
Abstract
Purpose
Postoperative wound infection (WI) is a main complication after head and neck surgery. Poor oral health may be a risk factor for WI. We therefore assessed the contribution of oral health care in preventing postoperative WI in patients with oral squamous cell carcinoma (OSCC).
Methods
A total of 66 consecutive inpatients with OSCC (mean age, 68 years) was divided into two groups that did or did not receive oral health care. There were no significant between group differences in gender, age, or T-, N-, or clinical stage. Patients in the care group were given oral health care plans by doctors of oral medicine, whereas patients in the control group were not. Twenty-three variables were recorded for each patient.
Results
WI was observed in 14/66 patients (21%), three (3/33 = 9%) in the care group and 11 (11/33 = 33%) in the control group (p < 0.025). Univariate statistical analysis showed that 11 factors correlated with WI significantly: T-stage, clinical stage, wearing of dentures, tracheostomy, neck dissection, tissue transplantation, oral health care, preoperative radiation, blood transfusion, operation time, and blood loss. In multiple logistic regression analysis, only two factors were significant independent risk factors for WI: tissue transplantation (p = 0.01; odds ratio, 24.5) and lack of oral health care (p = 0.04; odds ratio, 6.0).
Conclusion
Oral health care may reduce the risk of postoperative WI in patients with OSCC.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The number of the patients with oral cancer is increasing gradually. Although diagnostic modalities and therapeutic management of oral cancer have improved, there has been little improvement in treatment outcome, frequency of complications after surgery, and prognosis of patients with advanced oral cancer [16]. Complications after surgery for patients with oral cancer increase treatment costs and lower patient quality of life (QOL), and can also affect prognosis [6, 15]. Postoperative infection is a major complication, and includes wound infection (WI) and non-wound infection (NWI) [5, 8]. WI may cause significant morbidity, poor cosmetic results, delayed wound healing, and prolonged hospitalization [5, 8], leading to delayed postoperative cancer treatment. Patients with postoperative WI were more likely to have recurrent disease than those who remained free of postoperative WI [8]. Therefore, it is so important to prevent WI in patients with oral squamous cell carcinoma (OSCC).
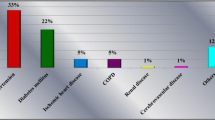
WI rate after surgery is mainly determined by the degree of contamination of the wound [5]. Surgery of oral cancer is usually clean contaminated, and develops relatively high rates of WI. Grandis et al. [8] reported that postoperative WI developed in 22% of patients with head and neck SCC. De Melo et al. [6] reported a WI rate of 23% in patients with OSCC. Preoperative risk factors for postoperative WI are thought to be related to the patients (e.g., diabetes mellitus, nutritional deficiency, excessive tobacco, and/or alcohol intake, poor oral health and dental status), to the tumor (e.g., stage and localization of the tumor), and to the treatment (e.g., prior radiotherapy, prior chemotherapy, or tracheostomy) [5, 6, 11, 13, 14]. Intraoperative risk factors are thought to be related to the type of surgical procedure (e.g., extent of resection, method of reconstruction, and individual surgical technique) [8, 9, 13].
Microorganisms in the oral cavity may be sources of pathogenesis of postoperative WI and NWI, including bacterial pneumonia following head and neck surgery [1, 12]. Oral health care has been found to reduce the number of microorganisms in the oral cavity, thereby decreasing the incidence of bacterial pneumonia [21]. We started performing systematic oral health care in patients with OSCC in April 2006 to prevent NWI including bacterial pneumonia. We hypothesized that poor oral health may be also an important risk factor for postoperative WI in patients with oral cancer. Many of these patients have poor oral health due to their inability to perform adequate oral care because of the pain and swelling caused by oral cancer [17]. Moreover, dry mouth and impairment of self-cleaning of the oral cavity worsens their oral health. To our knowledge, it has not been determined whether oral health care would lower the risk of postoperative WI in patients with OSCC. We therefore assessed whether systematic oral health care could prevent postoperative WI during treatment of inpatients with OSCC.
Patients and methods
Patients
The study included 66 consecutive inpatients with OSCC at Hokkaido University Hospital between 2005 and 2007. Of these patients, 40 (61%) were men and 26 (39%) were women; their average age was 68 years (range, 24-89 years). Thirty-three patients referred to our hospital from April 2006 to March 2007 received systematic oral health care (care group), whereas 33 referred from April 2005 to March 2006 did not receive systematic oral health care (control group). As we started systematic oral health care to the patients with OSCC in April 2006, the patients were divided into two groups automatically according to the term of administration. Gender, age, the primary tumor sites, T-stage, N-stage, and clinical stage of both groups are listed in Table 1. There were no significant between group differences in gender distribution, patient age, or T-stage, N-stage, or clinical stage (Table 1).
This study was approved by the Institutional Review Boards of Hokkaido University, Graduate School of Dental Medicine (2006).
Treatment
All 66 patients underwent surgery, with 18 receiving pre-operative chemotherapy and 11 receiving preoperative radiotherapy. Surgical technique (i.e., tracheostomy, radical neck dissection) and pre-operative radiation and chemotherapy in the care and control groups are listed in Tables 2 and 3. Tissue transplantation was performed in 18 patients in the care group (53%) and 16 in the control group (47%). Free flap transplantation with microsurgery was performed on four patients in the care group, with three receiving rectus abdominis musculocutaneous flaps and one receiving an anterolateral thigh flap. Free flap transplantation was performed on five patients in the control group, with one receiving a rectus abdominis musculocutaneous flap, two receiving osteocutaneous scapular flaps, and two receiving anterolateral thigh flaps. Split-thickness skin grafts were performed in 14 patients in the care group and 11 in the control group. Primary closure was performed in eight and ten patients, respectively, with collagen-based artificial dermis (TERUDERMIS®; Olympus Terumo Biomaterials Corp. Tokyo, Japan) used for closure in seven patients in each group (Table 3). No patients entered the intensive care unit after surgery.
Systematic oral health care and dental status
Each patient in the care group was given an oral health care plan by doctors of oral medicine and dental hygienists, including professional mechanical teeth cleaning (PMTC), scaling, and instruction on how to care for their oral health. Each patient in the care group received PMTC and scaling at least one time until surgery. Each patient was instructed on the manner of tooth brushing using appropriate dental brush and dental floss, on cleaning the oral mucosa and tongue using a sponge brush and mouth rinse (Biotene Mouthwash®; Incorporated Healthcare Products, Gardena, CA, USA) and on the application of oral moisturizing gel (Biotene Oral Balance®; Incorporated Healthcare Products, Gardena, CA, USA) to the oral mucosa. This mouth rinse was selected as it is an available alcohol-free mouth rinse [18], that contains the enzymes; lysozyme, sialoperoxidase, and lactoferin. These enzymes have been shown to have anti-microbial effects in the oral cavity [6, 7]. Care was carefully applied to avoid irritation to the tumor site. The doctors of oral medicine performed care on each patient once a day, and the patients performed self-care five times per day from the first day of admission to the day before surgery. On the first day following surgery, the doctors and the patients continued to perform oral health care in the same manner. If the patients could not perform this oral health care by themselves, the doctors supported them in this care. All of the patients could perform oral health care independently by themselves. In the control group, special care was not applied by dentists and dental hygienists, with only self-care performed as usual. From the next day following surgery, the dentist performed oral care around the wound one or two times per day with physiological saline.
At the time of operation, 56 patients were dentulous, ten were edentulous, and 37 were wearing dentures. Periodontal diseases were evaluated according to periodontal status described by WHO [3, 20]. In the present study, 30 patients were defined as having periodontal disease (Table 2). The percentage of patients with periodontal disease was significantly higher in the care group than in the control group (chi-square: 3.9: p < 0.05). However, there were no significant differences between the two groups for teeth or denture status (Table 2). Radiographs revealed chronic apical lesions in six cases in the care group and seven cases in the control group. Preoperatively, “bad teeth” were extracted in three cases and four cases, and during surgery, in ten and three cases in the care and control groups, respectively. These teeth were extracted because of periodontal disease, apical lesions, advanced caries, and inclusion in the extent of resection of cancer. There were no significant correlations between these dental treatments and WI (data not shown).
Antibiotic
All patients in both groups were administrated cephalosporin antimicrobial drugs (cefazolin sodium: 2 g/day or cefmetazole sodium: 2 g/day), beginning just before surgery, and continuing for 3 days after surgery.
Definition of WI
According to the criteria of Johnson et al., WI was defined as the presence of purulent drainage from the wound or the presence of an orocutaneous fistula regardless of origin. Erythema, induration, or tenderness around the suture line was not accepted as indicative of WI. WI was defined only when the microbial cultures revealed positive [4, 8, 13].
Factors
The 23 variables recorded for each patient included patient characteristics (gender, age, tobacco and alcohol history, diabetes mellitus, teeth and denture status, periodontal diseases, preoperative white blood count, and preoperative serum albumin levels), disease characteristics (T-stage, N-stage, and clinical stage), previous treatment (preoperative chemotherapy, preoperative radiation, oral health care, and duration of hospital stay before surgery), and surgical procedure (tissue transplantation, tracheostomy, neck dissection, operation time, blood loss, and blood transfusion).
Patients who had smoked prior to hospital admission and had stopped smoking less than 1 year before admission were considered as having tobacco habits. All patients were prevented from smoking while in hospital. Patients who drank alcohol more than three times per week were considered as having alcohol habits.
The percentage of the patients with tobacco habits was significantly higher in the care group than in the control group (chi-square: 3.9: p < 0.05). However, there were no significant between group differences for the other 19 factors (Tables 1, 2, and 3).
Statistics analysis
For univariate statistical analysis, we used the chi-square test or the Mann-Whitney U test. For multiple logistic regression analysis, we used median patient age, operation time, blood loss, duration of hospital stay before surgery, white blood cell count, and serum albumin to divide patients into two groups. Patients with T1/T2, N-negative, stage I/II were defined as the “low group”, and those with T3/T4, N-positive, and stage III/IV were defined as the “high group”. StatView J-5.0 (Abacus Concepts, Berkeley, CA, USA) was used for all statistical analyses. All p values less than 0.05 were considered statistically significant.
Results
Of the 66 patients, 14 (21%) had WI, three of 33 (9%) in the care group, and 11 of 33 (33%) in the control group (p < 0.025). WI was found in eight cases intraorally, two cases extraorally, and in four cases as orocutaneous fistula.
In univariate statistical analysis, 11 factors significantly correlated with WI, including T-stage (p < 0.05), clinical stage (p < 0.025), denture status (p < 0.025), preoperative radiation (p < 0.005), tracheostomy (p < 0.01), neck dissection (p < 0.025), tissue transplantation (p < 0.005), oral health care (p < 0.025), blood transfusion (p < 0.005), operation time (p = 0.01), and blood loss (p = 0.02; Table 4).
In multiple logistic regression analysis, only two factors were significant independent risk factors for WI: tissue transplantation (p = 0.01, odds ratio (OR): 24.5, 95% confidence interval (CI): 2.2-273.6) and oral health care (p = 0.04, OR: 6.0, 95% CI: 1.1-34.3; Table 5).
Discussion
We have shown here that the systematic oral health care lowered the risk of postoperative WI in patients with OSCC. To our knowledge, it has not been studied whether systematic oral health care reduces the risk of post-operative WI in patients with OSCC.
In selecting factors to evaluate, we chose those previously shown to be risk factors for post-operative WI [5, 6, 11, 13, 14]. We especially focused on oral health care, since microorganisms in the oral cavity are possible sources of pathogens of WI [12]. Many patients with oral cancer have poor oral health, since they cannot perform adequate oral care due to, for example, bleeding, dry mouth, pain, and/or swelling caused by oral cancer. Some tumorigenesis-associated dysfunctions, such as eating and swallowing disorders, can seriously impair patient QOL and might worsen a patient’s oral and general conditions. Moreover, these dysfunctions can lead to serious complications during treatment. Oral health care may not only reduce the number of microorganisms in the oral cavity, but stimulate oral membranes, leading to activation of the swallowing reflex, secretion of saliva, and stimulation of muscle functions. These reactions may contribute to more rapid patient recovery. Patients undergoing surgery for oral cancers should be made aware of their conditions and of the need for oral hygiene.
Several risk factors for WI have been identified in patients undergoing head and neck surgery [5, 6, 11, 13, 14]. The pathogenesis of WI after head and neck surgery traditionally has been explained in terms of mechanical factors, such as tumor size, extent of resection, method of reconstruction, and individual surgical technique [8, 19]. Patients with stage IV tumors have been found to be at higher risk for postoperative WI than patients with lower stage tumors [13]. In addition, complex reconstruction increases the risk of mucocutaneous fistula and WI [10, 19]. Patients requiring blood transfusion after head and neck surgery were found to be at increased risk of WI [10, 19], because of decreased phagocytic cell function and impaired immunity after blood transfusion [2, 14, 19]. Other factors identified as significantly associated with WI include age, blood loss, operation time, previous chemotherapy, tracheostomy, and preoperative duration of hospital stay [6, 13, 14]. In the present study, univariate analysis identified the above 11 factors as significantly altering the incidence of WI. Many of these factors, however, are related to each other, such as T-stage and clinical stage, preoperative radiation and duration of hospital stay before surgery, operation time and blood loss, blood transfusion and blood loss, neck dissection and tracheostomy, and operation time and tissue transplantation. We therefore performed multiple logistic regression analysis to identify independent risk factors for WI.
In addition to oral health care, we found that tissue transplantation was an independent significant risk factors for WI. Since tissue transplantation is usually performed for cosmetics reasons and/or to preserve patient functionality after surgery [14], it is not reasonable to avoid tissue transplantation, even if it is a significant risk factor for WI. The result presented here showed that oral health care effectively prevented WI, independent of tissue transplantation.
We found it difficult to quantitatively evaluate several important factors, including nutritional deficiency, tumor localization, extent of resection, and individual surgical technique. Although we substituted serum albumin concentration for nutritional conditions, albumin levels may not be low, even in the presence of nutritional depletion [4]. Tumor localization and extent of resection were excluded from evaluation, because we evaluated patients with tumors at various primary sites. Regarding individual surgical technique, all of the operations were performed by a small number of oral cancer specialists. Moreover, we thought that preoperative dental status may be an important risk factor for postoperative WI. However, univariate statistical analysis showed that only lack of dentures was a significant risk factor for WI. Penel et al. [14] reported that the preoperative dental status (bad, good, or edentulation) were not significant risk factors for WI in patients with head and neck cancer. We think that it is very difficult to evaluate patients’ dental status quantitatively, because each patient may show several different dental conditions.
Patients with postoperative WI have been found more likely to develop recurrent disease than those free of postoperative infection [8]. Thus, efforts to prevent postoperative WI are very important, especially when considering an individual patient’s prognosis and QOL.
In conclusion, the results presented here indicate that oral health care may reduce the risk of postoperative WI in patients with OSCC. To our knowledge, this study is the first to demonstrate the usefulness of oral health care for patients with OSCC.
References
Abe S, Ishihara K, Okuda K (2001) Prevalence of potential respiratory pathogens in the mouths of elderly patients and effects of professional oral care. Arch Gerontol Geriatr 32(1):45–55
Blumberg N, Heal JM (1989) Transfusion and recipient immune function. Arch Pathol Lab Med 113(3):246–253
Brailo V, Vučićević-Boras V, Cekić-Arambašin A, Alajbeg IŽ, Milenović A, Lukač J (2006) The significance of salivary interleukin 6 and tumor necrosis factor alpha in patients with oral leukoplakia. Oral Oncol 42:370–373
Brown BM, Johnson JT, Wagner RL (1987) Etiologic factors in head and neck wound infections. Laryngoscope 97(5):587–590
Coskun H, Erisen L, Basut O (2000) Factors affection wound infection rates in head and neck surgery. Otolaryngol Head Neck Surg 123(3):328–333
de Melo GM, Ribeiro KCB, Kowalski LP, Deheinzelin D (2001) Risk factors for postoperative complications in oral cancer and their prognostic implications. Arch Otolaryngol Head Neck Surg 12(7):828–833
Epstein JB, Emerton S, Le ND, Steveson-Moore P (1999) A double-blind crossover trial of Oral Balance gel and Biotene® toothpaste versus placebo in patients with xerostomia following radiation therapy. Oral Oncol 35:132–137
Grandis JR, Snyderman CH, Johnson JY, Yu VL, D’Amico F (1992) Postoperative wound infection. A poor prognostic sign for patients with head and neck cancer. Cancer 70(8):2166–2170
Johnson JT (1983) Prophylaxis in surgical procedures. Am J Otolaryngol 4(6):433–434
Joyce LD, McQuarrie DG (1976) Applications of contemporary reconstructive techniques in head and neck surgery for anterior oral-facial cancers. Surgery 80(3):373–378
Kowalski LP, Alcantara PSM, Magrin J, Parise Junior O (1994) A case-control study on complications and survival in elderly patients undergoing major head and neck surgery. Am J Surg 168(5):485–490
Matsunaga K, Oobu K, Yoshikawa H, Sasaguri M, Takeda E, Tauchi A, Kawano S, Nagata T, Ohishi M (2002) A clinical study of postoperative infection in oral and maxillofacial surgery. J Jpn Stomatol Soc 51(1):62–68
Ogihara H, Takeuchi K, Yuta A, Majima Y (2005) Analysis of risk factors of postoperative infection in head and neck surgery. J Jpn Soc Infect Dis in Otolaryngol 23(1):116–118
Penel N, Lefebvre D, Fournier C, Sarini J, Kara A, Lefebvre JL (2001) Risk factors for wound infection in head and neck cancer surgery: a prospective study. Head Neck 23(6):447–455
Rhys Evans PH (1989) Complications in head and neck surgery and how to avoid trouble. J Laryngol Otol 103(10):926–929
Seiwert TY, Cohen EEW (2005) State-of-the-art management of locally advanced head and neck cancer. Br J Cancer 92(8):1341–1348
Suzuki K (2004) Prevention of respiratory infections in the elderly. Jpn J Gerodontol 18(4):301–308
Warde P, Kroll B, O’Sullivan B, Aslanidis J, Tew-George E, Waldron J, Maxymiw W, Liu FF, Payne D, Cummings B (2000) A phase II study of Biotene in the treatment of postradiation xerostomia in patients with head and neck cancer. Support Care Cancer 8:203–208
Weber RS, Hankins P, Rosenbaum B, Raad I (1993) Nonwound infections following head and neck oncologic surgery. Laryngoscope 103(1):22–27
World Health Organization (1997) Oral health surveys. Basic methods. Geneva, World Health Organization
Yoneyama K, Yoshida M, Matsui T, Sasaki H, Oral Care Working Group (1999) Oral care and pneumonia. Lancet 354(9177):515
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Additional Table 1
Correlations between the dental status and WI (PPT 94 kb)
Rights and permissions
About this article
Cite this article
Sato, J., Goto, J., Harahashi, A. et al. Oral health care reduces the risk of postoperative surgical site infection in inpatients with oral squamous cell carcinoma. Support Care Cancer 19, 409–416 (2011). https://doi.org/10.1007/s00520-010-0853-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-010-0853-6