
Seven eligible studies (1220 participants) were identified that used three intervention tools: website programs (n = 5), e-mail counseling (n = 1), and a single-session psycho-educational intervention (n = 1). The quality of all studies was moderate. The meta-analysis showed that Internet-based psycho-educational interventions had a significant effect on decreasing depression (standardized mean difference (SMD) − 0.58, 95% confidence interval (CI) (− 1.12, − 0.03), p = 0.04) and fatigue (mean difference (MD) − 9.83, 95% CI (− 14.63, − 5.03), p < 0.01). However, there was no evidence for effects on distress (SMD − 1.03, 95% CI (− 2.63, 0.57), p = 0.21) or quality of life (MD 1.10, 95% CI (− 4.42, 6.63), p = 0.70).
Conclusion
Internet-based psycho-educational interventions reduce fatigue and depression in cancer patients. More rigorous studies with larger samples and long-term follow-up are warranted to investigate the effects of these interventions on cancer patient quality of life and other psychosocial outcomes.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Cancer is the highest barrier to increasing life expectancy and may be the leading cause of death worldwide in the twenty-first century [1]. The process of treating cancer is usually complex. The side effects of cancer treatments (e.g., chemotherapy, radiation therapy) may have an impact on cancer patients’ self-efficacy and quality of life (QoL) and their physical function [2]. Even after treatment, cancer survivors continue to face a variety of difficulties and challenges that can affect their QoL [3], a term describing the modification and enhancement of life attributes. There are a few common symptoms in patients with cancer, such as anxiety, depression, and fatigue [4,5,6,7]. In addition to physical symptoms, patients frequently struggle with psychological issues [8, 9]. Moreover, cancer patients often lack confidence [10] or feel ill-prepared to effectively manage life following cancer treatment, resulting in a common need for information [11]. These cancer-related sequelae may significantly impact patient mental health and QoL [12, 13]. In response, supportive and rehabilitative services may be used to promote health [14]. Furthermore, cancer survivors may feel a need to cope with and relieve symptoms after treatment [15].
Background
Psycho-educational interventions are defined as information provided about health-related condition and management [16]. Psycho-educational interventions combine patient education with activities [17, 18], such as structured, time-limited interventions consisting of stress management, health education, and psychological support [19]. This differs from psychosocial interventions that represent less specific interventions through social support, suggestions, and encouragement in order to improve mental health [20]. There is considerable overlap between psycho-educational interventions and specific psychotherapies, such as cognitive behavioral therapy (CBT) and family-focused therapy (FFT) [21]. CBT can be conducted individually and in a group, family involvement, and the computer or Internet-based [22], which can be included as a component of psycho-education.
Given the educational and support needs of patients regarding their disease, they increasingly use online resources to learn how to cope with illness, as opposed to traditional psychosocial resources such as healthcare professionals, family members, and friends [23]. A systematic review has shown that e-Health interventions (e.g., teleconference, interactive app-based project, and internet-based program) can improve fatigue and self-efficacy in cancer survivors [24]. The Internet has various advantages, including accessibility, availability, and anonymity, which can overcome spatial, temporal, and psychological barriers [25]. The online environment can allow anonymous access to information and support, at anytime, anywhere, and in a format easily tailored and personalized for patients [26, 27]. Thus, use of the Internet has facilitated numerous new ways to deliver psycho-educational interventions to cancer patients [28].
The Internet is used more frequently for particular types of intervention and to provide psycho-oncological support [27, 29]. Cancer patients use the Internet to seek information after diagnosis [30]. Recent studies have integrated the use of the Internet into patient care through information support [31], peer support groups [32, 33], patient forums [34], and therapeutic games [35]. Several online interventions are therapist guided and appear to have similar efficacy as face-to-face interventions [21]. Hence, this is a promising medium to deliver psycho-oncological interventions [27]. Several stand-alone web-based psychosocial interventions have been evaluated; however, only preliminary results have been published [32, 36,37,38]. Studies have explored the effects of Internet-based psycho-educational interventions on QoL [39], distress [40], anxiety [41], and fatigue [42]. These studies included different instruments, durations, frequencies, and outcomes. Furthermore, several groups investigated the use and effects of Internet-based self-help and reported meaningful results; for example, the use of discussion boards can improve social support [43, 44]. To date, evidence regarding the effects of Internet-based psycho-educational intervention on cancer patients has not been synthesized for clinical practice.
The review
Aims
The aim of this review was to evaluate the available evidence regarding the effects of Internet-based psycho-educational interventions on mental health and QoL among cancer patients.
Design
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement, using the order prescribed by the Cochrane Collaboration. The protocol for this systematic review was registered in PROSPERO (registration number: CRD42018097205).
Search methods
Articles were identified through a systematic search of 12 electronic databases: Medline, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), PsycINFO, Web of Science, Cochrane Central Register of Controlled Trials, Proquest Digital Dissertations, Foreign Medical Retrieval System, China National Knowledge Infrastructure, VIP Journal Integration Platform, China Wanfang Database, and Taiwanese Airiti Library, from their inception to March 2019. We also reviewed the bibliographies of relevant review articles to identify additional publications. Search strategies were tailored for each database (see Additional file 1).
Inclusion criteria
The inclusion criteria were as follows:
-
(a)
Study designs: randomized controlled trials or clinical controlled trials in English or Chinese;
-
(b)
Participants: patients with confirmed diagnosis of any cancer, with no restriction on the age, sex, or ethnicity;
-
(c)
Interventions: Internet-based instruments such as websites, smartphone applications, online games, and online video for conducting psycho-education interventions. Meanwhile, interventions were required to meet the definition of psycho-education or use material related to psycho-education or as a component of psycho-education;
-
(d)
Controls: eligible controls were required to receive standard care or usual care, or be a conditional control group;
-
(e)
Outcomes: studies were eligible if a mental health outcome (e.g., QoL, depression, anxiety, distress, life satisfaction) was assessed.
Exclusion criteria
-
(a)
Study designs: other types of studies (e.g., observational, review, protocol, case reported) were excluded;
-
(b)
Participants: patients who could not use internet by themselves or had cognitive disorders;
-
(c)
Interventions: participants who were receiving other types of interventions (e.g., music therapy, life review therapy, or group-based or family involvement cognitive therapy);
-
(d)
Studies without available full-text articles were excluded.
Search outcomes
After analyzing the characteristics of the selected studies, two reviewers codified and organized the articles. The extracted data included publication details, study designs, participants, sample sizes, interventions, facilitators, settings, outcomes, measuring instruments, and results. Data were independently extracted by two reviewers, and a consensus was reached by consulting with a senior researcher. The reliability (kappa value) between the two reviewers was 0.830 (p < 0.001). If any information was missing or unclear, the original authors were contacted by e-mail for more information.
Quality appraisal
The tool provided by the Cochrane Collaboration was used to assess the risk of bias based on the adequacy of sequence generation, allocation concealment, blinding of patients and personnel, blinding of outcome assessment, reporting of incomplete outcome data, selective outcome reporting, and other sources of bias [45]. The risk of bias for each outcome was categorized into three levels: low, high, and unclear. The quality of included studies was independently assessed by the two researchers. Disagreements were resolved by discussion, or if unsuccessful, by consulting the senior researcher. The inter-rater reliability (kappa value) was 0.874 (p < 0.001).
Data abstraction
The data extraction forms for each publication included in the review were independently completed by the two reviewers. They read each article and recorded information regarding the study design, participants, intervention characteristics, and outcomes. Data extraction forms were used to complete a narrative synthesis of the results. Additionally, evidence regarding the effects of Internet-based psycho-educational interventions on the mental health and QoL of cancer patients was synthesized by collating the publication details, study designs, participants, interventions, samples, primary outcomes, measuring instruments, and results, in a narrative manner. Any discrepancy or uncertainties were resolved through regular meetings and discussion among the research team.
Data synthesis
Data synthesis was performed using Revman Manager 5.3, and all numeric outcome data were double entered to prevent data entry errors. Heterogeneity was quantified using I2 statistics. When I2 < 50%, a fixed effects model was used. Where there was evidence of a significant heterogeneity (I2 ≥ 50%), a random effects model was applied. A narrative overview was taken when I2 > 75%. For continuous data that used the same scale, the mean difference (MD) was chosen as the summary measure. When the same outcome was measured by different scales, the standardized mean difference (SMD) was used. Outcomes were pooled and presented in a narrative form and in tables.
Results
Description of the studies
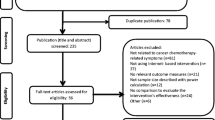
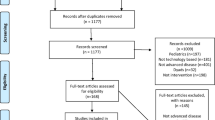
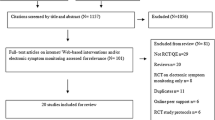
After systematically searching 12 electronic databases, a total of 868 studies were selected. After removal of duplicates, 552 studies remained. Following the screening of titles and abstracts, 51 studies were identified for further assessment. After reading the full articles, 7 studies were finally identified for inclusion in this review. The flow of selection is described in Fig. 1. All seven eligible studies were randomized controlled trials. Four studies were performed in the Netherlands, while the others were conducted in Germany (n = 1), Korea (n = 1), and Switzerland (n = 1). The studies were published from 2011 to 2018 (n = 7). Two studies were performed in hospitals, whereas the settings for the remaining five studies were unclear. Although these included studies have reported intervention components (e.g., CBT, PST), only one study mentioned the theoretical intervention [28] (Table 1).

Literature search flowchart. n, number of citations
Participants and professionals
The seven studies included a total of 1220 participants, of which 1034 (84.8%) were female. The range of sample sizes was 36–518 participants, with 6 having > 50 participants. Studies recruited participants with breast cancer (n = 3), with glioma (n = 1), with several types of cancer (n = 2), or who were unclear regarding cancer type (n = 1). Interventions were primarily performed by trained professionals (n = 6) including clinical psychologists, trained and supervised psychology students, and registered nurses. One study [37] did not provide a specific description of the practitioners who conducted the intervention (Table 1).
Characteristics of interventions
There were no uniform standards or commonalities across all included studies. Interventions were diverse in terms of the instrument, duration, frequency, setting, and facilitator. The tools used for Internet-based psycho-educational interventions included websites (n = 5), tablet personal computers (PCs) (n = 1), and e-mail (n = 1). The range of study duration was 3–16 weeks, including 3 weeks (n = 1), 5 weeks (n = 1), and 8–12 weeks (n = 5). The frequencies of interventions were reported as at least once per week (n = 3) or unclear (n = 4). The facilitators of Internet-based psycho-educational interventions included clinical psychologists or nurses, supervised psychology students (n = 6) who had been well trained in the use of psycho-educational interventions, or the patients themselves (n = 1). The psycho-educational interventions could be divided into four types, including counseling, education, behavioral therapy, and social support that can be used individually or in combination. In this review, most studies were conducted using single or mixed modules. The modules for each study differed considerably. For example, the ENCOURAGE [40] program included four modules: (a) distress education, (b) cancer survivor interview, (c) coping strategies and stress management, and (d) psychosocial services. Conversely, the BREATH components were based on cognitive behavioral therapy and included information, assignment, assessment, and videos [37]. The KNW program included eight modules, the majority of which were self-management training modules covering topics such as returning to work, fatigue, anxiety and depression, social relationships and intimacy issues, physical activity, diet, and smoking cessation [46]. Another study was implemented by online consultation [39]. Five studies have published study protocols [37, 39, 41, 42, 46].
Control interventions
Control groups received usual care (n = 5), standard care (n = 1), or other control therapy (e.g., a single-session movie clip) (n = 1). Usual care included routine nursing and health education. In this review, standard care involved regular visits to a medical specialist (medical, surgical, or radiation oncologist, and/or oncology nurse) every 3 or 4 months during the first year of follow-up.
Variables, instruments, and results
Ten outcome variables measured using 16 scales were identified. Most studies used validated (self-rating) questionnaires or scales. In the selected studies, QoL was assessed using various scales as follows: EORTC QLQ-C30 [39, 40, 46], Short-form 8 Health Survey [47], The Short-Form Health Survey [48], and Functional Assessment of Chronic Illness Therapy-Fatigue [49]. Mental health (e.g., distress) was assessed using The Brief Symptom Inventory [50], Dutch Distress Thermometer/Problem List [51], the Hospital Anxiety and Depression Scale (HADS) [52], and Symptom Checklist-90 [53].
Outcomes
Distress
Five studies [28, 37, 39,40,41] assessed the effect of Internet-based psycho-educational interventions on distress. However, just four studies [28, 37, 39, 40] including 355 participants were evaluated in the meta-analysis for the reason that one study [41] only reported the interquartile range and median of outcomes (no mean values and standard deviation were reported). The pooled data of the four studies showed no significant difference in improvement between the intervention and control groups (SMD − 1.03, 95% confidence interval (CI) (− 2.63, 0.57), p = 0.21) (Fig. 2a).

Effect sizes of the Internet-based psycho-educational intervention group versus the control group on (a) distress rating scores, (b) depression rating scores, (c) quality of life rating scores, and (d) fatigue rating scores
Depression
Four studies [28, 41, 42, 46] investigated the effects of Internet-based psycho-educational interventions on depression. Three studies [28, 42, 46] including 462 participants were evaluated in the meta-analysis. The data from one study [41] was not pooled because the mean values and standard deviation of outcomes were not reported. Meta-analysis showed a significant difference in improvement between the intervention and control groups (SMD − 0.58, 95% CI (− 1.12, − 0.03), p = 0.04) (Fig. 2b).
QoL
A total of six studies [28, 39,40,41,42, 46] reported the effects of Internet-based psycho-educational interventions on QoL among cancer patients. Different scales were used to measure QoL. Two studies including 185 participants that provided sufficient data were combined in the meta-analysis [39, 40]. The result showed no significant difference in improvement between the intervention and control groups (MD 1.10, 95% CI (− 4.42, 6.63), p = 0.70) (Fig. 2c).
Fatigue
Two studies assessed the effect of Internet-based psycho-educational interventions on fatigue [42, 46]. The pooled data included 427 participants and showed a significant difference in improvement between the intervention and control groups (MD − 9.83, 95% CI (− 14.63, − 5.03), p < 0.01) (Fig. 2d).
Additional outcomes
Other outcomes were only described in one study. They reported that for cancer patients, empowerment was not affected by the Internet-based psycho-educational interventions (− 1.71; 95% CI, 5.2 to − 1.79; p = 0.34). One study showed a significant effect on anxiety using HADS (U = 69.0; p = 0.006) [28]. One of these studies reported that for breast cancer patient, online counseling via e-mail for breast cancer patients can increase their satisfaction [39]. One reported that using of the ENCOURAGE program had improvement in optimism and control more than inpatients in the control group (Cohen’s d = 0.65) [40].
Quality of evidence
The Cochrane Risk of Bias Tool was used to assess the risk of bias. All studies were rated “B,” suggesting a moderate risk of bias. Although all included studies used randomization, only four described the generation of the random sequence. Four studies reported allocation concealment. In most studies, patients or researchers were not blinded because of the nature of Internet-based psycho-educational interventions. Only one study reported that outcome assessors were blinded to the intervention groups. All studies reported discontinuation rates and provided detailed reasons (Figs. 3 and 4).

Risk of bias summary: a review of authors’ judgments regarding each risk of bias item for each included study

Risk of bias graph: a review of authors’ judgments regarding each risk of bias item presented as percentages across all included studies
Discussion
To the best of our knowledge, this is the first review to explore the effects of Internet-based psycho-educational interventions on mental health and QoL among cancer patients. Seven RCTs, with a total sample of 1220 participants, were identified for inclusion in the review. The meta-analysis showed that Internet-based psycho-educational interventions significantly reduced depression and fatigue, but there was no evidence for effects on distress and QoL among cancer patients.
Previous studies indicate that online interventions have the potential to improve mental health in cancer patients, including the amelioration of depression and fatigue [54, 55]. A systematic review reported that Internet-based interventions conducted by healthcare professionals have elicited positive effects on distress among cancer patients [56]. Although only two of the included studies have reported significant improvements in QoL among cancer patients [28, 41], the results of the present meta-analysis did not indicate significant differences in QoL outcomes between the intervention and comparison groups (or the conditional control groups), which is contrary to the results of a previous study [57]. For some important outcomes (e.g., anxiety, empowerment, and satisfaction) that were only reported in one study, it was not appropriate to draw a conclusion because the evidence was insufficient. Caution is warranted when interpreting the outcomes, considering the limited number of studies.
Internet-based interventions incorporate multiple behavior change techniques and are increasingly being used as an efficient method to improve support for cancer patients, overcoming obstacles such as time, mobility, and geography [58, 59]. Our review found that Internet-based psycho-educational interventions usually include various components (e.g., CBT and PST), which might have short-term effects on mental health among cancer patients. The intervention schedules, intensity, and duration were not described in detail. The relative value and importance of intervention elements and frequency for cancer patient outcomes remain unclear. Therefore, the effectiveness of specific components should be further studied.
In our review, evidence for the long-term effects of Internet-based psycho-educational interventions among cancer patients was limited. One study reported that during a 12-month measurement period to assess long-term effects of interventions on QoL among cancer patients, no significant difference was found between the intervention and control groups [46]. In comparison, a review reported that telepsychology interventions ameliorated patient distress and decreased depression symptoms over time [57]. More trials are needed to appropriately explore the long-term effects of Internet-based psycho-educational interventions among cancer patients and survivors.
In the seven studies covered by this review, the Internet-based psycho-educational interventions were conducted by various individuals, including clinical psychologists, nurses, a researcher-psychologist, a trained and supervised psychology student, or the patients themselves. Although the benefits from having psychologists versus RNs remain unclear because of the limited evidence, a previous study has indicated that patients tend to rely on professionals when receiving online support [60]. Healthcare professionals are often involved in conducting Internet-based interventions that would be expected to have a positive impact on patients’ health [59]. It is therefore important that these professionals receive appropriate psychological counseling training, so that they can better serve as counselors or therapists on online platforms to resolve psychological issues among cancer patients [59, 60].
In this review, the majority of participants who accessed Internet-based psycho-educational interventions were women. Gender differences may play a role in the effectiveness of Internet-based psycho-educational interventions. Previous studies have reported that cancer patients who are female have a higher tendency to participate in online interventions [19, 32]. This may be because women have higher levels of interest in Internet-based solutions for coping with health problems and are more likely to complete online programs [61]. This review indicated that women may potentially benefit more from Internet-based psycho-educational interventions compared with men.
Participants who were lost to follow-up or those who discontinued the intervention were considered dropouts. In this review, the main reasons for discontinuation included the individual patient circumstances (e.g., unwillingness, exhaustion, finding the interventions excessively burdensome, or lack of satisfaction with the interventions) and disease progression. Additionally, patient expectations from the intervention, the timing of the intervention node, and the duration of intervention may also affect withdrawal from the interventions or lack of engagement. The rate of discontinuation is an issue worthy of investigation, and a particularly common problem for Internet-based psychological interventions, which are typically associated with low adherence [62, 63]. Previous study indicates that several strategies (e.g., e-mail reminders, individualized feedback) may have a positive influence on adherence for online-based interventions [64]. The present findings should serve as a reminder for healthcare professionals that specific intervention procedures and the individual characteristics of the participants should be fully considered to minimize attrition rates when implementing Internet-based psycho-educational interventions.
Limitations
This systematic review was characterized by some limitations. Firstly, the review was limited to published studies, which may have introduced publication bias. Secondly, this review included only English or Chinese studies, potentially introducing publication and language biases. Thirdly, the measurement instruments varied in most included studies, resulting in heterogeneity for important outcomes. Therefore, it was difficult to pool all the data and conduct subgroup analyses. Finally, it was necessary to combine and compare results due to the heterogeneity between studies.
Implications and recommendations
Our findings have implications whereby Internet-based psycho-educational interventions may be effective in improving depression and fatigue and can be used as a part of stepped care in clinical practice. Future studies can be conducted to investigate the effectiveness of different components from Internet-based psycho-educational interventions among cancer patients/survivors. Intervention manuals or protocols guided by related conceptual framework should be provided to monitor the treatment fidelity of these interventions. There is insufficient evidence regarding the efficacy of Internet-based psycho-educational interventions in improving QoL; more rigorously designed studies that generate high-quality data are warranted to investigate the effects of Internet-based psycho-educational interventions on the QoL of patients with cancer in the future.
Conclusions
This review demonstrated that Internet-based psycho-educational interventions may be effective in improving mental health symptoms such as depression and fatigue among patients with cancer. As such, Internet-based psycho-educational interventions with various components can be used to complement usual care so that cancer patients and survivors can gain psychological support and better manage health-related symptoms.
References
Bray F, Ferlay J, Soerjomataram I, Siegel R, Torre L, Jemal A (2018) Global Cancer Statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68:394–424
Sajjad S, Ali A, Gul RB, Mateen A, Rozi S (2016) The effect of individualized patient education, along with emotional support, on the quality of life of breast cancer patients - a pilot study. Eur J Oncol Nurs 21:75–82
Wu H, Harden J (2015) Symptom burden and quality of life in survivorship: a review of the literature. Cancer Nurs 38:E29–E54
Brown LF, Kroenke K, Theobald DE, Wu J, Tu W (2010) The association of depression and anxiety with health-related quality of life in cancer patients with depression and/or pain. Psychooncology 19:734–741
Mitchell A, Ferguson D, Gill J, Paul J, Symonds P (2013) Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: a systematic review and meta-analysis. Lancet Oncol 14:721–732
Prue G, Rankin J, Allen J, Gracey J, Cramp F (2006) Cancer-related fatigue: a critical appraisal. Eur J Cancer 42:846–863
Simard S, Thewes B, Humphris G, Dixon M, Hayden C, Mireskandari S, Ozakinci G (2013) Fear of cancer recurrence in adult cancer survivors: a systematic review of quantitative studies. J Cancer Surviv 7:300–322
Armes J, Crowe M, Colbourne L, Morgan H, Murrells T, Oakley C, Palmer N, Ream E, Young A, Richardson A (2009) Patients’ supportive care needs beyond the end of cancer treatment: a prospective, longitudinal survey. J Clin Oncol 27:6172–6179
Schmid-Büchi S, Halfens R, Dassen T, van den Borne B (2011) Psychosocial problems and needs of posttreatment patients with breast cancer and their relatives. Eur J Oncol Nurs 15:260–266
Foster C, Fenlon D (2011) Recovery and self-management support following primary cancer treatment. Br J Cancer 105(Suppl 1):S21–S28
Stanton A (2012) What happens now? Psychosocial care for cancer survivors after medical treatment completion. J Clin Oncol 30:1215–1220
Bokhour B, Clark J, Inui T, Silliman R, Talcott J (2001) Sexuality after treatment for early prostate cancer: exploring the meanings of “erectile dysfunction”. J Gen Intern Med 16:649–655
Gray R, Fitch M, Phillips C, Labrecque M, Klotz L (1999) Presurgery experiences of prostate cancer patients and their spouses. Cancer Pract 7:130–135
Alfano C, Ganz P, Rowland J, Hahn E (2012) Cancer survivorship and cancer rehabilitation: revitalizing the link. J Clin Oncol 30:904–906
Allen JD, Savadatti S, Levy AG (2009) The transition from breast cancer ‘patient’ to ‘survivor’. Psychooncology 18:71–78
Sin J, Gillard S, Spain D, Cornelius V, Chen T, Henderson C (2017) Effectiveness of psychoeducational interventions for family carers of people with psychosis: a systematic review and meta-analysis. Clin Psychol Rev 56:13–24
Barsevick A, Sweeney C, Haney E, Chung E (2002) A systematic qualitative analysis of psychoeducational interventions for depression in patients with cancer. Oncol Nurs Forum 29:73–87
Lukens EP, McFarlane WR (2004) Psychoeducation as evidence-based practice: considerations for practice, research, and policy. Brief Treat Crisis Interv 4:205–225
Kohl LF, Crutzen R, Vries NKD (2013) Online prevention aimed at lifestyle behaviors: a systematic review of reviews. J Med Internet Res 15:e146
Douglas MacInnes SM (2019) Psychological and psychosocial interventions offered to forensic mental health inpatients: a systematic review. BMJ Open 9:e024351
Bond K, Anderson IM (2015) Psychoeducation for relapse prevention in bipolar disorder: a systematic review of efficacy in randomized controlled trials. Bipolar Disord 17:349–362
Sigurvinsdottir AL, Jensinudottir KB, Baldvinsdottir KD, Smarason O, Skarphedinsson G (2019) Effectiveness of cognitive behavioral therapy (CBT) for child and adolescent anxiety disorders across different CBT modalities and comparisons: a systematic review and meta-analysis. Nord J Psychiatry:1–13
Dunkel-Schetter C (1984) Social support and cancer: findings based on patient interviews and their implications. J Soc Issues 40:77–98
Xu A, Wang Y, Wu X (2019) Effectiveness of e-health based self-management to improve cancer-related fatigue, self-efficacy and quality of life in cancer patients: systematic review and meta-analysis. J Adv Nurs 75:3434–3447
Owen J, Klapow J, Roth D, Nabell L, Tucker D (2004) Improving the effectiveness of adjuvant psychological treatment for women with breast cancer: the feasibility of providing online support. Psychooncology 13:281–292
Beatty L, Lambert S (2013) A systematic review of internet-based self-help therapeutic interventions to improve distress and disease-control among adults with chronic health conditions. Clin Psychol Rev 33:609–622
Leykin Y, Thekdi S, Shumay D, Muñoz R, Riba M, Dunn L (2012) Internet interventions for improving psychological well-being in psycho-oncology: review and recommendations. Psychooncology 21:1016–1025
Joo-Young Lee HYP, Jung D, Moon M, Keam B, Hahm B-J (2014) Effect of brief psychoeducation using a tablet PC on distress and quality of life in cancer patients undergoing chemotherapy: a pilot study. Psychooncology 23:928–935
Hamel L, Robbins L, Wilbur J (2011) Computer- and web-based interventions to increase preadolescent and adolescent physical activity: a systematic review. J Adv Nurs 67:251–268
Casellas-Grau A, Sumalla EC, Lleras M, Vives J, Sirgo A, León C, Rodríguez A, Campos G, Valverde Y, Borràs JM (2018) The role of posttraumatic stress and posttraumatic growth on online information use in breast cancer survivors. Psychooncology 27:1971–1978
Ryhanen AM, Siekkinen M, Rankinen S, Korvenranta H, Leino-Kilpi H (2010) The effects of Internet or interactive computer-based patient education in the field of breast cancer: a systematic literature review. Patient Educ Couns 79:5–13
Brouwer W, Oenema A, Raat H, Crutzen R, de Nooijer J, de Vries NK, Brug J (2010) Characteristics of visitors and revisitors to an Internet-delivered computer-tailored lifestyle intervention implemented for use by the general public. Health Educ Res 25:585–595
Hoybye MT, Dalton SO, Deltour I, Bidstrup PE, Frederiksen K, Johansen C (2010) Effect of Internet peer-support groups on psychosocial adjustment to cancer: a randomised study. Br J Cancer 102:1348–1354
Strickland-Marmol LB, Muro-Cacho CA, Washington K, Foulis PR (2018) “Ask the pathologist”: an Internet forum facilitating communication between cancer registrars and pathologists. Arch Pathol Lab Med 142:1275–1283
Kato PM, Cole SW, Bradlyn AS, Pollock BH (2008) A video game improves behavioral outcomes in adolescents and young adults with cancer: a randomized trial. Pediatrics 122:e305–e317
Beatty L, Koczwara B, Wade T (2016) Evaluating the efficacy of a self-guided Web-based CBT intervention for reducing cancer-distress: a randomised controlled trial. Support Care Cancer 24:1043–1051
van den Berg S, Gielissen M, Custers J, van der Graaf W, Ottevanger P, Prins J (2015) BREATH: web-based self-management for psychological adjustment after primary breast cancer--results of a multicenter randomized controlled trial. J Clin Oncol 33:2763–2771
Wootten AC, Abbott J-AM, Meyer D, Chisholm K, Austin DW, Klein B, McCabe M, Murphy DG, Costello AJ (2015) Preliminary results of a randomised controlled trial of an online psychological intervention to reduce distress in men treated for localised prostate cancer. Eur Urol 68:471–479
David N, Schlenker P, Prudlo U, Larbig W (2011) Online counseling via e-mail for breast cancer patients on the German Internet: preliminary results of a psychoeducational intervention. GMS Psycho-Social-Medicine 8
Admiraal JM, van der Velden AWG, Geerling JI, Burgerhof JGM, Bouma G, Walenkamp AME, de Vries EGE, Schröder CP, Reyners AKL (2017) Web-based tailored psychoeducation for breast cancer patients at the onset of the survivorship phase: a multicenter randomized controlled trial. J Pain Symptom Manag 54:466–475
Grossert A, Urech C, Alder J, Gaab J, Berger T, Hess V (2018) Web-based stress management for newly diagnosed cancer patients (STREAM-1): a randomized, wait-list controlled intervention study. BMC Cancer 16:780–788
Boele FW, Verdonck-de Leeuw IM, Cuijpers P, Reijneveld JC, Heimans JJ, Klein M (2018) Internet-based guided self-help for glioma patients with depressive symptoms: a randomized controlled trial. J Neuro-Oncol 137:191–203
Sijercic I, Ennis N, Monson CM (2019) A systematic review of cognitive and behavioral treatments for individuals with psoriasis. J Dermatol Treat:1–8
Shaw B, McTavish F, Hawkins R, Gustafson D, Pingree S (2000) Experiences of women with breast cancer: exchanging social support over the CHESS computer network. J Health Commun 5:135–159
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928
Willems R, Mesters I, Lechner L, Kanera I, Bolman C (2017) Long-term effectiveness and moderators of a web-based tailored intervention for cancer survivors on social and emotional functioning, depression, and fatigue: randomized controlled trial. J Cancer Surviv 11:691–703
Ellert U, Lampert T, Ravens-Sieberer U (2005) Messung der gesundheitsbezogenen Lebensqualität mit dem SF-8. Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz 58:1330–1337
Aaronson NK, Muller M, Cohen PDA, Essink-Bot M-L, Fekkes M, Sanderman R, Sprangers MAG, te Velde A, Verrips E (1998) Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J Clin Epidemiol 51:1055–1068
Webster K, Cella D, Yost K (2003) The Functional Assessment of Chronic Illness Therapy (FACIT) measurement system: properties, applications, and interpretation. Health Qual Life Outcomes 1:79
Derogatis LR, Melisaratos N (1983) The Brief symptom inventory: an introductory report. Psychol Med 13:595–605
Tuinman MA, Gazendam-Donofrio SM, Hoekstra-Weebers JE (2008) Screening and referral for psychosocial distress in oncologic practice: use of the Distress. Thermometer Cancer 113:870–878
Zigmond AS, Snaith RP (1983) The hospital anxiety and depression scale. Acta Psychiatr Scand 67:361–370
Arindell WA, Ettema J (2003) Handleiding bij een multidimensionele psychopathologie-indicator: Symptom Checklist SCL-90. (Herziene uitgave). Swets & Zeitlinger, Lisse
Bruggeman-Everts FZ, Wolvers MDJ (2017) Effectiveness of two web-based interventions for chronic cancer-related fatigue compared to an active control condition: results of the “Fitter na kanker” randomized controlled trial. J Med Internet Res 19:e336
Zhao D, Lustria MLA, Hendrickse J (2017) Systematic review of the information and communication technology features of web- and mobile-based psychoeducational interventions for depression. Patient Educ Couns 100:1049–1072
Zhu J, Ebert L, Chan WC (2017) Integrative review on the effectiveness of Internet-based interactive programs for women with breast cancer undergoing treatment. Oncol Nurs Forum 44:E42
Bártolo A, Pacheco E, Rodrigues F, Pereira A, Monteiro S, Santos IM (2017) Effectiveness of psycho-educational interventions with telecommunication technologies on emotional distress and quality of life of adult cancer patients: a systematic review. Disabil Rehabil 41:870–878
Corbett T, Singh K, Payne L, Bradbury K, Foster C, Watson E, Richardson A, Little P, Yardley L (2017) Understanding acceptability of and engagement with web-based interventions aiming to improve quality of life in cancer survivors-a synthesis of current research. Psychooncology 27:22–33
Lleras de Frutos M, Casellas-Grau A, Sumalla EC, de Gracia M, Borras JM, Ochoa Arnedo C (2019) A systematic and comprehensive review of internet use in cancer patients: psychological factors. Psychooncology 29:1–17
Klemm P (2012) Effects of online support group format (moderated vs peer-led) on depressive symptoms and extent of participation in women with breast cancer. Comput Inform Nurs 30:9–18
Rice RE (2006) Influences, usage, and outcomes of Internet health information searching: multivariate results from the Pew surveys. Int J Med Inform 75:8–28
Melville KM, Casey LM, Kavanagh DJ (2009) Dropout from Internet-based treatment for psychological disorders. Br J Clin Psychol 49:455–471
Aboujaoude E, Salame W, Naim L (2015) Telemental health: a status update. World Psychiatry 14:223–230
Schweier R, Romppel M, Richter C, Grande G (2016) Dissemination strategies and adherence predictors for web-based interventions-how efficient are patient education sessions and email reminders? Health Educ Res 31:384–394
Acknowledgments
The authors thank the librarian Feng-Zhen Guan for her contribution in the search strategy and Hai-Yan Guo for her kind assistance in the revision of the English language in this manuscript.
Funding
This study was supported by the Scientific Research Talents Training Project from Fujian Province Health Commission, China (Grant No. 2018-ZQN-63), and Fujian Provincial Nature Science (Grant No. 2019J01684).
Author information
Authors and Affiliations
Contributions
Ying Wang and Yazhu Lin contributed equally to this work. Rong Hu was responsible for the study conception and design. Ying Wang and Yazhu Lin contributed to data acquisition, analysis, and interpretation. Ying Wang was responsible for manuscript preparation. Rong Hu and Yong Wu contributed to the critical revision of the manuscript, obtained funding, and supervised the research. Jingyi Chen and Chunfeng Wang contributed to the review of the data and manuscript. All authors approved the final manuscript and have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOC 39 kb)
Rights and permissions
About this article

Cite this article
Wang, Y., Lin, Y., Chen, J. et al. Effects of Internet-based psycho-educational interventions on mental health and quality of life among cancer patients: a systematic review and meta-analysis. Support Care Cancer 28, 2541–2552 (2020). https://doi.org/10.1007/s00520-020-05383-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-020-05383-3