
Abstract
Aside from climatic factors, the impact of heat waves on mortality depends on the demographic and socio-economic structure of the population as well as variables relating to local housing. Hence, this study’s main aim was to ascertain whether there might be a differential impact of heat waves on daily mortality by area of residence. The study is a time-series analysis (2000–2009) of daily mortality and minimum and maximum daily temperatures (°C) in five geographical areas of the Madrid region. The impact of such waves on heat-related mortality due to natural causes (ICD-10: A00- R99), circulatory causes (ICD-10: I00-I99) and respiratory causes (ICD-10: J00-J99) was obtained by calculating the relative risk (RR) and attributable risk (AR), using GLM models with the Poisson link and controlling for trend, seasonalities and the autoregressive nature of the series. Furthermore, we also evaluated other external variables, such as the percentage of the population aged over 65 years and the percentage of old housing. No heat-related mortality threshold temperature with statistical significance was detected in the northern and eastern areas. While the threshold temperatures in the central and southern areas were very similar and close to the 90th percentile, the threshold in the western area corresponded to the 97th percentile. Attributable mortality proved to be highest in the central area with 85 heat wave-related deaths per annum. External factors found to influence the impact of heat on mortality in Madrid were the size of the population aged over 65 years and the age of residential housing. Demographic structure and the percentage of old housing play a key role in modulating the impact of heat waves. This study concludes that the areas in which heat acts earliest are those having a higher degree of population ageing.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Globally, the planet’s temperature has risen by 0.60 °C over the course of the twentieth century. (Nicholls and Lavery 1996). In 2003, record maximum temperatures were registered across Europe (Schär et al. 2004; Díaz et al. 2005; Martínez et al. 2004), which coincided with episodes of high pollution and posed a serious threat to the population at risk (Lee and Sheridan 2018)—fundamentally the age segment over 65 years (Díaz and Linares 2008; Takeda et al. 2016; Ma et al. 2017; Díaz et al. 2002; Jimenez et al. 2011)—causing an increase in mortality of historic proportions (Robine et al. 2008,Martínez et al. 2004).
Aside from factors of a purely climatic nature, the impact of heat on mortality is modulated by socio-economic, demographic, environmental and temperature-adaptation variables (Alberdi et al. 1998; Barrett 2015; Khaw 1995; Gosling et al. 2009; Konkel 2014; Guo et al. 2014). Moreover, these factors are not static but, like extreme temperatures and heat waves in particular, tend to vary over time. In this respect, an increase is expected in the frequency and intensity of future heat waves, boosted by the heat island effect, with intense effects in southern Europe (IPCC 2013, Fernández et al. 2016, Li et al. 2015, Linares et al. 2017, Santos and de Lara 2008), accompanied by a prolongation of summer months and a late, abrupt onset of winter (Brunetti et al. 2000; WHO 2008; Byford 2014).
In the face of an increase in extreme meteorological phenomena, adaptation strategies are clearly crucial in minimising the health impact of heat waves; and in the context of such adaptation strategies, heat wave prevention plans are showing themselves to be effective (Díaz et al. 2018; Mayrhuber et al. 2018).
The heat wave prevention plan currently in force in Spain takes these differences into account at a provincial level, by calculating the temperature above which a heat wave is defined for each province (Díaz et al. 2015a, b), rather than assuming a constant percentile across the board. Despite this significant advance, however, there are different climatic regions within each province, something that calls for the implementation of prevention plans on a scale that is smaller than the provincial, an example being the plan proposed for Madrid (Carmona et al. 2017), based on the definition of existing different isoclimatic areas. Evidently, it is not the climatic component alone which must be considered. Extreme-temperature adaptation strategies must be pursued at a local level. Factors such as the existence of adequate home infrastructures (Sanz et al. 2016; Bittner et al. 2014), green areas (Xu et al. 2013), energy poverty, income level (Sanz et al. 2016) and even the intensity of the heat island effect (Wilby et al. 2011) can modify the impact of high temperatures on daily mortality.
This study was thus an exploratory, ecological, retrospective study, whose main aim was to ascertain whether there might be a different mortality behaviour pattern between surrounding towns and the city centre in response to extremely high-temperature events.
Material and methods
Determination of geographical areas and dependent and independent variables
The study included towns situated within a radius of 30 km. from the Puerta de Sol (Madrid city centre) having a population of 10,000 inhabitants or more. These towns were classified by compass bearing into five groups, ‘north’, ‘south’, ‘east’ and ‘west’, with the fifth group, “centre”, being made up of the city of Madrid (Fig. 1).

Location meteorological observatories, according to zones, used in the study
For each of the towns making up the respective groups, we took daily mortality recorded from 1 January 2000 to 31 December 2009 as the dependent variable. This information was obtained from microfiches containing death data supplied under a data-loan agreement by the National Statistics Institute (Instituto Nacional de Estadística/INE) to the Carlos III Institute of Health (Instituto de Salud Carlos III) (INE, 2018a, b). Mortality was classified for each group according to the International Classification of Diseases, 10th Revision (ICD-10) as follows: deaths due to natural causes (ICD-10: A00-R99), and within these, deaths due to respiratory causes (ICD-10: J00-J99) and cardiovascular causes (ICD-10: I00-I99).
The independent variables were the minimum and maximum daily temperature series, as measured at the observatories of Tres Cantos (north), Barajas (east), Getafe (south), Cuatro Vientos (west) and Retiro (centre). The observatories representative of the respective areas were identified and the minimum and maximum daily temperature series were furnished by the State Meteorological Agency (Agencia Estatal de Meteorología/AEMET).
Determination of daily mortality trigger threshold temperatures
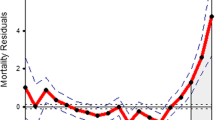
We determined the heat-related mortality threshold temperature (Tthreshold) for each area, since this represents the temperature above which there is a statistically significant increase in temperature-related mortality. This threshold was determined with the aid of scatterplot diagrams showing mortality residuals and minimum and maximum daily temperatures (grouped by intervals). The residuals were obtained using ARIMA modelling of the daily mortality series in each group (Kent et al. 2014; Montero et al. 2010; Mirón et al. 2006; Díaz et al. 2015a, b; Sánchez-Martínez et al. 2018).
Based on this Tthreshold, for each group, we calculated the variable Theat, which takes into account the fact that minimum and maximum daily temperature differ from Tthreshold in the following way in the case of the maximum (Díaz et al. 2015b):
The advantage of calculating the Tthreshold for each group is that, in addition to purely climatic factors, it also includes factors of a local nature. Furthermore, such a Tthreshold will correspond to different percentiles of the minimum and maximum daily temperature series at each group’s designated observatory, and will thus be the right temperature for ascertaining precisely when to define the impact of a heat wave in any given area.
It is well known that the effect of heat may manifest itself after some time has passed (Li et al. 2015), with the ability to affect cardiovascular-cause mortality at a lag of as much as 3 days, and up to 5 days in the case of respiratory diseases (Alberdi and Diaz 1997). We therefore included the lagged variables Theat1, Theat2, Theat3, Theat4 and Theat5 for each of the two definitions of Tthreshold.
Modelling process
To quantify the impact of heat waves on daily mortality due to natural, circulatory and respiratory causes, generalised linear models (GLMs) with the Poisson link were fitted for each Tthreshold value in each group for the period from May to June, with the Theat variables being introduced at the corresponding lags. The trend was controlled for by introducing a count variable denominated n1, and defined as n1 = 1 for the first day of the series, n1 = 2 for the second and so on. We controlled for seasonalities by introducing sine and cosine functions with four- and three-monthly periodicities. Similarly, the autoregressive nature of the series was controlled for by including first-order autoregressive parameters in the various models.
To obtain the final models, we used the backward stepwise method, retaining all variables with a p value < 0.05, and to select the final model, the Akaike and Bayesian information criteria were also applied.
Lastly, the relative risks (RRs) were calculated using the significant values of the relevant Theat estimators.
Calculation of attributable mortality
Attributable mortality was calculated on the basis of the percentage of attributable risk (AR), i.e. the estimated proportion of mortality which, for any given degree, is related to exposure to Theat (Coughlin et al. 1996), and which is in turn is related to the RR via the following expression (Coste and Spira 1991):
Heat wave-related mortality throughout the period was calculated as proposed by Tobías et al. 2015, namely, by multiplying the AR by total mortality broken down by group, and dividing this by 100. This figure is then divided by 10, the number of years covered by the time series, to obtain the heat wave-related mortality corresponding to an annual value.
Analysis of non-climatic variables
In addition, we analysed the population at risk and the age of housing, i.e. predating 1980, to observe the existence of patterns concordant with the threshold temperatures detected. The percentage of the population at risk was calculated on the basis of data on the population segment aged over 65 years (INE 2018a, b) and the total population by town (INE 2014). The percentage of old housing was calculated using records with a breakdown by date of statistics on housing conditions drawn up by the Madrid Regional Statistics Institute (Instituto Regional de Estadística 2006). To observe differences between groups, we used Generalised Linear Mixed Models (GLMMs) that included random effects associated with towns, taking the percentage of the population at risk and old housing as the dependent variable, and the group to which the town was assigned as the independent variable.
All analyses were performed using the SPSS 13 time-series package, Stata 15 and R.
Results
Table 1 shows the descriptive values of the variables used. In general, all areas were climatically very similar. Closer examination shows that the maximum daily temperatures were less extreme in Madrid than on the city outskirts, i.e. at least 1° lower for the third quartile and 2° lower for the maximum values. In contrast, minimum daily temperatures were somewhat warmer in central Madrid than in towns in the remaining groups, with mean temperatures in the centre being 0.6° to 2.2 °C warmer than in the outlying areas.
Furthermore, the central area registered a mean of 53 to 64 deaths more per day than did the outskirts, 4 to 9 persons more in the case of respiratory-cause mortality, and 14 to 17 more in the case of circulatory-cause mortality.
By way of example, Fig. 2 shows the scatterplot diagrams plotted with the maximum daily temperatures for the central, southern and western areas, the only ones in which this threshold temperature could be ascertained. If the minimum instead of the maximum daily temperature is used, the results are very similar, except in the case of the western area, where the threshold temperature could only be determined using the maximum, but not the minimum, daily temperature. These threshold temperatures and the percentiles to which they correspond in the minimum and maximum daily temperature series are shown in Table 2.

Scatter-plot to calculate the threshold temperature according to zone
Table 3 shows the impact of heat waves by reference to RR, AR and annual heat wave-related mortality. Although there were no significant differences in RRs between areas experiencing the effect of heat on mortality, the highest relative risks were registered for the west, namely, the area that had a threshold temperature corresponding to the highest percentile. These RRs corresponded to ARs of 19.09% (5.34–30.84) for the western area, 8.66% (1.45–15.34) for the central area and 13.65% (3.37–22.84) for the southern area. Heat-related mortality was higher in the centre and south, which are the most densely populated areas. Despite the similarity of the RRs for the two specific causes considered, heat-related mortality was nevertheless greater for circulatory than for respiratory causes.
The descriptive statistics of the external variables considered (Table 4) show that the centre had a mean of 10 to 12% more over-65-year-olds than did the outlying areas. Among the groups of outlying towns, it was the south that had the most aged population (mean of 9%), with persons over the age of 65 accounting for 12 to 13% of the population in towns having most persons at risk. Lying at the opposite extreme was the eastern area, with a mean over-65 population of 7%. Insofar as the age of housing was concerned, the outskirts had approximately 30% fewer pre-1980 dwellings than did the centre, with the west of Madrid being the area with the lowest mean stock of old housing (30.8%), and the south being the area with towns having the highest stocks of such housing (40.8 to 52.6%).
Table 5 shows the results of the GLM models with random effects, fitted for the percentage of population at risk and the percentage of old housing. In the former case, significant differences were found between the over-65-year-olds in the northern versus the southern and central areas; in the latter case, significant differences were found between the age of housing in the northern and central areas.
Discussion
As will be seen from Table 1, at the upper extreme of the maximum daily temperatures for Madrid city centre, temperatures are reached that are generally less elevated than those on the city outskirts. When it comes to minimum daily temperatures, however, the temperature in the central area of Madrid is higher than that in the remaining areas, a finding that goes to ratify the fact that, in cities, the heat-island effect (Milojevic et al. 2016) is to be found in the minimum rather than the maximum daily temperatures (Wilby et al. 2011). Moreover, this heat-island effect is less pronounced than that reported by other studies for the city of Madrid (Fernández et al. 2016). The fact that the contrast between temperatures is not any greater is due to the fact that all the observatories and towns included in this study were urban in nature (Consejería de Medio Ambiente de la CM 2006), whereas this effect has traditionally been described in comparisons between urban and outlying rural areas (Fernández et al. 2016).
Table 2 shows that, whereas no temperature threshold was detected in the western area when the minimum daily temperature was considered, it was detected when the maximum daily temperature was used. This would indicate that maximum daily temperatures are more closely linked to heat-related mortality phenomena (Díaz et al. 2015b), and would account for the fact that they enabled Tthreshold to be detected in one more group than did minimum daily temperatures. These results are in line with those obtained by Guo et al. 2017 in a study covering 400 cities in 19 countries, according to which mean or maximum daily temperatures are better indicators than minimum daily temperature for evaluating the impact of heat on daily mortality.
The values of these threshold temperatures agree with those obtained in the isoclimatic zoning performed by previous studies for the entire province of Madrid (Carmona et al. 2017). The differences observed with respect to Carmona’s study are due to the different areas considered and to the different location of the temperature-monitoring observatories.
With respect to the relative risks shown in Table 3, it should be noted that the differences among them are not statistically significant, though the highest RRs were found in the west, an area where the threshold temperature of 38 °C corresponded to the 97.5th percentile of the maximum daily temperature series. This finding is in line with what has been reported by other studies in Spain, in which high percentiles of the mortality threshold temperature are associated with high RRs (Díaz et al. 2015b). The higher mortality attributable to the city centre is due to the fact that it is here where daily mortality is highest.
As for the specific causes of mortality, in accordance with the relative risks, the impact of heat proved to be similar for both causes of mortality considered, a result that agrees with those obtained by other studies undertaken in Madrid (Alberdi et al. 1998; Díaz et al. 2002, 2015b). As can be seen yet again in Table 1, daily mortality due to circulatory causes is higher than that due to respiratory causes, leading by extension to heat-related mortality being higher for circulatory causes.
On analysing the Tthreshold values and their percentiles in Table 2 along with the results yielded by the analysis of non-climatic variables in Table 4, a pattern emerges which helps one understand how the impact of heat waves is being modulated in the centre and outskirts of Madrid. One of the factors responsible is the population aged over 65 years, which is the group most sensitive to the effects of heat (Takeda et al. 2016; Ma et al. 2017; Díaz et al. 2002; Jimenez et al. 2011; Montero et al. 2012; Díaz et al. 2015b). Table 2 shows that the areas where the threshold temperatures lie in the lowest percentiles (south and centre)—under the 90th percentile in both cases (88.9th and 89.9th respectively)—are where the population at risk is significantly larger than in the northern area of Madrid (Table 5). The fact that these populations comprise a great proportion of the populace sensitive to heat waves means that the temperatures required for observing a statistically significant mortality threshold are lower.
Moreover, these factors converge in the city centre, the area having the single greatest component of old housing, a feature that makes it significantly different from the northern area. Although significant differences are not observed between outlying areas vis-à-vis the north, the descriptive analysis nonetheless shows that the outlying towns possessing stocks of the oldest housing are to be found to the south of Madrid. The relevance of this lies in the fact that the degree of home conservation, housing-material quality, thermal insulation and air conditioning and heating systems have been shown to play a pivotal role in modulating the effects of heat and cold waves (Sanz et al. 2016; Bittner et al. 2014).
By virtue of its being an ecological study, one of this study’s limitations is that the results are only valid at a population level (ecological fallacy). Similarly, on being a retrospective study, these results could currently amount to an underestimate of the real impact of heat waves given the trend in climate and the impact that the economic crisis might have had on access to air conditioning systems, home maintenance, energy poverty or any other of the non-climatic variables that modulate the impact of heat.
Among the factors that amplify the urban heat island effect are household characteristics such as the age of buildings, residence in the highest floor of a building, the presence of a bedroom immediately beneath the roof (due to the concentration of heat that accumulates during the day and later irradiation during the night) and lack of good thermal isolation (Vandentorren et al. 2006). On the other hand, environmental factors have been found such as proximity to green space, locations with water or the coast that mitigate the impact of heat waves in urban places (after these variables are adjusted for socio-economic factors) (Burkart et al. 2016). Combatting the effects of heat islands in cities means adopting measures and adaptation strategies, including increasing plant coverage inside cities, increasing water covers and using fresh pavements.
In addition, this study is affected by the problem of discordance between the geographical situation of the AEMET observatories and the areas where the impact of temperature was analysed. Although relative humidity and atmospheric pressure are known to modulate the effect of heat, these were not controlled for, in view of their insignificant influence on the temperature-mortality relationship reported by previous studies (Mirón et al. 2006; Roldán et al. 2011). The lack of data made it impossible to control for heat wave impact due to non-climatic variables, such as socio-economic data or lifestyle. Furthermore, no adjustment was made for sex or age range, both of which could play an effect-modifier role (Vodonos et al. 2015; Barceló et al. 2016; Díaz et al. 2006).
In this study air pollution levels were not taken into account because validated data were not available at this level of spatial disaggregation. There have been few studies that address the issue of synergy between meteorology and pollution and the effects on health. Among the reported studies, most have investigated hot weather rather than cold weather. Some studies have reported effects of temperature modified by pollutants, and some have reported effects of pollutants modified by temperature. However, although the interaction was the same in statistical terms, the results reported did not always allow comparisons of the magnitude of effects. Sartor et al. (Sartor et al. 1997) and Díaz et al. (Díaz et al. 2002) reported synergy with ozone; Parodi et al.(Parodi et al. 2005) and Ren et al. (Ren et al. 2006) also reported synergy between temperature and ozone exposure for effects on cardiovascular mortality. In a study in Germany, Breitner et al. reported effect modification in the temperature–mortality association by O3 (Breitner et al. 2014).
However, the values of the ARs obtained in this study with a heat wave definition based on threshold temperature are very similar to those obtained for the province of Madrid in a study which was conducted for Spain as a whole (Díaz et al. 2015a) with an AR of 6.7%, and did take air pollution into account. This is in line with other studies which indicate that the fact of taking or not taking air pollution into account in temperature-mortality models does not change the trend in the results found (Bobb et al. 2014; Carson et al. 2006). That said, however, the use of minimum daily temperature obtained at a single observatory as an indicator of exposure for the entire province poses a bias which will have to be considered in future research (Carmona et al. 2017).
Strategies for combating climate change must be designed from a stance of mitigation and adaptation. The level of adaptation to heat waves is explained in large part by six levels of intervention of adaptation, which include individual, interpersonal, community, institutional, environmental and public policy levels as can be observed in the figure below. These adaptation interventions are capable of changing human physiology and behaviour and affect the impact of high temperatures. The details of this process are complex and not fully understood, but they include changes in physiology (for example, increases in central temperature), behaviour changes (for example, time spent in fresh air, clothing, physical activity, healthy lifestyles), improvements in health services and environmental improvements (for example, thermal properties and the nature of the built environment, including building design and city planning) (Guo et al. 2018).
This study highlights the fact that in adaptation strategies, local factors play a highly important role which can effectively modulate the impact of heat on mortality.
References
Alberdi J, Diaz J (1997) Modelización de la mortalidad diaria en la Comunidad Autónoma de Madrid (1986-1991). Gac Sanit 11(1):9–15 https://www.sciencedirect.com/science/article/pii/S0213911197712664
Alberdi JC, Díaz J, Montero C, Mirón I (1998) Daily mortality in Madrid community 1986-1992: relationship with meteorological variables. Eur J Epidemiol 14:571–578 https://springerlink.bibliotecabuap.elogim.com/article/10.1023/A:1007498305075
Barceló MA, Varga D, Tobias A, Diaz J, Linares C, Saez M (2016) Long term effects of traffic noise on mortality in the city of Barcelona, 2004-2007. Environ Res 147:193–206. https://doi.org/10.1016/j.envres.2016.02.010
Barrett J (2015) Increased minimum mortality temperature in France: data suggest humans are adapting to climate change. Environ Health Perspect 123(7):A 184 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4492254/
Bittner MI, Matthies EF, Dalbokova D, Menne B (2014) Are European countries prepared for the next big heat-wave? Eur J Pub Health 24(4):615–619. https://doi.org/10.1093/eurpub/ckt121
Bobb JF, Peng RD, Bell ML, Dominici F (2014) Heat-related mortality and adaptation to heat in the United States. Environ Health Perspect 122(8):811–816
Breitner S, Wolf K, Devlin RB, Diaz-Sanchez D, Peters A, Schneider A (2014) Short-term effects of air temperature on mortality and effect modification by air pollution in three cities of Bavaria, Germany: a time-series analysis. Sci Total Environ 485-486:49–61
Brunetti M, Maugeri M, Nanni T (2000) Variations of temperature and precipitation in Italy from 1866 to 1995. Theor Appl Climatol 65(3–4):165–174. https://doi.org/10.1007/s007040070041
Burkart K, Meier F, Schneider A, Breitner S, Canário P, Alcoforado MJ, Scherer D, Endlicher W (2016) Modification of heat-related mortality in an elderly urban population by vegetation (urban green) and proximity to water (urban blue): evidence from Lisbon, Portugal. Environ Health Perspect 124(7):927–934
Byford T (2014) Protecting health in Europe from climate change. Int J Environ Stud 71(3):410–411. https://doi.org/10.1080/00207233.2014.914678
Carmona R, Linares C, Ortiz C, Mirón IJ, Luna MY, Díaz J (2017) Spatial variability in threshold temperatures of heat wave mortality: impact assessment on prevention plans. Int J Environ Health Res 3123:1–13. https://doi.org/10.1080/09603123.2017.1379056
Carson C, Hajat S, Armstrong B, Wilkinson P (2006) Declining vulnerability to temperature-related mortality in London over the 20th century. Am J Epidemiol 164(1):77–84
Consejería de Medio Ambiente de la Comunidad de Madrid (2006) Comunidad de Madrid, Administración Local y Ordenación del Territorio. https://gestiona.madrid.org/azul_internet/html/web/3_1.htm?ESTADO_MENU=3_1
Coste J, Spira A (1991) Le proportion de cas attributable en Santé Publique: definition, estimation et interpretation. Rev Epidemiol Sante Publique 51:399–411
Coughlin S, Benichou J, Douglas W (1996) Estimación del riesgo atribuible en los estudios de casos y controles. Bol Oficina Sanit Panam 121(2):143–185
Díaz J, Linares C (2008) Temperaturas extremadamente elevadas y su impacto sobre la mortalidad diaria de acuerdo a diferentes grupos de edad. Gac Sanit 22:115–119 https://www.sciencedirect.com/science/article/pii/S0213911108712172
Díaz J, Jordán A, García R, López C, Alberdi JC, Hernández E, Otero A (2002) Heat waves in Madrid 1986-1997: effects on the health of the elderly. Int Arch Occup Environ Health 75(3):163–170. https://doi.org/10.1007/s00420-001-0290-4
Díaz J, García R, López C, Linares C, Tobías A, Prieto L (2005) Mortality impact of extreme winter temperatures. Int J Biometeorol 49(3):179–183. https://doi.org/10.1007/s00484-004-0224-4
Díaz J, Linares C, Tobías A (2006) Impact of extreme temperatures on daily mortality in Madrid (Spain) among the 45-64 age-group. Int J Biometeorol 50(6):342–348. https://doi.org/10.1007/s00484-006-0033-z
Díaz J, Carmona R, Linares C (2015a) Temperaturas umbrales de disparo de la mortalidad atribuible al calor en España en el periodo 2000–2009. Instituto de Salud Carlos III, Escuela Nacional de Sanidad, Madrid
Díaz J, Carmona R, Mirón IJ, Ortiz C, León I, Linares C (2015b) Geographical variation in relative risks associated with heat: update of Spain’s heat wave prevention plan. Environ Int 85:273–283. https://doi.org/10.1016/j.envint.2015.09.022
Díaz J, Carmona R, Mirón IJ, Luna MY, Linares C (2018) Time trend in the impact of heat waves on daily mortality in Spain for a period of over thirty years (1983-2013). Environ Int 116:10–17
Fernández F, Allende F, Alcaide J, Rasilla D, Martilli A, Alcaide J (2016) Estudio de detalle del clima urbano de Madrid. Ayuntamiento de Madrid, Área de Gobierno de Medio Ambiente y Movilidad, Dirección General de Sostenibilidad y Control Ambiental - Universidad Autónoma de Madrid, Departamento de Geografía, Madrid http://www.madrid.es/UnidadesDescentralizadas/Sostenibilidad/EspeInf/EnergiayCC/04CambioClimatico/4cEstuClimaUrb/Ficheros/EstuClimaUrbaMadWeb2016.pdf
Gosling SN, McGregor GR, Lowe JA (2009) Climate change and heat-related mortality in six cities part 2: climate model evaluation and projected impacts from changes in the mean and variability of temperature with climate change. Int J Biometeorol 53(1):31–51. https://doi.org/10.1007/s00484-008-0189-9
Guo Y, Gasparrini A, Armstrong B, Li S, Tobias A, Lavigne E, Stagliorio Z (2014) Global variation in the effects of ambient temperature on mortality: a systematic evaluation. Epidemiology 25(6):781–789 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4180721/
Guo Y, Gasparrini A, Armstrong BG, Tawatsupa B, Tobias A, Lavigne E, Coelho MSZS et al (2017) Heat wave and mortality: a multicountry, multicommunity study. Environ Health Perspect 125(8):087006. https://doi.org/10.1289/EHP1026
Guo Y, Gasparrini A, Li S, Sera F, Vicedo-Cabrera AM, de Sousa Zanotti Stagliorio Coelho M et al (2018) Quantifying excess deaths related to heatwaves under climate change scenarios: a multicountry time series modelling study. PLoS Med 15(7):e1002629
INE (2014) Proyección de la Población de España 2014-2064: Notas de prensa. Instituto Nacional de Estadística (INE), 1–9. Retrieved from: http://www.ine.es/prensa/np870.pdf
INE (2018a) Estadística del Padrón Continuo a 1 de enero de 2011. Datos por municipios. Instituto Nacional de Estadística, España Retrieved from: http://www.ine.es/jaxi/Tabla.htm?path=/t20/e245/p05/a2011/l0/&file=00028001.px&L=0
INE (2018b) Cifras oficiales de población resultantes de la revisión del Padrón municipal a 1 de enero. Instituto Nacional de Estadística, España http://www.ine.es/jaxiT3/Tabla.htm?t=2881&L=0
Instituto Regional de Estadística (2006) Edificios. Indicadores Municipales de la Comunidad de Madrid. Madrid: http://www.madrid.org/iestadis/fijas/estructu/general/territorio/iindimuni06.htm
IPCC (2013) Climate change 2013: the physical science basis. Working group I contribution to the fifth assessment report of the intergovernmental panel on climate change. http://www.climatechange2013.org/
Jimenez E, Linares C, Martinez D, Diaz J (2011) Particulate air pollution and short-term mortality due to specific causes among the elderly in Madrid (Spain): seasonal differences. Int J Environ Health Res 21(5):372–390. https://doi.org/10.1080/09603123.2011.560251
Kent ST, McClure LA, Zaitchik BZ, Smith TT, Gohlke JM (2014) Heat waves and health outcomes in Alabama (USA): the importance of heat wave definition. Environ Health Perspect 122(2):151–159 Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3914868/
Khaw K (1995) Temperature and cardiovascular mortality. Lancet 345:337–338 https://www.sciencedirect.com/science/article/pii/S0140673695903364
Konkel L (2014) Learning to take the heat declines in U.S. Heat-related mortality Americans. Environ Health Perspect 122(8):A 202. https://doi.org/10.1289/ehp.1307392.2
Lee C, Sheridan SC (2018) A new approach to modeling temperature-related mortality: non-linear autoregressive models with exogenous input. Environ Res 164:53–64. https://doi.org/10.1016/j.envres.2018.02.020
Li M, Gu S, Bi P, Yang J, Liu Q (2015) Heat waves and morbidity: current knowledge and further direction: a comprehensive literature review. Int J Environ Res Public Health 12(5):5256–5283. Retrieved from. https://doi.org/10.3390/ijerph120505256
Linares C, Carmona R, Ortiz CD (2017) Temperaturas extremas y Salud. Editorial La Catarata, Madrid
Ma T, Xiong J, Lian Z (2017) A human thermoregulation model for the Chinese elderly. J Therm Biol 70:2–14. https://doi.org/10.1016/j.jtherbio.2017.08.002
Martínez F, Simón-Soria F, López-Abente G (2004) Valoración del impacto de la ola de calor del verano de 2003 sobre la mortalidad. Gac Sanit 18(Supl 1):250–258 http://www.gacetasanitaria.org/es/valoracion-del-impacto-ola-calor/articulo/13062535/
Mayrhuber EA, Dückers MLA, Wallner P, Arnberger A, Allex B, Wiesböck L et al (2018) Vulnerability to heatwaves and implications for public health interventions—a scoping review. Environ Res 166:42–54
Milojevic A, Armstrong BG, Gasparrini A, Bohnenstengel SI, Barratt B, Wilkinson P (2016) Methods to estimate acclimatization to urban heat island effects on heat- and cold-related mortality. Environ Health Perspect 124(7):1016–1022
Mirón IJ, Montero JC, Criado-Álvarez JJ, Gutierrex G, Paredes D, Mayoral Arenas S, Linares C (2006) Tratamiento y estudio de series de temperatura para su aplicación en salud pública. El caso de Castilla La Mancha. Rev Esp Salud Pública 80(2):113–124 http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1135-57272006000200002
Montero JC, Mirón IJ, Criado JJ, Linares C, Díaz J (2010) Comparison between two methods of defining heat waves: a retrospective study in Castile-La Mancha (Spain). Sci Total Environ 408(7):1544–1550. https://doi.org/10.1016/j.scitotenv.2010.01.013
Montero JC, Mirón IJ, Criado JJ, Linares C, Díaz J (2012) Influence of local factors in the relationship between mortality and heat waves: Castile-La Mancha (1975-2003). Sci Total Environ 414:73–80. https://doi.org/10.1016/j.scitotenv.2011.10.009
Nicholls N, Lavery B (1996) Recent apparent changes in relationships between the El Niño-southern oscillation and Australian rainfall and temperature. Geophys Res Lett 23:3357–3360
Parodi S, Vercelli M, Garrone E, Fontana V, Izzotti A (2005) Ozone air pollution and daily mortality in Genoa, Italy between 1993 and 1996. Public Health 119(9):844–850
Ren C, Williams GM, Tong S (2006) Does particulate matter modify the association between temperature and cardiorespiratory diseases? Environ Health Perspect 114(11):1690–1696
Robine JM, Cheung SLK, Le Roy S, Van Oyen H, Griffiths C, Michel JP, Herrmann FR (2008) Death toll exceeded 70,000 in Europe during the summer of 2003. C R Biol 331(2):171–178. https://doi.org/10.1016/j.crvi.2007.12.001
Roldán E, Gómez M, Pino MR, Esteban M, Díaz J (2011) Determinación de zonas isoclimáticas y selección de estaciones meteorológicas representativas en Aragón como base para la estimación del impacto del cambio climático sobre la posible relación entre la mortalidad y temperatura. Rev Esp Salud Pública 85:603–610
Sánchez-Martínez G, Díaz J, Linares C, Nieuwenhuyse A, Hooyberghs H, Lauwaet D, De Ridder K, Carmona R, Ortiz C, Kendrovski V, Aerts R, Dunbar M (2018) Heat and health under climate change in Antwerp: projected impacts and implications for prevention. Environ Int 111:135–143
Santos E, de Lara P (2008) Método de regionalización de temperaturas basado en análogos. Explicación y validación. Agencia Estatal de Meteorología. http://www.aemet.es/documentos/es/idi/clima/escenarios_CC/Metodo_regionalizacion_temperatura.pdf
Sanz A, Gómez G, Sánchez-Guevara C, Núñez M (2016) Estudio técnico sobre pobreza energética en la ciudad de Madrid. Ecologistas en Acción, Madrid http://www.madrid.es/UnidadesDescentralizadas/Consumo/NuevaWeb/pobreza%20energ%C3%A9tica/Estudio%20Pobreza%20energ%C3%A9tica%204%20febrero%202017.pdf
Sartor F, Demuth C, Snacken R, Walckiers D (1997) Mortality in the elderly and ambient ozone concentration during the hot summer, 1994, in Belgium. Environ Res 72(2):109–117
Schär C, Vidale PL, Lüthi D, Häberli C, Liniger MA, Appenseller C (2004) The role of increasing temperature variability in European summer heatwaves. Nature 427(6972):332. https://www.nature.com/articles/nature02300–336
Takeda R, Imai D, Suzuki A, Ota A, Naghavi N, Yamashina Y, Okazaki K (2016) Lower thermal sensation in normothermic and mildly hyperthermic older adults. Eur J Appl Physiol 116(5):975–984. https://doi.org/10.1007/s00421-016-3364-4
Tobías A, Recio A, Díaz J, Linares C (2015) Health impact assessment of traffic noise. Environ Res 137:136–140
Vandentorren S, Bretin P, Zeghnoun A, Mandereau-Bruno L, Croisier A, Cochet C, Ribéron J, Siberan I, Declercq B, Ledrans M (2006) August 2003 heat wave in France: risk factors for death of elderly people living at home. Eur J Pub Health 16(6):583–591
Vodonos A, Friger M, Katra I, Krasnov H, Zahger D, Schwartz J, Novack V (2015) Individual effect modifiers of dust exposure effect on cardiovascular morbidity. PLoS One 10(9):1–12. https://doi.org/10.1371/journal.pone.0137714
WHO (2008) Protecting health in Europe from climate change. Copenhagen. http://www.euro.who.int/__data/assets/pdf_file/0016/74401/E91865.pdf?ua=1
Wilby R, Jones P, Lister D (2011) Decadal variations in the nocturnal heat island of London. Weather 66(3):59–64
Xu Y, Dadvand P, Barrera-Gomez J, Sartini C, Mari-Dell’Olmo M, Borrell C, Medina-Ramón M, Sunyer J, Basagaña X (2013) Differences on the effect of heat waves on mortality by sociodemographic and urban landscape characteristics. J Epidemiol Community Health 67(6):519–525
Acknowledgement of funding
The authors gratefully acknowledge Project ENPY 1133/16 Project ENPY 376/18 and Project ENPY 107/18 grants from the Carlos III Institute of Health.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclaimer
This paper reports independent results and research. The views expressed are those of the authors and not necessarily those of the Carlos III Institute of Health (Instituto de Salud Carlos III).
Rights and permissions
About this article

Cite this article
López-Bueno, J.A., Díaz, J. & Linares, C. Differences in the impact of heat waves according to urban and peri-urban factors in Madrid. Int J Biometeorol 63, 371–380 (2019). https://doi.org/10.1007/s00484-019-01670-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-019-01670-9