
Abstract
Objectives
Prevalence of bisphosphonate-associated osteonecrosis of the jaws within the catchment area of a university hospital maxillofacial unit and to review the outcome of treatment.
Methods
In a retrospective study, all patients with osteonecrosis, osteomyelitis and osteoradionecrosis treated in the period from January 2000 to March 2005 in the department for Maxillo Facial Surgery at the University of Mainz, Germany were analysed.
Results
Forty percent of the patients are grouped to odontogenic or surgically induced osteomyelitis. The second largest group (28%) were patients with osteoradionecrosis (ORN). Ten percent of all patients developed an osteonecrosis after treatment with bisphosphonates (BOJ). Eight percent showed osteomyelitis or sequester due to a trauma while 14% of all patients had osteomyelitis of unknown origin. All BOJ patients took bisphosphonates because of metastatic diseases of the bone (plasmocytoma, mamma carcinoma and prostate cancer) for up to 5 years. All had been administered a nitrogen-containing bisphosphonate (either pamidronat or zoledronat). Thirteen out of the 17 patients with BOJ and 14 of the 45 with ORN reported a possible trigger like previous tooth extraction, pressure denture sore or periodontal diseases.
Conclusion
These findings support the association of bisphosphonate therapy and osteonecrosis of the jaw. The importance of this new disease is characterised by the growing number of patients. The role of dental trigger factors and the poor surgical outcome both seem to justify a prophylactic dental care concept in high-risk patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bisphosphonates can be grouped into nitrogen-containing and non-nitrogen-containing bisphosphonates (Table 1). Currently, they are the most important anti-resorptive agents used in the treatment of metabolic bone diseases, metastatic diseases to the bone, hypercalcemia, Paget’s disease and osteoporosis [1]. Known since the 19th century, they were first synthesised in 1865. The therapeutic efficiency was improved by chemical modifications of the molecule [2]. Effects of bisphosphonates are inhibition of osteoclasts, adhesion of tumour cells to mineralised bone, inhibition of tumour cell proliferation and infiltration [3, 4]. Furthermore, apoptosis of tumour cells is induced and cytotoxic T cells are stimulated [5].
Because of their low lipophilicity, bisphosphonates are poorly resorbed from the gastrointestinal tract [6]. About 50% of the resorbed dose bind to bone; the rest is immediately eliminated by the kidneys without metabolisation. The half-live period of bisphosphonates in plasma is a few hours [7, 8] but in the bone, about 10 years [6].
Bisphosphonates specifically bind to hydroxyapatite and are ingested by osteoclasts, in which the drugs influence cell functions. Non-nitrogen-containing bisphosphonates are built into the ATP molecule and finally have a cytotoxic effect, whereas nitrogen-containing bisphosphonates inhibit the cholesterol synthesis. By both mechanisms, the osteoclast’s signal transmission is disturbed [9, 10].
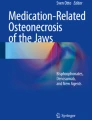
Known side effects of bisphosphonates are local damages of the mucous membrane, gastrointestinal bleedings, abdominal pain, perforating ulcera ventriculi, vomiting and oesophagitis. Recently, articles of a new side effect of bisphosphonates have been published. The first to describe the new phenomenon was Marx in 2003 [11] who reported 36 cases of painful bone exposure (Fig. 1) in the mandible, maxilla or both. These lesions were resistant to any kind of surgical or medical treatment. The patients in this report received bisphosphonates because of plasmocytoma, breast carcinoma or osteoporosis. In 78%, a dental treatment was described before the bone exposure. In this period, further episodes were reported [12–15].

This clinical photograph shows exposed bone of the maxilla. A large area distal and a second smaller area mesial. The patient took bisphosphonates for 4 years because of a mamma carcinoma with multiple metastasis
Several theories on necrosis development are being discussed in literature. Important factors seem to be the bisphosphonate’s anti-angiogenetic potency [16–18] and the effect on osteoclasts [19]. Moreover a possible effect on osteoblasts [20] and osteocytes [21] is discussed. A typical histologic pattern is patchy areas of necrosis in contrast to the osteoradionecrosis where larger areas are affected [22]. It is interesting that the bone necrosis has only been described for the jaws. One reason might be the increased danger of contamination with bacteria by direct contact to the bone, e.g. after tooth extraction, periodontic lesions or pressure denture sore. It should be noted that a similar symptomatic has been described as phossy jaw by Dearden in 1899 in workers producing matches [23].
As therapy is critical, prevention seems to play an important role. It is accepted that necrotic areas should be removed and covered with soft tissue [15]. Several differential diagnoses exist. These are osteoradionecrosis, trauma-induced infections of the bone, surgical and odontogenic infections together with infections and necrosis of unknown origin.
In several case series, the existence of this special disease has been described and is generally accepted. On the other hand frequency and relevance are often discussed in controversy. The purpose of this study was to describe the demographic and clinical parameters of patients that were hospitalised due to osteonecrosis of the jaws. The specific aim of the study was to obtain data on the prevalence of bisphosphonate-associated osteonecrosis of the jaws and to report on the outcome of treatment.
Materials and methods
Study population and design
In this retrospective study, all patients who were treated in the Clinic of Oral and Maxillofacial Surgery at the University of Mainz, Germany in the period from January 2000 to March 2005 were comprised, who fulfiled the following criteria: (1) The clinical or clinical and histopathological diagnosis was either osteonecrosis, sequester or bone infection. (2) Located at the mandible, maxilla or both. In detail, a PC based searching algorithm for diagnosis and treatment procedures was applied to all patient records of the concerning years. Using these criteria, 163 patients were included. All patient records were evaluated and patients were allocated into five groups:
-
Bisphosphonate associated necrosis: all patients with osteonecrosis, sequester or bone infection and a bisphosphonate anamnesis were included. Additionally, all patients with concomitant diseases that potentially indicated the use of bisphosphonates (breast cancer, plasmocytoma, prostate cancer, Paget’s disease or osteoporosis) were phoned and their physicians were asked for a drug history to identify the possible use of bisphosphonates. Patients fulfiling these criteria (diagnosis plus anamesis) were included in this group. As histopathological criteria for bisphosphonate osteonecrosis are not yet available, the diagnosis was done primary clinical due to anamnesis and supported histopathologically if possible.
-
Osteoradionecrosis: patients with a history of head and neck cancer treated surgically and with postoperative radiation therapy who developed in the aftermath osteoradionecrosis were included into this group. The diagnosis was clinical, radiological and histolopathological.
-
Traumatainduced infections: patients with a previous trauma and consecutive fracture of the bone but with no bisphosphonate or radiation in anamnesis were assorted in this group. The diagnosis was clinical and radiological.
-
Surgical and odontogenic infections: patients with a history of dental surgery or dental infections with osteomyelitis or sequester not belonging to one of the above named groups were assorted in this group.
-
Infections and necrosis of the bone of unknown origin: patients who presented none of the above criteria.
From all patient histories, the following data were extracted: patients’ age, gender, localisation and chronologic appearance. For the bisphosphonate group, the kind of bisphosphonate that was applied and possible triggers like tooth extraction or periodontal diseases were recorded.
The groups were compared concerning number of patients, demographic data and localisation. Due to the explorative character of this study, the statistical analysis was restricted to a descriptive analysis only.
Results
Demographic data of the patients are given in Table 2. The largest number of patients (40%) is found in the group odontogenic or surgically induced osteomyelitis. The second largest group (28%) were patients with osteoradionecrosis. Ten percent of all patients developed an osteonecrosis after treatment with bisphosphonates. Eight showed osteomyelitis or sequester due to a trauma while 14% of all patients had osteomyelitis of unknown origin. The average age of patients in the bisphosphonate group is the highest with 64 years. Patients with osteoradionecrosis show an average age of 58 years. The bisphosphonate group and patients with unknown origin of the osteonecrosis contains more female patients than male patients. The trauma and osteoradionecrosis groups mainly consisted of male patients.
The majority of patients (n=9) of the bisphosphonate group had first received pamidronat followed by zoledronat. Two patients took zoledronat and later ibandronat. One patient took pamidronat only, another one received pamidronat which was disrupted by a phase with zoledronat. The remaining four patients took zoledronat only. In all patients, the medication was applied at least for 1 year and for a maximum of 5 years until the necrosis developed (Table 3). In the years 2000 and 2001, no patient with bisphosphonate-associated necrosis was seen at our clinic. In the next years, the number of patients increased by every year: 2002, two patients; 2003, four patients; 2004, eight patients. In 2005, 17 patients were seen, of which three were included into this study due to the proposed time period. The patient numbers in the other groups were not changing over the years. Taking this into account, the number of patients with bisphosphonate-associated necrosis has exceeded the number of patients with osteoradionecrosis in the year 2004 and is constantly growing. In 2005, it has become the major reason for osteonecrosis in our group of patients.
The bisphosphonates were administered because of plasmocytoma (nine patients), mamma carcinoma (seven patients) and prostate cancer (one patient). Thirteen patients out of the 17 patients with bisphosphonates-associated osteonecrosis reported possible trigger factors. They underwent prior dental treatment or reported pressure denture sore or periodontal diseases before a necrosis developed. No obvious dental or surgical reason was detected in the other cases. In the group of patients with osteoradionecrosis, only 14 out of 45 patients (31%) had trigger factors as described above.
In all patients, the bisphosphonate necrosis was resistant to conservative therapy like medical treatment with antibiotics and local treatment with disinfection. The treatment data of the patients is given in Table 3. Surgical treatment with decortication, sequestrotomia with soft tissue covering was performed in all cases, if the general status of the patient allowed it. Out of the 15 patients who underwent surgical therapy until March 2005 only two had no relapse.
Discussion
In this study, the prevalence of bisphosphonates-associated necrosis of the jaw related to the population of patients with osteonecrosis in the time period of the last 5 years was evaluated. During this time period, the overall prevalence was 10%. But with constantly growing incidence in the last 2 years, it has in 2005 become the major reason for osteonecrosis in our group of patients. All patients with bisphosphonate-associated necrosis were administered nitrogen-containing bisphosphonates. These findings align to data from case reports [11, 14]. Pamidronat and zoledronat seem to provoke the development of osteonecrosis. The problem in the interpretation of the data is that the overall incidence of bisphosphonate-associated osteonecrosis is unknown. Even the prevalence within the group of patients regularly taking bisphosphonates is not known yet.
The clinical entity of bisphosphonate associated osteonecrosis has been described only recently in 2003. This correlates with the findings in our clinic. In the aftermath the number of patients increased at our clinic. Aledronat was first used in Germany in 1996, pamidronat in 1999 and zoledronat in 2001. In our patients from the very beginning of the ingestion of the drug to the appearance of the necrosis the time period was 1 to 5 years.
The average age of the patients reflects the age of the patients with the underlying diseases. A major part of tumours of the head and neck region occur between the fifth and sixth decade [24]. Breast cancer, prostate carcinoma and plasmocytoma are malign diseases of the advanced age. This is of relevance because of the therapy decision. Often, therapy options are limited due to the associated diseases.
In contrast to the largest case series, where 13% of the patients received bisphosphonates because of osteoporosis [14], in our study, all patients took the bisphosphonate within the scope of malignant diseases. The genesis of this special osteonecrosis is discussed controversially in the literature. Osteonecrosis can appear with prostate cancer [25], breast cancer [26] or in any way with malignant diseases [27]. The therapy resistance of bisphosphonate-associated osteonecrosis compared to osteonecrosis of other origin is of considerable interest. Eventually, a bisphosphonate therapy in combination with cytostatic therapy nurtures the development of osteonecrosis.
In general, the mandible is affected by the osteonecrosis comparable to the osteoradionecrosis [28–30]. A reason for this might be the more critical blood circulation of the mandible [30]. A further factor for the bisphosphonate-associated osteonecrosis is the anti-angiogenetic potency [16, 18] that could boost this mechanism. The endothelial proliferation is inhibited by bisphosphonates. One can assume that the bone’s blood circulation is altered.
Conspicuous is the existence of trigger factors (dental origin) in a large number of bisphosphonate-associated osteonecrosis. A contamination of bacteria to the bone is possible via pressure denture sores, extraction alveolus or periodontal diseases. According to, this very often, a tooth extraction is reported in the anamnesis [31]. In contrast, osteoradionecrosis seems to appear more often spontaneously. Risk factors for the development of osteoradionecrosis are the tumour’s localisation, the kind of operation, the total dose of radiation, the applied daily dose of radiation, the radiation modus and the dental status [29]. This difference between osteoradionecrosis and bisphosphonate-associated necrosis is that the former received special dental care before irradiation, which often involves preventive teeth extraction. Moreover, these patients are well cared during and after the period of radiation [32]. With respect to the high number of patients, who reported a dental trigger factor, a special dental hygiene and treatment plan should be considered before the administration of bisphosphonates. An additional risk factor might be the combination of bisphosphonate therapy and radiation as it is discussed for patients with prostate cancer or plasmocytoma [33, 34]. In our study, only two patients have responded to the treatment until now. This resistance to therapy is discussed in literature as a characteristic point of bisphosphonate-associated osteonecrosis [14, 35].
As a clinical conclusion, with respect to the difficulties in treatment of bisphosphonate-associated osteonecrosis and the high rate of trigger factors, the prevention of this clinical problem should be focused. Due to the rising prevalence in the last 2 years, a dental examination at the beginning of a new bisphosphonate therapy with adequate restorations seems to be reasonable. The patients should be instructed in sufficient mouth hygiene and informed about the possible risk for osteonecrosis. The next important scientific step might be to estimate the incidence of bisphosphonate-associated osteonecrosis and calculate the value and benefit of prophylactic measures.
References
Rogers MJ, Gordon S, Benford HL, Coxon FP, Luckman SP, Monkkonen J, Frith JC (2000) Cellular and molecular mechanisms of action of bisphosphonates. Cancer 88:2961–2978
Fleisch H (2002) Development of bisphosphonates. Breast Cancer Res 4:30–34
van der Pluijm G, Vloedgraven H, van Beek E, van der Wee-Pals L, Lowik C, Papapoulos S (1996) Bisphosphonates inhibit the adhesion of breast cancer cells to bone matrices in vitro. J Clin Invest 98:698–705
Boissier S, Magnetto S, Frappart L, Cuzin B, Ebetino FH, Delmas PD, Clezardin P (1997) Bisphosphonates inhibit prostate and breast carcinoma cell adhesion to unmineralized and mineralized bone extracellular matrices. Cancer Res 57:3890–3894
Clezardin P, Fournier P, Boissier S, Peyruchaud O (2003) In vitro and in vivo antitumor effects of bisphosphonates. Curr Med Chem 10:173–180
Lin JH (1996) Bisphosphonates: a review of their pharmacokinetic properties. Bone 18:75–85
Perry CM, Figgitt DP (2004) Zoledronic acid: a review of its use in patients with advanced cancer. Drugs 64:1197–1211
Leyvraz S, Hess U, Flesch G, Bauer J, Hauffe S, Ford JM, Burckhardt P (1992) Pharmacokinetics of pamidronate in patients with bone metastases. J Natl Cancer Inst 84:788–792
Amin D, Cornell SA, Gustafson SK, Needle SJ, Ullrich JW, Bilder GE, Perrone MH (1992) Bisphosphonates used for the treatment of bone disorders inhibit squalene synthase and cholesterol biosynthesis. J Lipid Res 33:1657–1663
Amin D, Cornell SA, Perrone MH, Bilder GE (1996) 1-Hydroxy-3-(methylpentylamino)-propylidene-1,1-bisphosphonic acid as a potent inhibitor of squalene synthase. Arzneimittelforschung 46:759–762
Marx RE (2003) Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of jaws: a growing epidemic. J Oral Maxillofac Surg 61:1115–1117
Carter GD, Goss AN (2003) Bisphosphonates and avascular necrosis of the jaws. Aust Dent J 48:268
Migliorati CA (2003) Bisphosphanates and oral cavity avascular bone necrosis. J Clin Oncol 21:4253–4254
Ruggiero SL, Mehrotra B, Rosenberg TJ, Engroff SL (2004) Osteonecrosis of the jaws associated with the use of bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg 62:527–534
Grötz KA, Diel IJ (2005) Osteonekrose des Kiefers unter Bisphosphonat Langzeittherapie. Im Focus Onkologie 8:52–55
Fournier P, Boissier S, Filleur S, Guglielmi J, Cabon F, Colombel M, Clezardin P (2002) Bisphosphonates inhibit angiogenesis in vitro and testosterone-stimulated vascular regrowth in the ventral prostate in castrated rats. Cancer Res 62:6538–6544
Santini D, Vincenzi B, Avvisati G, Dicuonzo G, Battistoni F, Gavasci M, Salerno A, Denaro V, Tonini G (2002) Pamidronate induces modifications of circulating angiogenetic factors in cancer patients. Clin Cancer Res 8:1080–1084
Wood J, Bonjean K, Ruetz S, Bellahcene A, Devy L, Foidart JM, Castronovo V, Green JR (2002) Novel antiangiogenic effects of the bisphosphonate compound zoledronic acid. J Pharmacol Exp Ther 302:1055–1061
Hughes DE, Wright KR, Uy HL, Sasaki A, Yoneda T, Roodman GD, Mundy GR, Boyce BF (1995) Bisphosphonates promote apoptosis in murine osteoclasts in vitro and in vivo. J Bone Miner Res 10:1478–1487
Pan B, Farrugia AN, To LB, Findlay DM, Green J, Lynch K, Zannettino AC (2004) The nitrogen-containing bisphosphonate, zoledronic acid, influences RANKL expression in human osteoblast-like cells by activating TNF-alpha converting enzyme (TACE). J Bone Miner Res 19:147–154
Plotkin LI, Aguirre JI, Kousteni S, Manolagas SC, Bellido T (2005) Bisphosphonates and estrogens inhibit osteocyte apoptosis via distinct molecular mechanisms downstream of extracellular signal-regulated kinase activation. J Biol Chem 280:7317–7325
Hansen T, Kunkel M, Weber A, James Kirkpatrick C (2006) Osteonecrosis of the jaws in patients treated with bisphosphonates—histomorphologic analysis in comparison with infected osteoradionecrosis. J Oral Pathol Med 35:155–160
Dearden WF (1899) Fragilitas ossium amongst workers in Lucifer match factories. BMJ 2:270
Bernardi D, Barzan L, Franchin G, Cinelli R, Balestreri L, Tirelli U, Vaccher E (2005) Treatment of head and neck cancer in elderly patients: state of the art and guidelines. Crit Rev Oncol Hematol 53:71–80
Macdonald AG, Bissett JD (2001) Avascular necrosis of the femoral head in patients with prostate cancer treated with cyproterone acetate and radiotherapy. Clin Oncol (R Coll Radiol) 13:135–137
Dawson LK, Nussey F, Oliver TB, Marks RC, Leonard RC (2001) Osteonecrosis of the femoral head following adjuvant chemotherapy for breast cancer. Breast 10:447–449
Tarassoff P, Csermak K (2003) Avascular necrosis of the jaws: risk factors in metastatic cancer patients. J Oral Maxillofac Surg 61:1238–1239
Kluth EV, Jain PR, Stuchell RN, Frich JC Jr (1988) A study of factors contributing to the development of osteoradionecrosis of the jaws. J Prosthet Dent 59:194–201
Curi MM, Dib LL (1997) Osteoradionecrosis of the jaws: a retrospective study of the background factors and treatment in 104 cases. J Oral Maxillofac Surg 55:540–544 (Discussion 545–546)
Reuther T, Schuster T, Mende U, Kubler A (2003) Osteoradionecrosis of the jaws as a side effect of radiotherapy of head and neck tumour patients-a report of a thirty year retrospective review. Int J Oral Maxillofac Surg 32:289–295
Robinson NA, Yeo JF (2004) Bisphosphonates-a word of caution. Ann Acad Med Singapore 33:48–49
Wagner W, Kuffner HD, Hartmann U (1986) Der bestrahlte Patient als Risikopatient bei zahnärztlich—chirurgischen Eingriffen. Dtsch Zahnarztl Z 41:440–443
Hoskin PJ (2003) Bisphosphonates and radiation therapy for palliation of metastatic bone disease. Cancer Treat Rev 29:321–327
Algur E, Macklis RM, Hafeli UO (2005) Synergistic cytotoxic effects of zoledronic acid and radiation in human prostate cancer and myeloma cell lines. Int J Radiat Oncol Biol Phys 61:535–542
Schwartz HC (2004) Osteonecrosis and bisphosphonates: correlation versus causation. J Oral Maxillofac Surg 62:763–764
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Walter, C., Grötz, K.A., Kunkel, M. et al. Prevalence of bisphosphonate associated osteonecrosis of the jaw within the field of osteonecrosis. Support Care Cancer 15, 197–202 (2007). https://doi.org/10.1007/s00520-006-0120-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-006-0120-z