
Abstract
Purpose
The aim of this study was to determine the relationship between the time to antibiotic administration and patients’ outcomes of febrile neutropenia (FN). We also investigated the relationship between the time to antibiotics and mortality rates in a subgroup of patients with bacteremia or severe sepsis or septic shock.
Methods
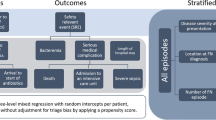
From the Neutropenic Fever Registry, we analyzed 1001 consecutive FN episodes diagnosed from November 1, 2011, to August 31, 2014. Timing cutoffs for antibiotics included the following: ≤1 vs. >1 h, ≤2 vs. >2 h, ≤3 vs. >3 h, and ≤4 vs. >4 h. Multivariate logistic regression was used to adjust for potential confounders in the association between timing intervals and outcomes of FN episodes.
Results
The median length of time from triage to antibiotics was 140 min (interquartile range, 110–180 min). At each time cutoff, the time from triage to antibiotic administration was not significantly associated with FN outcomes after adjusting for potential confounders. Antibiotic timing was not significantly associated with complication rates in overall FN episodes. We failed to find a significant relationship between antibiotic timing and mortality in FN episodes with severe sepsis or septic shock or with bacteremia. Procalcitonin concentration and the Multinational Association for Supportive Care in Cancer (MASCC) risk index score were found to be more crucial determinants of outcomes in patients with FN.
Conclusions
The time to antibiotic administration is not a major factor in FN outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Neutropenia is a major toxic effect of chemotherapeutic agents that predisposes cancer patients to serious infections [1]. The aim of initial empirical antibiotic therapy in patients with febrile neutropenia (FN) is to prevent serious morbidity and mortality associated with bacterial pathogens. Because infection can rapidly progress and become life threatening in this group of patients, clinical practice guidelines recommend administration of broad-spectrum antibiotics as soon as possible after fever is documented, ideally within an hour [1–3]. However, there are limited data on the time to antibiotic administration and its impact on outcomes in patients with FN [4, 5]. This recommendation is primarily based on expert opinion and evidence from studies of diverse patients with severe sepsis or septic shock [6–8].
The Surviving Sepsis Campaign Guidelines recommend intravenous antibiotic administration within the first hour after recognition of severe sepsis [8]. Through various studies, timely and appropriate antibiotic administration, along with early goal-directed therapy, has been shown to decrease mortality in patients with severe sepsis or septic shock [7, 9]. However, because most patients who develop fever during neutropenia have no identifiable site of infection, including negative blood culture results, and usually have favorable outcomes, evidence obtained from distinct groups of patients with severe sepsis or septic shock might not be applicable to patients with FN.
The aim of this study was to determine the relationship between the time to antibiotics and outcomes of FN in cancer patients. We also studied the relationship between the time to antibiotics and mortality rates in subgroups of patients with bacteremia or with severe sepsis or septic shock.
Methods
Asan Medical Center has an annual emergency department (ED) volume of approximately 106,000 patients and serves as a tertiary referral center in Seoul, Korea. Since November 2011, all adult cancer patients diagnosed with chemotherapy-induced FN in the ED of Asan Medical Center were enrolled with their data prospectively collected in the Neutropenic Fever Registry. Patients who had been managed at other hospitals for FN and subsequently transferred to our ED were not included in the registry. At the time of the ED visit, data, including underlying cancer, presence of distant metastasis, vital signs, and laboratory results, were collected. Along with other clinical variables, timing of antibiotics, defined as the time from triage to the first dose of parenteral antibiotic administration (in minutes), and the Multinational Association of Supportive Care in Cancer (MASCC) risk index scores are routinely calculated [10]. From the registry, we analyzed 1001 consecutive FN episodes diagnosed from November 1, 2011, to August 31, 2014.
FN was defined as a temperature of ≥38 °C using a tympanic thermometer and a neutrophil count of <500 cells/mm3 or a count of <1000 cells/mm3 with a predicted decrease to <500 cells/mm3 [11]. Bacteremia was defined as a blood culture growing an organism determined not to be a contaminant from peripheral blood or from a central venous indwelling catheter if present. After the FN was diagnosed, all patients were administered parenteral antibiotics including extended-spectrum penicillin/β-lactamase inhibitor (piperacillin/tazobactam), fourth-generation cephalosporin (cefepime), cefazolin/ceftazidime combination, or imipenem/cilastatin. Outcomes were categorized as unfavorable if serious medical complications, including death, occurred. Complications included refractory hypotension, respiratory failure, intensive care unit admission, disseminated intravascular coagulation, altered mental status, congestive heart failure, electrocardiogram changes requiring anti-arrhythmic treatment, renal failure requiring renal replacement therapy, and other complications considered serious and clinically significant by the investigator. This definition of outcome was adapted from the study of Klastersky et al., from which the MASCC risk score index was derived [12].
Descriptive data are presented as mean ± standard deviation (SD) or median (interquartile range [IQR]) for continuous variables and frequencies with percentages for categorical variables. Timing cutoffs for antibiotics included the following: ≤1 vs. >1, ≤2 vs. >2, ≤3 vs. >3, and ≤4 vs. >4 h. With each cutoff, multivariable logistic regression analyses were separately performed to adjust for potential confounding in the association between timing intervals and episode outcomes. We considered the MASCC risk-index score, serum C-reactive protein and procalcitonin levels, Eastern Cooperative Oncology Group (ECOG) performance score, and days passed since the last chemotherapy as potential confounders [13–15]. These potential confounding factors were determined a priori, forced into the final model along with the antibiotic timing at each timing cutoff, and adjusted odds ratios (ORs) with 95 % confidence intervals (CIs) for the outcomes were presented. Statistical significance was defined as P < 0.05. All statistical analyses were performed with SPSS (version 20.0; SPSS Inc., Chicago, IL). This study was approved by the institutional review board of our hospital.
Results
In total, 1001 episodes of FN in 863 patients were analyzed in this study. The average age of the patients was 54.3 ± 13.9, with 34.5 % males. Regarding underlying malignancies, 785 (78.4 %) had solid tumors and 216 (21.6 %) had hematologic malignancies. Breast and lung cancers were the most frequent solid tumors, being involved in 380 (38.0 %) and 95 (9.5 %), respectively, of FN episodes. Lymphoma was the most common hematologic malignancy, accounting for 194 (19.4 %). Distant metastases were present in 45.4 %. Prophylactic antibiotics and prophylactic granulocyte colony-stimulating factor were administered in 202 (20.2 %) and 90 (9.0 %) episodes, respectively. The average time to when patients presented to the ED from the last day of chemotherapy was 10.8 ± 3.2 days. Of 1001 episodes, 899 (89.8 %) were in the MASCC low-risk group and 102 (10.2 %) were in the high-risk group. The median length of time from triage to antibiotics was 140 min (IQR, 110–180 min) (Table 1). Piperacillin/tazobactam (76.2 %) was the most common empirical antibiotic used, followed by piperacillin/tazobactam plus levofloxacin (8.1 %), cefepime (7.9 %), and cefazolin/ceftazidime combination (4.7 %). Vancomycin was added to piperacillin/tazobactam in 2.4 %, and imipenem/cilastatin was used in 0.7 % of cases as initial antibiotics.
A known source of infection was identified in 331 episodes (33.1 %), including 122 (12.2 %) microbiologically documented infections and 209 (20.9 %) clinically documented infections (Table 2). Twenty-eight (2.8 %) episodes had bacteremias without an identifiable source. Unfavorable outcomes with complications developed in 174 (17.4 %), including 23 deaths. In addition, 64 patients (6.4 %) had positive blood cultures and 67 (67 %) had severe sepsis or septic shock during their stay in the ED.
At every time cutoff, we could not find a statistically significant relationship between the time from triage to the administration of antibiotics and the outcomes of FN after adjusting for potential confounders. Antibiotic timing was not significantly associated with complication rates in overall FN episodes (0–1 h, 31.4 %; 1–2 h, 15.4 %; 2–3 h, 15.9 %; 3–4 h, 17.1 %; and >4 h, 20.8 %) (Fig. 1). Similarly, we failed to find a significant relationship between antibiotic timing and mortality in episodes with severe sepsis or septic shock (0–1 h, 23.1 %; 1–2 h, 38.9 %; 2–3 h, 31.8 %; 3–4 h, 22.2 %; and >4 h, 20.0 %) (Fig. 2) or episodes with bacteremia (0–1 h, 33.3 %; 1–2 h, 20.0 %; 2–3 h, 17.4 %; 3–4 h, 9.1 %; and >4 h, 33.3 %) (Fig. 3). In multivariate logistic regression analysis, the independent factors with the highest ORs for outcomes were serum procalcitonin (≤1 vs. >1 h: OR 5.793; ≤2 vs. >2 h: OR 5.759; ≤3 vs. >3 h: OR 5.667; and ≤4 vs. >4 h: OR 5.664; all P < 0.001) and the MASCC risk-index sore (≤1 vs. >1 h: OR 3.947; ≤2 vs. >2 h: OR 3.980; ≤3 vs. >3 h: OR 4.107; and ≤4 vs. >4 h: OR 4.076, all P < 0.001).

Time to antibiotic administration and complication rates in overall febrile neutropenia (FN) episodes (n = 1001). Numbers and complication rates at hourly intervals from triage to antibiotics are shown using a histogram. OR odds ratio, CI confidence interval

Time to antibiotics and mortality rates in FN episodes with severe sepsis or septic shock (n = 67). Numbers and mortality rates at hourly intervals from triage to antibiotics in episodes with severe sepsis or septic shock are shown using a histogram. OR odds ratio, CI confidence interval

Time to antibiotics and mortality rates in FN episodes with bacteremia (n = 64). Numbers and mortality rates at hourly intervals from triage to antibiotics in episodes with bacteremia are shown using a histogram. OR odds ratio, CI confidence interval
Discussion
The question of how antibiotics should be prioritized in the initial management of patients with FN remains unanswered. There is no doubt that timely and appropriate antibiotic administration is crucial in patients with infection or patients who are suspected to have one, especially among those with neutropenia, and current international guidelines recommend initiation of empirical antibiotic administration within 1 h of presentation of FN [1–3]. Several studies have attempted to determine the importance of antibiotics in the initial FN management, assessing the time to antibiotic administration in neutropenic cancer patients presenting to the ED. Szwajcer et al. [16] retrospectively analyzed 68 patients with FN visiting the EDs of a regional health authority. Their median time from triage to antibiotic administration was 5 h (range, 1.23–22.8 h), and timely antibiotic administration was defined as less than 5 h from ED triage. They could not find any deleterious effect (on mortality and increased hospital length of stay) from a delay in antibiotic administration in FN. Recently, Lynn et al. [5] used the decision tree approach in 81 episodes of FN managed at a tertiary medical center in Taiwan and showed that the latency of the first dose of antibiotics was an independent factor associated with serious complications in FN. However, only patients with an absolute neutrophil count (ANC) of <500/μL were included, and by adopting this narrow definition, data on other patients with ANC between 500 and 1000/μL, whose neutrophils were expected to decrease to <500/μL, were likely lost. In addition, relatively small numbers of FN episodes were analyzed, making it more difficult to draw definite conclusions. More recently, Perron et al. [17] reported the data of 105 patients with FN, showing a median time to antibiotic administration of 2.5 h (range, 0.03–50 h) from ED registration and an association between a delay in antibiotic administration and a longer hospital stay. However, no clinical variable, including time to antibiotic administration, significantly correlated with mortality or intensive care unit admission. The above studies were performed retrospectively with relatively small numbers of patients, different primary outcomes, and different inclusion criteria, limiting the generalizability of the findings. So far, no evidence-based recommendations exist for the time of antibiotic administration in FN.
In our study, an analysis of prospectively collected data of 1001 FN episodes with a complication rate of 17.4 % and a median time to antimicrobials of 140 min (IQR, 110–180 min), earlier antibiotic administration was not associated with positive FN outcomes after adjusting for confounders. No impact of time to antibiotics on the mortality rate was shown in the subgroup of patients with bacteremia or severe sepsis or septic shock. In fact, although statistically not significant, patients who had earlier antibiotic administration were shown to have more overall complications (≤1 h, 31.4 vs. >1 h, 16.3 %). Regarding the observational nature of the data collected, it is conceivable that this result could reflect physicians’ tendencies toward earlier antibiotic administration in patients with more unstable conditions.
Not only timely, but also appropriate antibiotic administration is emphasized, and this approach has been shown to improve morbidity and mortality in patients with severe sepsis or septic shock [18–21]. The risk of in-hospital mortality was eight times greater in patients receiving inadequate antibiotics than in those receiving adequate empirical antibiotics [22]. However, in our study, only four out of 64 bacteremias were shown to be from antibiotic-resistant organisms: one methicillin-resistant Staphylococcus aureus and three extended-spectrum beta-lactamase-producing organisms. Due to the low incidence of antibiotic resistance, the effect of the appropriateness of the initial antibiotic therapy on outcome could not be statistically analyzed, and it is likely that the overall appropriateness of the antibiotic prescription, in the context of a prospective trial, may have obscured the effect of timing.
Our study had several limitations. It was performed at a single center using a uniform strategy, and caution should be taken when generalizing the results. Even though we included a relatively large number of FN episodes, the numbers of episodes with bacteremia or severe sepsis or septic shock were not large enough to reveal a strong relationship between antibiotic timing and mortality in this patient subgroup. Similarly, compared with previous reports [12], the risk of death and complications in our included patient population was relatively low: only 10 % of these cases had high-risk features according to the MASCC risk index, and 6.7 % of all episodes had severe sepsis or septic shock. We did not evaluate the potential reasons for delayed antibiotic administration, and we cannot exclude the possibility that patients in a more critical condition received antibiotics sooner and that the results are confounded by these factors. In addition, we did not include the time from the first episode of fever (or any other sign of infection) to the first antibiotic administration, and the relationship between outcomes and the interval from triage to first antibiotic administration could be subject to a huge degree of variability depending on the timing of the patient’s referral to the hospital. In this study also, we did not analyze other outcomes, such as the duration of hospital stay, which was adopted as an outcome of interest in previous studies.
There is no doubt that earlier and appropriate antibiotic administration is crucial in the treatment of patients with neutropenia. However, we could not find strong evidence to support the antibiotic timeline recommendations of several practice guidelines. In multivariate analysis, the independent factors with the highest ORs were found to be procalcitonin concentration and the MASCC risk index score. This result suggests that inflammatory markers and risk stratification tools are more important determinants of outcomes in patients with FN. Our study could not provide sufficient evidence to establish a benefit in outcomes from antibiotic administration within less than 1 or 2 h from ED arrival. Time to antibiotic administration was not a major factor in the outcomes of FN.
References
Freifeld AG, Bow EJ, Sepkowitz KA, Boeckh MJ, Ito JI, Mullen CA, Raad II, Rolston KV, Young JA, Wingard JR, Infectious Diseases Society of A (2011) Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of America. Clin Infect Dis 52(4):e56–93
de Naurois J, Novitzky-Basso I, Gill MJ, Marti FM, Cullen MH, Roila F, Group EGW (2010) Management of febrile neutropenia: ESMO clinical practice guidelines. Ann Oncol 21(Suppl 5):v252–256
Tam CS, O'Reilly M, Andresen D, Lingaratnam S, Kelly A, Burbury K, Turnidge J, Slavin MA, Worth LJ, Dawson L, Thursky KA (2011) Use of empiric antimicrobial therapy in neutropenic fever. Australian consensus guidelines 2011 steering committee. Intern Med J 41(1b):90–101
Zuckermann J, Moreira LB, Stoll P, Moreira LM, Kuchenbecker RS, Polanczyk CA (2008) Compliance with a critical pathway for the management of febrile neutropenia and impact on clinical outcomes. Ann Hematol 87(2):139–145
Lynn JJ, Chen KF, Weng YM, Chiu TF (2013) Risk factors associated with complications in patients with chemotherapy-induced febrile neutropenia in emergency department. Hematol Oncol 31(4):189–196
Gaieski DF, Mikkelsen ME, Band RA, Pines JM, Massone R, Furia FF, Shofer FS, Goyal M (2010) Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med 38(4):1045–1053
Gross PA (2006) Hypotension and mortality in septic shock: the “golden hour. Crit Care Med 34(6):1819–1820
Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL (2008) Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med 36(1):296–327
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M, Early Goal-Directed Therapy Collaborative G (2001) Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 345(19):1368–1377
Innes H, Lim SL, Hall A, Chan SY, Bhalla N, Marshall E (2008) Management of febrile neutropenia in solid tumours and lymphomas using the multinational association for supportive care in cancer (MASCC) risk index: feasibility and safety in routine clinical practice. Support Care Cancer 16(5):485–491
Lee DG, Kim SH, Kim SY, Kim CJ, Park WB, Song YG, Choi JH (2011) Evidence-based guidelines for empirical therapy of neutropenic fever in Korea. Korean J Intern Med 26(2):220–252
Klastersky J, Paesmans M, Rubenstein EB, Boyer M, Elting L, Feld R, Gallagher J, Herrstedt J, Rapoport B, Rolston K, Talcott J (2000) The multinational association for supportive care in cancer risk index: a multinational scoring system for identifying low-risk febrile neutropenic cancer patients. J Clin Oncol 18(16):3038–3051
Ahn S, Lee YS, Chun YH, Kwon IH, Kim W, Lim KS, Kim TW, Lee KH (2011) Predictive factors of poor prognosis in cancer patients with chemotherapy-induced febrile neutropenia. Support Care Cancer 19(8):1151–1158
Ahn S, Lee YS, Lim KS, Lee JL (2013) Adding procalcitonin to the MASCC risk-index score could improve risk stratification of patients with febrile neutropenia. Support Care Cancer 21(8):2303–2308
Ahn S, Lee YS (2012) Predictive factors for poor prognosis febrile neutropenia. Curr Opin Oncol 24(4):376–380
Szwajcer D, Czaykowski P, Turner D (2011) Assessment and management of febrile neutropenia in emergency departments within a regional health authority—a benchmark analysis. Curr Oncol 18(6):280–284
Perron T, Emara M, Ahmed S (2014) Time to antibiotics and outcomes in cancer patients with febrile neutropenia. BMC Health Serv Res 14:162
Houck PM, Bratzler DW, Nsa W, Ma A, Bartlett JG (2004) Timing of antibiotic administration and outcomes for medicare patients hospitalized with community-acquired pneumonia. Arch Intern Med 164(6):637–644
Garnacho J, Sole-Violan J, Sa-Borges M, Diaz E, Rello J (2003) Clinical impact of pneumonia caused by Acinetobacter baumannii in intubated patients: a matched cohort study. Crit Care Med 31(10):2478–2482
Meehan TP, Fine MJ, Krumholz HM, Scinto JD, Galusha DH, Mockalis JT, Weber GF, Petrillo MK, Houck PM, Fine JM (1997) Quality of care, process, and outcomes in elderly patients with pneumonia. JAMA 278(23):2080–2084
Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L, Gurka D, Kumar A, Cheang M (2006) Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 34(6):1589–1596
Valles J, Rello J, Ochagavia A, Garnacho J, Alcala MA (2003) Community-acquired bloodstream infection in critically ill adult patients: impact of shock and inappropriate antibiotic therapy on survival. Chest 123(5):1615–1624
Conflict of interest
The authors declare that they have no conflicts of interest. We have full control of all primary data and agree to allow the journal to review the data if requested.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ko, B.S., Ahn, S., Lee, YS. et al. Impact of time to antibiotics on outcomes of chemotherapy-induced febrile neutropenia. Support Care Cancer 23, 2799–2804 (2015). https://doi.org/10.1007/s00520-015-2645-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-015-2645-5