
Abstract
Objective
In addition to question prompts for information transfer, we also used prompts to facilitate the expression of emotions. Our aim was to investigate how a question prompt list (QPL) is accepted by patients and whether it enhances interactional empowerment of the patients in the consultation with the radio-oncological treatment team before the beginning of radiotherapy.
Methodology
Adult cancer patients before the beginning of radiotherapy were randomly assigned to the intervention group (IG) or control group (CG). The patients in the IG received a QPL with predefined subsets and subject areas. After the physician’s consultation, both groups completed a self-developed, content validated questionnaire on interactional empowerment. The IG evaluated the QPL using a self-developed instrument.
Result
A total of 279 adult cancer patients participated in the study (IG n = 139/CG n = 140). The participants of the IG reported a significantly higher interactional empowerment compared with those of the CG (t(277) = − 2.71, p = .007, 95% CI [− 1.61, − 0.26], d = 0.29). 60.4% of the IG agreed “rather” or “very” that they used the QPL in consultation with the medical team.
Conclusion
The QPL used in the consultation improved the self-assessed competence for interaction with the medical team and strengthened the interactional empowerment. The QPL was well accepted by the patients and is to be introduced into a routine as a practicable and simple instrument in the future. The support of patients in addressing concerns and fears is an important innovation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Patients in radiation oncology are exposed to particular stress and treatment burdens. The term “radiotherapy” can cause frightening associations (atomic bomb, general carcinogenic effect of radiation) [1, 2]. Patients often report a need for information which is only unsatisfactorily met by the treatment team [3, 4]. Patients’ information needs are usually highest at the time of treatment planning and before the start of the treatment [5]. Physicians tend to underestimate the patients’ need for information [6] and in addition, patients with life-threatening diseases often feel unable to ask questions [7]. A higher level of information among patients is associated with a higher health-related quality of life and higher empowerment [6, 8] as well as lower psychological stress such as depression and anxiety [9, 10]. Empowerment is a construct that varies according to the persons, contexts, and time involved, and is important in cancer research [11]. In relation to health care, empowerment can describe how people see themselves and assess their ability to deal with the disease (intrapersonal), how they understand and interact with the health system (interactional), and what behaviors they learn and use to experience control (behavioral) [11].
One possible way to increase the level of information and thus empowerment is to use “Question prompt lists” (QPLs). QPLs are a patient-oriented, activating approach that can be used to strengthen the informedness of patients, for example, with regard to illness and treatment [12]. Patients with cancer are thus encouraged to ask questions to the physician [13] to satisfy their information needs or reduce their information deficits [14]. QPLs are assessed by patients as useful and helpful [15], by practitioners as positive and not interfering routine procedures [16]. Even if questions like “What is my prognosis?” or “What side effects may I notice?” implicitly express the feelings of the patient, QPLs are primarily aimed at the transmission of cognitive information. In addition to health-related information, patients also need emotional support from their medical team [17]. Therefore, in this study, implicit question prompts (iQP) were used along with prompts explicitly aimed at addressing the expression of emotions, such as “I am worried about the side effects. How can you help me?” We call these kinds of prompts explicit question prompts (eQP). According to our state of knowledge, this is an innovation within QPL research and combines the activating approach of QPLs with emotional support of the patients on the part of the medical team. Patients who participate more actively in discussions with the medical team are more satisfied with their health care and receive more patient-oriented care [18]. Due to the many and varied strains on patients during radiation therapy, it is essential to establish a trustworthy doctor-patient relationship right from the first medical consultation to take all concerns into account and ask as many questions as necessary. The expression of concerns and needs is also related to a trusting and constructive relationship with the treatment team and the experience of self-efficacy. This is well described by the construct “interactional empowerment,” [19] i.e., how the patient understands and can work with the healthcare system [11]. In this study, we examined in a randomized controlled and regarding physicians single-blinded trial whether the application of this QPL contributed to a higher degree of interactional empowerment of the patients than no QPL and how the patients who used it assessed the QPL. Although QPLs are more effective when the physician proactively supports using QPLs [20], the goal of the study was to investigate the effects of this kind of QPL without modifications of the physicians, so that regular debriefing of physicians can be avoided.
Methods
Participants
Participants of the study were adult cancer patients > 18 years who were treated in the Department of Radiation Oncology, University Hospital Wuerzburg because of their malignant cancer in curative or palliative therapy intention. They were recruited in the waiting period before the initial consultation with the radiation oncologist. Exclusion criteria were insufficient knowledge of German and cognitive impairment or lack of consent.
Design and procedure
We used a prospective randomized controlled trial with one intervention group (IG) and one control group (CG). At the first consultation in the Department of Radiation Oncology, University Hospital Wuerzburg, patients routinely reported in the waiting time about their comorbidities, their medications, and the nutritional status. Patient-reported symptoms, psychosocial distress, and information needs were assessed using the palliative care outcome scale (iPOS) [21] and the distress thermometer [22] in a paper-pencil version. Participants were recruited consecutively. All patients meeting the inclusion criteria and providing informed consent were randomly assigned to the IG or CG at the time of their approval. The randomization list (with computer-generated random numbers) was created by the Department of Radiation Oncology, Interdisciplinary Centre for Palliative Medicine, University Hospital Wuerzburg. The IG received a written QPL in preparation for the first contact with the radiation oncologist right before entering the waiting room. The CG received treatment as usual. After this first consultation, both groups completed a questionnaire to assess interactional empowerment. At the measurement point, the IG was also asked to evaluate comprehensibility, usefulness, and applicability of the QPL. The IG also had the opportunity to comment on the QPL. The Ethics Commission of the University of Wuerzburg has approved the study in advance (59/18-sc).
Question prompt list
The QPL, which the IG received, contained predefined sentences and topics, which have been asked for in the routine screening questionnaire, such as physical complaints, need for information on support and palliative care. Patients in the IG were encouraged to use the QPL to prepare for the consultation with the radiation oncologist. They could supplement the predefined sentences on the QPL with individually relevant topics. The predefined sentences aimed at the one hand at cognitive information transfer and implicit expression of emotions (iQP), like “Which offers are there to...” or “What can you tell me about...” On the other hand, sentences such as “I care about...” and “I feel depressed because of ...” were supposed to improve the explicit expression of emotions (eQP).
Questionnaires
Interactional empowerment questionnaire
Various questionnaires were established for measuring empowerment in cancer research [23,24,25]. Since empowerment seems to be person, time, and context dependent, and suitable measurement instruments for the oncological context of interactional empowerment are not yet available, a questionnaire validated by cognitive interviews was used for the study. The self-developed interactional empowerment questionnaire (iE-Q) was based on the questionnaires Patient Satisfaction Questionnaire (PSQ) [26], EORTC QLQ INFO [27], and the subscales “health service” and “skills” of the health education impact questionnaire (heiQ) [24]. The iE-Q assesses interactional empowerment of oncological patients after consultation with the radiotherapist, i.e., how the patient understands the medical team after the initial consultation and how he or she can work with it. Content validity of the items was investigated using cognitive interviews with 15 oncological patients. The questionnaire consisted of eight items (see Table 2). All items had a four-level response scale (0 not at all, 1 little, 2 quite, 3 very much). The responses were added to a sum score with a range of 0–24, with higher values indicating higher interactional empowerment.
Information needs
Information needs of the patients were recorded with the question “Would you have liked to receive more / less information?” with dichotomous response options (yes/no) [27].
Evaluation of QPL
The assessment of the QPL included questions on the application of QPL in the radiation oncologists’ consultation and its comprehensibility and usefulness. The QPLs were evaluated on a five-level scale (0 not at all, 1 rather not, 2 partially,3 rather yes, 4 yes very much). Textual answers for improvement suggestions and comments were also possible.
Sociodemographic and clinical data
In addition, sociodemographic data such as age, gender, nationality, and level of education were recorded. Patients also indicated the type of cancer and previous therapies.
Statistical analyses
Data were analyzed using Statistical Package for the Social Sciences version 25 (SPSS Inc., Chicago, Illinois). For the descriptive analyses iE-Q, classified into IG and CG, evaluation sheet for IG and sociodemographic data were evaluated descriptively and reported as (absolute) percentages. The statistical analysis was subsequently performed with the Welch t test for independent samples with given normal distribution and adjustments for variance heterogeneity. The statistical significance level for the primary outcome (sum score iE-Q) has been set at α = 0.05. The statistical significance level within the explorative analysis of the sum score of the individual questions (8 items) between IG and CG was adjusted to the number of tests using Bonferroni-Holm adjustment. This resulted in the significance level α = 0.05/(9—rank number of pair) a value between 0.0056–0.05, depending on degree of significance.
Results
Participant flow and assignment
From June to October 2018, 360 participants met the inclusion criteria. Informed consent was given by 313 patients, of which 156 were randomized to the IG and 157 to the CG. A total of 12 of the IG and 8 of the CG members did not participate in the follow-up interview after the physician’s consultation. A total of 14 had to be excluded because of cognitive impairments or no malignant cancer. Since less than 5% of the questionnaires contained missing data and these did not differ significantly from the completed questionnaires in terms of gender, age, cancer identity, or duration of treatment, these data were excluded [28] (see Fig. 1 for more details). Within the study period, 15 radiotherapists worked in the Department of Radiation Oncology.

CONSORT flow diagram
Demographics and clinical characteristics
A total of 279 patients were included in the study (140 KG, 139 IG). Participants’ age ranged from 25 to 95 (M = 64.9, SD = 11.9); 46.2% were women; 97.5% had German nationality; 50% had a primary or lower secondary school educational level. The participants in the study were predominantly affected by breast cancer (23.7%) or prostate cancer (21.9%) (see Table 1 for more details).
Interactional empowerment (iE-Q)
The mean of the sum score differed significantly at the significance level of α = .05 between the IG (M = 21.7, SE = .22, SD = 2.65) and the CG (mean = 20.8, SE = .26; SD = 3.08) (t(277) = − 2.71, p = .007, 95% CI [− 1.61, − 0.26]) with a small effect size d = .29 (r = 0.16) (see Fig. 2).

Sum-score of iE-Q (range 0–24) in IG and CG. (mean and standard deviation)
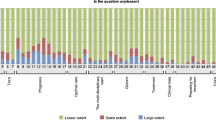
On an item basis, in the IG, 83.5% of patients (CG 67.1%) agreed “very much” that they were able to discuss all their problems with the physician. Likewise, 74.1% of the IG (CG 56.4%) felt it was easy to tell the treatment team if and what was depressing them. There was hardly any difference in the question of how self-confident the patients were providing information to the medical team (“very much” IG 71.2% vs. CG 66.4%). 87.1% of the IG and 71.4% of the CG agreed “very much” that they were able to talk openly with the medical team about their health problems. When asked about good and cooperative cooperation with the treatment team, 80.6% of the IG patients (CG 66.4%) agreed “very much.” 51.8% of the IG (CG 47.1%) agreed “very much” about knowing to deal with their health problems after consultation. The groups did not differ substantially in satisfaction with the amount of information given (“very satisfied” 68.3% IG vs. 65% CG). Also, 74.1% of the IG and 66.4% of the CG found the given information “very” helpful. A more detailed description of the items can be found in Fig. 3.

Description of the answer categories across all questions divided into IG and CG
The results of the explorative t tests of the individual items of the questionnaire can be found in Table 2.
No significant differences are found in the single question “Would you have liked to receive more / less information” between the two groups. In both groups, 15 patients reported that they wanted more information.
Acceptance of the question prompt list in IG
60.4% of patients with QPL (IG) used it “frequently” or “mostly.” Only 15% used them “not at all” or “rather not.” 79% of the IG rated the QPL as “very” or “rather” comprehensible and 55% as “very” or “rather” helpful (see Table 3 for more details).
In the textual answers, six participants named the listing of different subject areas as helpful, as important topics were recalled and new relevant topics were described. Three of the participants had prepared themselves in advance of the radiation oncologist’s consultation with their own question lists—therefore they would have preferred to be offered the QPL at an earlier point. The wish for a more specific question for radiation therapy was mentioned once.
Discussion
The study supports the assumption that QPLs can improve interactional empowerment, i.e., perceived interaction with the medical team. We examined a simple, feasible intervention designed to increase the interactional empowerment of cancer patients in radio-oncology. Also, this was one of the first studies with QPL that, in addition to providing information, also focused on the explicit expression of emotions. Our study showed that this QPL was well accepted by the patients and that it improved subjective interactional empowerment. There was a significant difference with small effect size between the patient group with and without QPL. The offered QPL was used by the majority of the IG and was evaluated as understandable and helpful, as has been shown in other studies [15]. According to the results of the study, the QPL promoted a cooperative relationship with the medical team.
Adequate information about the patients and shared decision-making is getting more and more important in oncology [29]. QPLs can help to meet the information needs [14] and to reduce psychological distress [30]. But in addition to sufficient information, the communication between physicians and patients is also essential in radiotherapy [31]. Not only the communication skills but also an appreciative and respectful attitude is required by the medical team to build a constructive relationship [31]. When looking at the single items, the IG showed significantly higher values than the CG for four of the eight items. These four items were more focused on the emotional aspects, e.g., addressing (health) problems and worries and especially cooperative cooperation with the medical team than the other four items, which focused more on information and knowledge.
QPLs support oncological patients in addressing their problems and concerns with their physicians. Compared with other studies [12], the type of QPL used in this study is a great innovation. Patients were not given entirely predefined sentences, as is usual with QPLs [32]. The partial sentences and/or questions and subject areas, which are often of interest to oncological patients, were intended to encourage patients to ask individualized, specific, and important questions. The routine screening reminded patients of possible topics that they also found in the QPL’s list of topics. In this way, patients could determine their information needs independently, systematically, and promptly. In addition, the QPL was designed to enable patients to address their own concerns and emotions. This should help the patients not only to stay with the formal aspects, i.e., treatment duration, but also to be able to deal with the emotional aspects with the treatment team [17].
The use of a QPL with additional prompts for expressing emotions and concerns might cause the difference between IG and CG for items that comprise emotional topics. It would be interesting to know which type of QPLs, implicit or explicit, has a stronger effect or whether it is important for the two to interact. A follow-up study in which the efficacy of QPLs with and without prompts for the expression of emotions and concerns is examined could answer this question more precisely. In order to be able to develop an effective intervention that fits as closely as possible and can support the patient in his needs and worries, the focus should increasingly be on comparing different methods, for example, question prompt list vs. question sheet, [33] or QPL with and without emotion prompts.
The study involved cancer patients who were about to receive radiotherapy. At the beginning of radiotherapy, patients need sufficient information to be able to make the right decisions for them together with the physician [4]. The benefits and risks of the treatment must be weighed individually so that there is no over- or under-treatment. Well-informed patients are better able to deal with their individual problems with sufficient motivation and realistic expectations and to participate in decisions that are relevant for further treatment [10]. However, physicians rarely talk about the risks of treatment [34] and healthcare professionals are usually reluctant to share all important information about cancer and its treatment, which often limits the ability to obtain necessary information [35]. In addition, the first consultation usually takes place with a previously unknown radiation oncologist that justifies the need to invest in a trustful relationship since good cooperation is essential for further treatment planning. In the decision-making process, patients want to be perceived with their individual concerns and worries on the one hand, and on the other hand, the specialist knowledge of the physician and his recommendations are taken into account [29]. To build this bridge, the use of a QPL with additional prompts for the expression of concerns and emotions makes sense in cancer treatment, especially at the beginning of treatment. However, an improvement of the interaction only on the side of the patients can have only a limited effect. Various studies suggest that oncological physicians still have problems with joint decision-making [36, 37]. This aspect must be taken into account and verified in further studies with active training of communication skills for medical professionals [33].
QPLs are currently relatively general in design so that every cancer patient can use them. It may be helpful to design the QPLs needs-oriented, e.g., according to tumor entities [38] or therapy intentions (palliative vs. curative). Moreover, it would be important to transfer QPLs for cultural and special needs groups and to figure out the optimal length of QPLs [39]. Further research should focus on the effects of prompts to foster the expression of emotional disclosure and how this can be better integrated into everyday hospital life despite limited resources.
Limitations
This study had several limitations. It examined “interactional empowerment.” Since empowerment is a multifaceted construct and seems to be dependent on context and persons, a questionnaire was designed for this purpose. Cognitive interviews in a group of oncological patients were held to examine content validity, but a construct- or criterion-related validity for this questionnaire was not known.
Furthermore, we only collected subjective data of the patients. Data that can be objectified, such as how many questions they asked during the interview or whether they bring up any emotional statements, are to be recorded in follow-up studies.
Since iQP and eQP were used simultaneously in the IG, the improvement in empowerment cannot be attributed to the use of one of these QPLs. In further studies, efficacy and the difference between iQP and eQP will be further investigated.
In addition, the QPL was only tested on patients prior to radiation treatment. Other results may be obtained with a QPL in patients prior to chemotherapy, surgery, or other oncological treatment. Due to the monocentric orientation of the study, the generalizability of the results may be limited. No data were collected from doctors or informal or family caregivers. Studies using the QPL should be conducted in other settings and with other patient groups. Moreover, it could be interesting to test the contribution of QPL interactional empowerment to different outcomes such as understanding of prognosis, shared decision-making, or quality of life.
Though the QPL was evaluated positively in our study immediately after the consultation with the physician, long-term effects of the QPL are not yet established. Future studies should examine whether patients’ information or their handling of cancer differ in the long term between those who used QPL and those who did not.
Moreover, due to the lack of an active control group or placebo group, it could not be excluded that the positive effects of QPL referred to non-specific factors such as the attention of the investigator or the sympathy of the investigator. The extent of this possible bias was unknown and difficult to estimate. Nevertheless, the study was formal single-blind concerning the physicians, so that this aspect has as little influence as possible on the evaluation of the QPL. Even if the physicians did not know which patients received QPL during the waiting period and also did not get a direct request to proactively respond to QPL [20], it remained unclear to what extent blinding was actually ensured, as no data were collected during the physician-patient consultation.
Conclusion and implications
Since the study supports the assumption that QPL can also improve the interactional performance of patients, iQP and eQP are to be introduced into the routine of radiotherapy. Therapy experience or the age of the patients should be included in further evaluations of the efficacy of QPL as possible moderators in the calculations. Besides, it would be advisable to use this QPL as early as possible at the beginning of cancer treatment to avoid a lack of information and dissatisfaction. In addition, for a more intensive, longer preparation time for the physician’s consultation before the radiation, it may also be helpful to send the patients a list with QPL before the first appointment. In this way, the patient can prepare himself at home for the physician’s consultation and then ask individual questions. There is some evidence that timely and comprehensive information about cancer and treatment options reduces psychological stress in patients [30].
References
Halkett GKB, Kristjanson LJ, Lobb EA (2008) If we get too close to your bones they’ll go brittle. Psycho-Oncol 17(9):877–884
Guidolin K, Lock M, Brackstone M (2017) Patient-perceived barriers to radiation therapy for breast cancer. Can J Surg 61(1):15716
Harrison JD, Young JM, Price MA, Butow PN, Solomon MJ (2009) What are the unmet supportive care needs of people with cancer? A systematic review. Supportiv Care Cancer 17(8):1117–1128
Wang S-Y, Kelly G, Gross C, Killelea BK, Mougalian S, Presley C, Fraenkel L, Evans SB (2017) Information needs of older women with early-stage breast cancer when making radiation therapy decisions. Int J Radiat Oncol 98(4):733–740
Halkett GKB, Kristjanson LJ, Lobb EA et al (2010) Meeting breast cancer patients’ information needs during radiotherapy. Eur J Cancer Care 19(4):538–547
Kinnersley P, Edwards A, Hood K et al (2008) Interventions before consultations for helping patients address their information needs. BMJ 3
Jefford M, Tattersall MHN (2002) Informing and involving cancer patients in their own care. The Lancet Oncology 3(10):629–637
Groen WG, Kuijpers W, Oldenburg HS et al (2015) Empowerment of cancer survivors through information technology. J Med Internet Res 17(11):e270–e270. https://doi.org/10.2196/jmir.4818
Fröjd C, Lampic C, Larsson G, Essen L (2009) Is satisfaction with doctors’ care related to health-related quality of life, anxiety and depression among patients with carcinoid tumours? A longitudinal report. Scand J Caring Sci 23(1):107–116. https://doi.org/10.1111/j.1471-6712.2008.00596.x
Vogel BA, Leonhart R, Helmes AW (2009) Communication matters. Patient Educ Couns 77(3):391–397
Eskildsen NB, Joergensen CR, Thomsen TG, Ross L, Dietz SM, Groenvold M, Johnsen AT (2017) Patient empowerment. Acta Oncol 56(2):156–165
Dimoska A, Butow PN, Lynch J, Hovey E, Agar M, Beale P, Tattersall MHN (2012) Implementing patient question-prompt lists into routine cancer care. Patient Educ Couns 86(2):252–258
Rodenbach RA, Brandes K, Fiscella K, Kravitz RL, Butow PN, Walczak A, Duberstein PR, Sullivan P, Hoh B, Xing G, Plumb S, Epstein RM (2017) Promoting end-of-life discussions in advanced cancer. J Clin Oncol 35(8):842–851
Smith SK, Trevena L, Simpson JM, Barratt A, Nutbeam D, McCaffery KJ (2010) A decision aid to support informed choices about bowel cancer screening among adults with low education. BMJ 341:c5370
Brandes K, Butow PN, Tattersall MHN, Clayton JM, Davidson PM, Young J, Epstein RM, Walczak A (2014) Advanced cancer patients’ and caregivers’ use of a Question Prompt List. Patient Educ Couns 97(1):30–37
Spiegle G, Al-Sukhni E, Schmocker S et al (2013) Patient decision aids for cancer treatment. Cancer 119(1):189–200
Bensing J, Verhaak PFM (eds) (2004) Chapter 11: communication in medical encounters. Health Psychology. Blackwell Publishing, Oxford
Street RL Jr, Millay B (2001) Analyzing patient participation in medical encounters. Health Commun 13(1):61–73
Zimmerman MA (1995) Psychological empowerment. Am J Commun Psychol 23(5):581–599
Brown RF, Butow PN, Dunn SM, Tattersall MHN (2001) Promoting patient participation and shortening cancer consultations. Brit J Cancer 85(9):1273–1279
Bausewein C, Fegg M, Radbruch L, Nauck F, von Mackensen S, Borasio GD, Higginson IJ (2005) Validation and clinical application of the german version of the palliative care outcome scale. J Pain Symptom Manag 30(1):51–62
National Comprehensive Cancer Network (NCCN) (2003) Distress management clinical practice guidelines. J Natl Compr Canc Netw 1:344–374
Maunsell E, Lauzier S, Brunet J, Pelletier S, Osborne RH, Campbell HS (2014) Health-related empowerment in cancer. Cancer 120(20):3228–3236
Schuler M, Musekamp G, Faller H et al (2013) Assessment of proximal outcomes of self-management programs: translation and psychometric evaluationof a German ersion of the health education impact questionnaire (heiQ). Qual Life Res 22:1391–1403
van den Berg SW, van Amstel FKP, Ottevanger PB, Gielissen MFM, Prins JB (2013) The cancer empowerment questionnaire. J Psychosoc Oncol 31(5):565–583
Langewitz W, Keller A, Denz M et al (1995) The Patient Satisfaction Questionnaire. Psychother Med Psych 45(9–10):351–357
Arraras JI, Greimel E, Sezer O, Chie WC, Bergenmar M, Costantini A, Young T, Vlasic KK, Velikova G (2010) An international validation study of the EORTC QLQ-INFO25 questionnaire. Eur J Cancer 46(15):2726–2738
Jakobsen JC, Gluud C, Wetterslev J, Winkel P (2017) When and how should multiple imputation be used for handling missing data in randomised clinical trials – a practical guide with flowcharts. BMC Med Res Methodol 17(1):162
Tamirisa NP, Goodwin JS, Kandalam A, Linder SK, Weller S, Turrubiate S, Silva C, Riall TS (2017) Patient and physician views of shared decision making in cancer. Health Exp 20(6):1248–1253
Schofield PE, Butow PN, Thompson JF et al (2003) Psychological responses of patients receiving a diagnosis of cancer. Ann Oncol 14:48–56
Llewellyn A, Howard C, McCabe C (2019) An exploration of the experiences of women treated with radiotherapy for breast cancer. Eur J Oncol Nurs 39:47–54
Shepherd HL, Barratt A, Trevena LJ, McGeechan K, Carey K, Epstein RM, Butow PN, del Mar CB, Entwistle V, Tattersall MHN (2011) Three questions that patients can ask to improve the quality of information physicians give about treatment options. Patient Educ Couns 84(3):379–385
Bottacini A, Goss C, Mazzi MA, Ghilardi A, Buizza C, Molino A, Fiorio E, Nortilli R, Amoroso V, Vassalli L, Brown RF (2017) The involvement of early stage breast cancer patients during oncology consultations in Italy. BMJ Open 7(8):e015079
Janz NK, Li Y, Zikmund-Fisher BJ, Jagsi R, Kurian AW, An LC, McLeod MC, Lee KL, Katz SJ, Hawley ST (2017) The impact of doctor–patient communication on patients’ perceptions of their risk of breast cancer recurrence. Breast Cancer Res Tr 161(3):525–535
Prip A, Møller KA, Nielsen DL, Jarden M, Olsen MH, Danielsen AK (2018) The patient–healthcare professional relationship and communication in the oncology outpatient setting. Cancer Nurs 41(5):E11–E22
Müller E, Hahlweg P, Scholl I (2016) What do stakeholders need to implement shared decision making in routine cancer care? A qualitative needs assessment. Acta Oncol 55(12):1484–1491
Kunneman M, Engelhardt EG, ten Hove FLL et al (2016) Deciding about (neo-)adjuvant rectal and breast cancer treatment. Acta Oncol 55(2):134–139
Ahamad A, Wallner P, Salenius S et al (2019) Information needs expressed during patient-oriented oncology consultations. J Canc Educ 34(3):488–497. https://doi.org/10.1007/s13187-018-1329-5
Sansoni JE, Grootemaat P, Duncan C (2015) Question. Prompt Lists Health Consult 98(12):1454–1464
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Zetzl, Mann, and Gruner report grants from Deutsche Krebshilfe, during conduct of the study. Schuler, Jentschke, Neuderth, Roch, and Oorschot have nothing to disclose.
Disclaimer
The design, conduct, data collection, analysis, and interpretation of the results were performed independently of the funders. The funders played no role in the review or approval of this manuscript.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zetzl, T., Mann, D., Gruner, S. et al. Question prompts to empower cancer patients: results of a randomized controlled trial. Support Care Cancer 28, 2571–2579 (2020). https://doi.org/10.1007/s00520-019-05036-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-019-05036-0