
Abstract
Background
The management of steroid-sensitive nephrotic syndrome (SSNS) requires treatment with high-dose glucocorticoids (GCs), but GC usage causes the most frequent form of drug-induced osteoporosis. The aim of our study was to evaluate the impact of GCs on bone mineralization in patients with SSNS using two diagnostic tools, dual-energy X-ray densitometry (DXA) and quantitative ultrasound (QUS), and to compare the diagnostic efficacy of these two imaging tools.
Methods
A total of 30 children with SSNS (age 5.20 ± 2.20 years) were evaluated at the start (T0) and after 1 (T1), 2.44 ± 0.75 (T2, 18 patients) and 5.96 ± 2.33 years (T4, 12 patients) of GC treatment. Patients who stopped at T2 were also evaluated at the 1-year timepoint after ceasing GC treatment (T3).
Results
Of the patients assessed at T2, 11 had bone mineralization at the lower limit of normal versus those at T0 and T1, with bone mineralization rescue at the 1-year timepoint after GC discontinuation. At T4, 6/12 patients had densitometric parameters at the lower limit of normal values, and 3/12 patients showed reduced bone mineralization. The parameters derived from measurements of DXA and QUS were significantly related to each timepoint.
Conclusions
Patients with SSNS receiving GC therapy undergo bone status alteration related to the dosage and duration of the therapy. In terms of diagnostic efficacy, DXA and QUS were comparable, indicating that QUS is a reliable tool to evaluate bone health in children with SSNS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Childhood steroid-sensitive nephrotic syndrome (SSNS) is a kidney disease which promptly responds to high-dose glucocorticoid (GC) therapy, with the patient going into complete remission within 30 days. Unfortunately, the majority of children with SSNS relapse when the GC dose is reduced, resulting in protracted, repeated courses of GCs. The standard prednisone dose for relapses is 60 mg/m2/day, which far exceeds the daily dose of 5 mg considered to be a risk factor for GC-induced osteoporosis in adults [1]. Bone loss caused by GC therapy occurs in two ways: direct suppression of the activity of osteoblasts, the bone-forming cells, and increased bone resorption by osteoclasts, the bone-reabsorbing cells [2, 3]. While GCs at physiological doses appear to be essential for normal osteoblast differentiation, at high doses they diminish the number of osteoblasts by promoting apoptosis [4]. GCs have also been found to promote osteoclastogenesis in several pediatric diseases that require long-term GC treatment [5, 6]. This spontaneous osteoclastogenesis seems to be supported by both the presence of circulating osteoclast precursors and factors released by T cells, which have been recognized as key regulators of osteoclast and osteoblast formation and activity in different diseases [7]. The growing skeleton may be particularly vulnerable to the negative effects of long-term GC therapy on bone remodeling. In fact, GC therapy in children is associated with impaired linear growth and increased fracture rates [8]. A low incidence of vertebral fractures and an inverse correlation between lumbar spine bone mineral density (BMD) Z-scores at 12 months of treatment and early GC exposure, despite an absence of increased GC exposure, has recently been observed in children with nephrotic syndrome [9].
In addition, given the distinct effects of puberty and gender on trabecular and cortical bone, the structural implications of GC therapy may differ in pubertal and prepubertal children [10]. Indeed, if a full recovery from underlying disease is achieved prior to puberty, obviating the need for ongoing GC use, normalization of BMD may be possible [11]. To the contrary, patients who continue to receive long-term steroid therapy or those who are systematically treated with GCs during the years of pubertal development may not have similar potential for recovery of BMD [12].
Previous studies evaluating bone mineralization in patients with SSNS using dual-energy X-ray absorptiometry (DXA) showed modest deficits of bone mineral content (BMC) in the lumbar spine, but a greater BMC of whole body and an increase of femoral shaft dimensions [13, 14]. However, DXA provides two-dimensional (areal) values for BMD, does not distinguish cortical from trabecular bone and should be adjusted for height and weight when used for assessing children and adolescents. In contrast, studies performed using peripheral quantitative computed tomography (pQCT), which provides volumetric measures of BMD (vBMD) and geometry in both cortical and trabecular bone and, unlike DXA, does not need adjustment for body size have demonstrated that the effects of GC therapy in pediatric patients with SSNS are associated with a significantly greater cortical vBMD and cortical area and a lower trabecular vBMD, with evidence of low bone turnover and potential risk of fractures [15]. Such changes in trabecular and cortical vBMD and cortical dimensions in children with SSNS has been recently confirmed by Tsampalieros et al. [16], who also demonstrated that GC exposure is associated with decreases in biomarkers of bone formation, decreases in height Z-scores, increases in cortical vBMD Z-score and suppression of bone formation.
Quantitative ultrasound (QUS) is an easy, inexpensive and radiation-free diagnostic tool that can be used to evaluate bone mineral status. Its clinical applications for fracture risk assessment, diagnosis of osteoporosis, treatment initiation, monitoring of treatment and quality assurance/quality control has recently been addressed by The International Society for Clinical Densitometry (ISCD) 2007 Pediatric Position Development Conference [17]. QUS has been used to assess bone quality and fracture rate in children and adolescents with bone and mineral disorders [18, 19], evaluate bone turnover and bone osteopenia in the dialysis population and to monitor uremic osteodistrophy and secondary hyperparathyroidism [20], also in patients with subclinical hypothyroidism [21].
The aim of our study was to evaluate the impact of GC therapy on bone health in childhood SSNS and to compare two different diagnostic tools, namely DXA and QUS.
Material and methods
Study subjects
Children and adolescents with a diagnosis of SSNS, as defined by the International Society of Kidney Disease in Children [22], were identified through a systematic review of the medical records of the Division of Pediatric Nephrology, Children’s Hospital Giovanni XXIII, Bari, Italy. Inclusion criteria were an age of 1–18 years, normal glomerular filtration rate (>90 ml/min/1.73 m2) as estimated by the Schwartz formula [23] and a history of systemic GC therapy for SSNS within the prior 12 months. Participants with illnesses or who were receiving medications unrelated to SSNS that may impact growth, nutritional status, pubertal development or bone accrual were excluded. In total, 40 potential subjects were initially enrolled in the study; all subjects were asked to complete a questionnaire on lifestyle and health-related topics, including questions on physical activity, smoking habits, intake of calcium, former or current diseases and use of medications.
Of the 40 subjects, six were not eligible due to current use of medications or former inflammatory diseases, and four declined to participate, leaving 30 participants (17 males; mean age at diagnosis 5.20 ± 2.20 years) who were evaluated at the start of GC treatment (T0) and after 1 year of starting GC treatment (T1). Of these, 18 were also evaluated after a mean treatment duration of 2.44 ± 0.75 years (T2) and 1 year after the end of GC treatment (T3); the remaining 12 subjects continued GC treatment and were evaluated after a total treatment duration of 5.96 ± 2.33 years (T4) (Fig. 1).

Flow chart of study subject enrollment. GC Glucocorticoid
The study protocol was approved by the appropriate ethics committee and was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. Written informed consent to participate in the study was obtained from all subjects’ parents.
Anthropometry and pubertal assessment
Standing height (H) was measured by a wall-mounted Harpenden Stadiometer and weight (W) was measured with the patient wearing only underwear on an electronic scale with digital readings accurate to 0.1 kg. Waist circumference was measured midway between the lower rib margin and the iliac crest in the standing position and at the end of a gentle expiration. Body mass index (BMI) was calculated by dividing W (kilograms) by the square of H (meters), during documented urinary remission at the time of the study visit to avoid overestimation caused by edema. Obesity was defined as a BMI of >95th percentile for age and sex, in keeping with Italian growth charts [24]. In addition, the BMI standard deviation score (BMI SDS) was derived from a population standard [25]. Pubertal development was assessed according to the criteria of Tanner [26].
Therapeutic protocol
Medical charts were reviewed for the date of diagnosis of SSNS, the dates and number of relapses (defined as the occurrence of proteinuria >40 mg/m2/h for 3 consecutive days). The therapeutic protocol we use at our nephrology center, supported by the recent international guidelines, recommends that the dose of prednisone given initially is equal to 60 mg/m2/day for 6 weeks, followed by 40 mg/m2/day on alternate days for 6 weeks. Relapses are treated with 60 mg/m2/day until remission for 3 days, followed by 40 mg on alternate days for 4 weeks, with tapering at 10 mg/m2/week, scaling down to the minimum dose of 2.5 mg/m2/day [27]. All intravenous doses of methylprednisolone (20–30 mg/kg/day per 3 days) performed in cases of corticosteroid resistance were documented and converted to prednisone equivalents. The total GC exposure was summarized in terms of cumulative milligrams, milligrams per kilogram and milligrams per kilogram per day. All patients underwent supportive therapy with furosemide (1.2 mg/kg/day), albumin, antithrombin III, ranitidine, calcium (0.05–0.20 mg/kg/day), vitamin D (0.01 mg/kg/day) and antibiotics when necessary on the basis of the clinical condition of the patients.
Laboratory data
A venous blood sample was drawn from all participants at 08:00 a.m. after a 12-h fast. Parathyroid hormone (PTH) and (25)OH-vitamin D serum concentrations were measured by immunological tests based on the principle of chemiluminescence using commercial kits (Liaison assay; DiaSorin, Stillwater, MN). Osteocalcin serum concentration was measured by enzyme immunoassay, using a commercial kit (IBL International GmbH, Hamburg, Germany). Calcium, phosphorus and alkaline phosphatase concentrations were measured by the nephelometric method.
Imaging studies
Bone age was evaluated only at the onset of disease in all patients, and we found that it corresponded well with chronological age. During the course of disease bone health was evaluated using both DXA and QUS.
In all subjects BMD was measured at the lumbar spine from the first to the fourth lumbar vertebra by DXA, using a Hologic QDR 1000 densitometer (Hologic, Waltham, MA). Daily calibrations of the densitometer performed with a phantom during a 1-year period had provided a coefficient of variation of 0.56 %. All examinations were carried out in the continuous presence of trained technicians. Results were expressed as BMD Z-scores calculated on the basis of the normal reference values for age and sex provided by the manufacturer of the DXA system.
Bone quality was assessed in each subject by QUS measurements, performed with a DBM Sonic 1200 bone profiler (IgeaS.r.l., Carpi, MO, Italy) employing a sound frequency of 1.25 MHz. QUS is a radiation-free technique which evaluates bone mineral status in the peripheral skeleton by measuring the amplitude-dependent speed of sound (Ad-SoS), which reflects the ultrasound velocity inside the bone, and the bone transmission time (BTT), reflecting the bone characteristics without the interference of the soft tissue. It has also been demonstrated that gender, age, BMI and pubertal stage are independent predictors of AD-SoS and BTT in both sexes; thus, although a possible effect of obesity and edema at the onset of disease may be considered in patients with SSNS, phalangeal QUS is a useful tool to assess bone mineral status with a very small confounding effect [18, 28].
QUS was performed on the second to the fifth proximal phalanges of the non-dominant hand, and the mean value per person was calculated. Measurements were performed by the same operator and the coefficient of variation was 0.73 %, as determined by repeated measurements in each group of subjects (3 measurements per person on 3 different days). Ad-SoS and BTT results were expressed as Z-scores calculated on the basis of the normal values for age and sex obtained in a large Italian population sample [28]. We also considered the ultrasound bone profile index (UBPI) which represents the ultrasound risk of fracture (normal values 0–1) [28].
In agreement with the ISCD’s guideline, BMD, Ad-SoS and BTT were considered to be normal when Z-score values were above −2 SD and at the lower limit of normal when Z-score values were between <−1 and >−2. The diagnosis of osteoporosis was made when the BMD, AD-SoS and BTT Z-score values were <−2 SD [28].
Statistical analyses
The statistical analyses were conducted using SPSS for Windows, version 15.0 (SPSS Inc., Chicago, IL). All data are expressed as mean ± SD. Analysis of the results was performed by paired Student’s t test or Wilcoxon matched pairs test. Correlations between variables were assessed by Pearson or Spearman’s rank correlations where appropriate. The significance of progressive worsening over the time of treatment was assessed by analysis of variance.
Multiple linear regression analysis was performed in order to assess the relative contribution of total dosage of prednisone, number of relapses, BMI SDS or height SDS on the BMD Z-score and BTT Z-score, with the BMD Z-score or BTT Z-score as the dependent variable and total dosage of prednisone, number of relapses, BMI SDS or height SDS as the independent variable.
Changes in the DXA Z-score, BTT Z-score, Ad-SoS Z-score and UBPI within the patients over the different treatment durations were assessed with quasi-least squares (QLS) regression using the xtqls function in Stata 11.2 (StataCorp LP, College Station, TX) [29, 30]. QLS models allow for a variable number of measurements per participant and the implementation of the Markov correlation structure, which is appropriate for modeling associations among measurements that are unequally spaced in time. The QLS models include changes within each interval as the outcome (i.e., T0, T1, T2, T3 and T4). The models for changes in the DXA Z-score, BTT Z-score, Ad-SoS Z-score and UBPI evaluated associations with height SDS, number of relapses and duration of therapy. Differences were considered to be statistically significant at P < 0.05.
Results
Characteristics of the SSNS patients are presented in Table 1. None of the patients had fractures during the acute phase or relapses. In terms of pubertal status, 16 of the 18 subjects (88 %) who had stopped GC treatment after a mean of 2.44 ± 0.75 years (T2) were prepubertal (Tanner I), while all of the subjects who continued GC treatment for a mean of 5.96 ± 2.3 (T4) started to develop sexually during the therapy (Tanner II).
With respect to height SDS, no differences were found after 1 year of treatment in all patients, while a significant decrease at T2 and T4 with respect to the start (T0) of GC therapy was observed. Interestingly, no differences were observed at 1 year following the end of treatment (T3) compared to the start (T0). These results suggest a rescue in catch-up growth following interruption of GC therapy.
No statistically significant differences were found in relation to the BMI-SDS in all subjects at the different stages of treatment. Patients who had stopped treatment after a mean of 2.44 ± 0.75 years presented an average of 1.53 ± 0.51 relapses in the course of the first year of treatment (T1), and 2.86 ± 0.83 relapses during the following period until the end of treatment (T2). Patients who were still on treatment presented an average of 6.73 ± 1.57 relapses from the date of diagnosis.
In terms of serum markers of bone turnover, no differences were found at the different treatment stages for calcium, phosphorus, alkaline phosphatase and 25-OH vitamin D levels in all subjects; the exceptions were PTH and osteocalcin (Table 1). None of the patients had hypoalbuminemia, thus the levels of total calcium were not affected by albumin concentration. The apparent secondary hyperparathyroidism was likely due to hypocalcemia induced by GC; high levels of PTH are known to induce the reabsorption of calcium from bone, thus maintaining calcium levels in the normal range. Along the same line, higher osteocalcin levels at the T2 stage of GC treatment were the consequence of a greater stimulation of calcium absorption from the gut induced by GC treatment.
The DXA and QUS measurements of the study population over the study interval are given in Table 2. At diagnosis (T0), the mean lumbar BMD Z-score was within the normal range in all subjects; the results of QUS, mean Ad-SoS Z-score and mean BTT Z-score were also normal in all subjects. All of these parameters were normal even when corrected for chronological age, height and pubertal stage. No difference was found in the BMD, Ad-SoS and BTT Z-scores between males and females (data not shown). The average value of UBPI fell within the normal range (0–1). At 12 months from the start of GC therapy (T1), the densitometric parameters measured by DXA and QUS showed values within the normal limits for age, height and pubertal stage, and no statistically significant differences were observed at T1 compared to T0. Of the 18 patients assessed at T2, 11 (61 %) were in a state of bone mineralization at the lower limit of normal (BMD, Ad-SoS and BTT Z-scores of between <−1 and >−2); none of these children had osteoporosis (BMD Ad-SoS and BTT Z scores <−2). Statistically significant differences were found between the densitometric parameters at the end of treatment (T2) and those at T0 and T1. UBP1 values were significantly higher at the end of treatment than at the start. At 1 year from the end of treatment (T3), only one of 18 subjects (5.5 %) showed a state of bone mineralization at the lower limit of normal; the other 17 showed a normal bone mineralization on both DXA and QUS evaluation. In fact, we observed a significant increase in the BMD Z-score and UBPI values at T3 (vs. T2).
The densitometric parameters of subjects who continued GC treatment (T4) were significantly lower than those of subjects at T0, T1 and T2; in addition, UBPI values were significantly higher at T4 than at T0. In particular, of the 12 patients assessed at T4, three (25 %) showed a state of bone mineralization in the range of normal values, six (50 %) had densitometric parameters at the lower limit of normal values and three (25 %) showed a reduced bone mineralization.
Figure 2 shows the progressive worsening of densitometric parameters, as assessed by QUS and DXA, starting from T0 up to T2 and further to T4. The graphs clearly illustrate that GC therapies of <1 year had a minimal impact on bone, whereas longer therapies increased the risk of bone loss. We also found improved densitometric parameters in patients who had stopped therapy for at least 1 year (T3): the distributions of the QUS parameters (Ad-Sos, BTT and UBPI) and DXA (BMD) are clearly better at T3 than at T2 and T4, confirming a fast capability for recovery, particularly in those subjects who underwent GC therapy when they prepubertal.

Amplitude-dependent speed of sound (Ad-SoS) Z-score (a), bone transmission time (BTT) Z-score (b), ultrasound bone profile index (UBPI, c) and bone mineral density (BMD) Z-score (d) in children with steroid-sensitive nephrotic syndrome at T0, T1, T2, T3 and T4. Upper and lower ends of boxes 25th and 75th percentiles, respectively, horizontal line in box median, whiskers highest and lowest values, respectively. See Fig. 1 and footnotes to Table 1 for definition of T0, T1, T2, T3 and T4
In those patients who underwent GC treatment for a mean of 2.44 ± 0.75 years, the BTT Z-score, BMD Z-score and height Z-score at the end of the therapeutic period were significantly correlated with total dosage of prednisone (r = 0.613, P < 0.0151; r = 0.57, P < 0.0265; r = 0.503, P < 0.05, respectively).
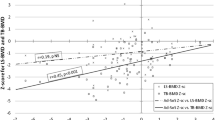
The patients who continued GC treatment for a mean of 5.96 ± 2.33 years showed a significant correlation between BTT Z-score and the number of relapses (r = −0.547; P < 0.0349), total dosage of prednisone ( r = −0.708; P < 0.00315), therapy duration (r = −0.547; P < 0.0349) and height Z-score (r = 0.520, P < 0.0566). The correlation coefficient between DXA and QUS parameters at different stages of the study are given in Table 3. The BMD Z-score significantly correlated with the BTT Z-score at each interval, while there was a variable correlation with other parameters at different stages of the GC treatment.
The impact of the number of relapses, total dosage of prednisone, therapy duration and height SDS predictor factors on the decrease of the BTT Z-score was analyzed by multiple logistic regression. This analysis revealed that the BTT Z-score was significantly related to the above-mentioned parameters according to different models (Table 4). No correlation was found with calcium supplementation, vitamin D supplementation, diuretic exposure and QUS measurements.
The BMD Z-score at T4 significantly correlated with the number of relapses (r = −0.751; P < 0.00126), total dosage of prednisone (r = −0.723; P < 0.00232), therapy duration (r = −0.751; P < 0.00126) and BMI-SDS (r = 0.201, P < 0.0126). The role of the number of relapses, total dosage of prednisone, therapy duration and BMI-SDS as predictor factors for the decrease in the BMD Z-score was analyzed by multiple logistic regression, which showed that the BMD Z-score was significantly correlated to the total dosage of prednisone and therapy duration according to the different models (Table 4).
The QLS model for changes in the BTT Z-score demonstrated that a smaller increase in the height SDS [β 0.177; 95 % confidence interval (CI) 0.05–0.30; P < 0.006] and prolonged GC therapy (β -0.12; 95 % CI −0.21 to 0.03; P < 0.007) were independently associated with the BTT Z-score.
In contrast, in the longitudinal analysis, prolonged GC therapy (β −0.87; 95 % CI −0.16 to 0.02; P < 0.016) was independently associated with the Ad-Sos Z-score. The QLS model for changes in UBPI demonstrated that a smaller increase in the height SDS (β 0.123; 95 % CI 0.03–0.21; P < 0.008) and prolonged GC therapy (β −0.74; 95 % CI −0.14 to −0.11; P < 0.02) were independently associated with UBPI. Further, in the longitudinal analysis, the QLS model for changes in the BMD Z-score demonstrated that a smaller increase in the height SDS (β 0.141; 95 % CI 0.03–0.26; P < 0.016), prolonged GC therapy (β −0.24; 95 % CI −0.27 to −0.21; P < 0.0001) and a higher number of relapses (β 0.11; 95 % CI 0.05–0.20; P < 0.04) were independently associated with a greater decrease in the BMD Z-score.
Discussion
In this study we examined changes in the bone health of a group of children and adolescents diagnosed with SSNS who were assessed for the first time by two diagnostic technologies, QUS and DXA. Our comparison of these two diagnostic tools revealed that they provided significant and overlapping significant information. Our longitudinal data shows that long-term high-dose GC therapy was associated with a status of bone mineralization at the lower limit of normal in most subjects and with a condition of reduced bone mineralization only in some patients (25 %) belonging to the group who underwent GC therapy for 3.8–9.6 years.
QUS is a free-radiation technique which has been validated for the prediction of subjects at risk of future fractures in areas where there is a limited availability of DXA data [31]. While DXA remains the gold standard for the diagnosis of osteoporosis, many studies in the dialysis patient population have also shown the effectiveness of QUS at the distal metaphysis of the phalanx in evaluating bone turnover and bone osteopenia [19]. The phalanx is a long bone consisting of a trabecular and cortical component, the main determinants of bone strength. This site is strongly predictive of the condition of the bone tissue in the entire skeletal system and the best predictor of osteoporotic fracture. The metaphysis of the phalanx is also characterized by a high bone turnover, which is sensitive to physiological changes (growth and aging), the presence of metabolic diseases (hyperparathyroidism) and/or iatrogenic effects (chronic dialysis treatment, GC treatment) [32, 33].
Many previous studies on bone status in patients with SSNS were performed using DXA or pQCT, both techniques that involve the use of radiation and, additionally, the data on bone health in these patients are discordant. In our study groups, QUS parameters were indicative of osteopenia in most subjects and of osteoporosis in a small percentage of subjects, reflecting data obtained by DXA. Our results are in agreement with those reported by Gulati et al. [34], who found that 61 % of their subjects had osteopenia (areal bone mineral density Z-score of <−1), and 22 % received a diagnosis of osteoporosis (Z-score of <−2.5). Patients who received prolonged steroid therapy (mean 5.96 ± 2.33 years) with frequent relapses (average 6.73) showed greater bone damage. Conversely, subjects treated for a mean of 2.44 ± 0.75 years and who had stopped treatment before entry into puberty showed an immediate recovery of bone status, which seems to reflect the ability of the skeleton to support transient decreases in bone formation induced by GC treatment during childhood. In contrast, peak bone mass is mainly reached during adolescence or early adulthood and, therefore, any factor affecting bone growth and remodeling or bone storage during this phase of life might impair the attainment of an optimal peak bone mass, predisposing the individual to osteoporosis and fracture later in life. This is in keeping with our data on patients who entered into puberty while they were in treatment and who subsequently demonstrated a worsening of densitometric parameters in comparison to prepubertal patients.
Similar to previously published findings, our longitudinal data demonstrate impaired linear growth: (1) subjects had a lower height SDS after 3 or more years of GC treatment compared to that at the start of treatment; (2) the parameters of longitudinal growth recovered to a level comparable to that at the start in subjects who stopped GC treatment after a mean of 2.44 ± 0.75 years, while growth impairment persisted in subjects who continued GC treatment for a mean of 5.96 ± 2.33 years. In these subjects, the BTT Z-score, BMD Z-score and height SDS significantly correlate with the total dosage of prednisone. Furthermore, the BTT and BMD Z-scores significantly correlate with the number of relapses, therapy duration and height SDS. Interestingly, in our study height SDS represents a significant predictor of bone status only in relation to the BTT Z-score, and not with the BMD Z-score, suggesting that QUS could be related to growth.
The effect of duration of the insult on the potential for bone mass recovery in young subjects was explored by Gafni et al. [35], who showed that short-term, high-dose dexamethasone administration to 5-week-old rabbits resulted in greatly reduced tibial bone mass. Complete recovery through endochondral bone formation was then achieved by 16 weeks following the cessation of dexamethasone. These data suggest that significant, but temporary, insults to the skeleton early in life may not ultimately affect bone strength because much of the young skeleton is replaced entirely through bone growth. On the other hand, insults that affect skeletal health in the long term, or during the later pediatric years when growth potential is less, may be associated with persistent skeletal disease [36].
In conclusion, our results indicate that long-term GC treatment in patients with SSNS causes a status of lower bone mineralization, based on assessments by both lumbar DXA and phalangeal QUS, which is related to dosage and therapy duration, with a better recovery of bone health in prepubertal than in pubertal children. Both Ad-SoS and BTT were comparable to BMD, indicating that phalangeal QUS is a reliable diagnostic tool to evaluate bone health.
Although none of our patients had significant bone disease and none showed fractures, we suggest a monitoring of bone health in such patients to prevent the risk of fractures, which although estimated to be low in childhood, increases to 20 % in adulthood [37]. Thus, the use of an easy, cheap [28] and radiation-free technique such as QUS provides an inexpensive and potentially efficacious method in terms of future benefits to follow up these patients.
References
van Staa TP, Cooper C, Leufkens HG, Bishop N (2003) Children and the risk of fractures caused by oral corticosteroids. J Bone Miner Res 18:913–918
Canalis E, Mazziotti G, Giustina A, Bilezikian JP (2007) Glucocorticoid-induced osteoporosis: pathophysiology and therapy. Osteoporos Int 10:1319–1328
Ventura A, Brunetti G, Colucci S, Oranger A, Ladisa F, Cavallo L, Grano M, Faienza MF (2013) Glucocorticoid-induced osteoporosis in children with 21-hydroxylase deficiency. Biomed Res Int 2013:250462
O’Brien CA, Jia D, Plotkin LI, Bellido T, Powers CC, Stewart SA, Manolagas SC, Weinstein RS (2004) Glucocorticoids act directly on osteoblasts and osteocytes to induce their apoptosis and reduce bone formation and strength. Endocrinology 145:1835–1841
Faienza MF, Brunetti G, Colucci S, Piacente L, Ciccarelli M, Giordani L, Del Vecchio GC, D’Amore M, Albanese L, Cavallo L, Grano M (2009) Osteoclastogenesis in children with 21-hydroxylase deficiency on long-term glucocorticoid therapy: the role of receptor activator of nuclear factor-kappaB ligand/osteoprotegerin imbalance. J Clin Endocrinol Metab 94:2269–2276
Brunetti G, Faienza MF, PiacenteL VA, Oranger A, Carbone C, Di Benedetto A, Colaianni G, Gigante M, Mori G, Gesualdo L, Colucci S, Cavallo L, Grano M (2013) High dickkopf-1 levels in sera and leukocytes from children with 21-hydroxylase deficiency on chronic glucocorticoid treatment. Am J Physiol Endocrinol Metab 304:E546–E554
Faienza MF, Ventura A, Marzano F, Cavallo L (2013) Postmenopausal osteoporosis: the role of immune system cells. Clin Dev Immunol 2013:575936
Foster BJ, Shults J, Zemel BS, Leonard MB (2004) Interactions between growth and body composition in children treated with high-dose chronic glucocorticoids. Am J Clin Nutr 80:1334–1341
Phan V, Blydt-Hansen T, Feber J, Alos N, Arora S, Atkinson S, Bell L, Clarson C, Couch R, Cummings EA, Filler G, Grant RM, Grimmer J, Hebert D, Lentle B, Ma J, Matzinger M, Midgley J, Pinsk M, Rodd C, Shenouda N, Stein R, Stephure D, Taback S, Williams K, Rauch F, Siminoski K, Ward LM (2014) Skeletal findings in the first 12 months following initiation of glucocorticoid therapy for pediatric nephrotic syndrome. Osteoporos Int 25:627–637
Hogler W, Blimkie CJ, Cowell CT, Kemp AF, Briody J, Wiebe P, Farpour-Lambert N, Duncan CS, Woodhead HJ (2003) A comparison of bone geometry and cortical density at the mid-femur between prepuberty and young adulthood using magnetic resonance imaging. Bone 33:771–778
Bianchi ML (2002) Glucorticoids and bone: some general remarks and some special observations in pediatric patients. Calcif Tissue Int 70:384–390
Halton JM, Atkinson SA, Fraher L, Webber C, Gill GJ, Dawson S, Barr RD (1996) Altered mineral metabolism and bone mass in children during treatment for acute lymphoblastic leukemia. J Bone Miner Res 11:1774–1783
Leonard MB, Feldman HI, Shults J, Zemel BS, Foster BJ, Stallings VA (2004) Long-term, high-dose glucocorticoids and bone mineral content in childhood glucocorticoid-sensitive nephrotic syndrome. N Engl J Med 351:868–875
Burnham JM, Shults J, Petit MA, Semeao E, Beck TJ, Zemel BS, Leonard MB (2007) Alterations in proximal femur geometry in children treated with glucocorticoids for Crohn disease or nephrotic syndrome: impact of the underlying disease. J Bone Miner Res 22:551–559
Wetzsteon RJ, Shults J, Zemel BS, Gupta PU, Burnham JM, Herskovitz RM, Howard KM, Leonard MB (2009) Divergent effects of glucocorticoids on cortical and trabecular compartment BMD in childhood nephrotic syndrome. J Bone Miner Res 24:503–513
Tsampalieros A, Gupta P, Denburg MR, Shults J, Zemel BS, Mostoufi-Moab S, Wetzsteon RJ, Herskovitz RM, Whitehead KM, Leonard MB (2013) Glucocorticoid effects on changes in bone mineral density and cortical structure in childhood nephrotic syndrome. J Bone Miner Res 28:480–488
Krieg MA, Barkmann R, Gonnelli S, Stewart A, Bauer DC, Del Rio BL, Kaufman JJ, Lorenc R, Miller PD, Olszynski WP, Poiana C, Schott AM, Lewiecki EM, Hans D (2008) Quantitative ultrasound in the management of osteoporosis: the 2007 ISCD Official Positions. J Clin Densitom 11:163–187
Baroncelli GI, Federico G, Bertelloni S, Sodini F, De Terlizzi F, Cadossi R, Saggese G (2003) Assessment of bone quality by quantitative ultrasound of proximal phalangeas of the hand and fracture rate in children and adolescents with bone and mineral disorders. Pediatr Res 54:125–136
Christoforidis A, Printza N, Gkogka C, Siomou E, Challa A, Kazantzidou E, Kollios K, Papachristou F (2011) Comparative study of quantitative ultrasonography and dual-energy X-ray absorptiometry for evaluating renal osteodystrophy in children with chronic kidney disease. J Bone Miner Metab 29:321–327
Guglielmi G, de Terlizzi F, Aucella F (2004) Quantitative bone ultrasonography: state of the art and perspectives. G Ital Nefrol 21:343–354
Di Mase R, Cerbone M, Improda N, Esposito A, Capalbo D, Mainolfi C, Santamaria F, Pignata C, Salerno M (2012) Bone health in children with long-term idiopathic subclinical hypothyroidism. Ital J Pediatr 38:56
International Study of Kidney Disease in Children (1981) The primary nephrotic syndrome in children. Identification of patients with minimal change nephrotic syndrome from initial response to prednisone. A report of the International Study of Kidney Disease in Children. J Pediatr 98:561–564
Schwartz GJ, Haycock GB, Edelmann CM Jr, Spitzer A (1976) A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics 58:259–263
Cacciari E, Milani S, Balsamo A, Spada E, Bona G, Cavallo L, Cerutti F, Gargantini L, Greggio N, Tonini G, Cicognani A (2006) Italian cross-sectional growth charts for height, weight and BMI (2 to 20 yr). J Endocrinol Investig 29:581–593
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH (2000) Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 320:1240–1243
Tanner JM, Whitehouse RH (1976) Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child 51:170–179
Lombel RM, Gipson DS, Hodson EM (2013) Treatment of steroid-sensitive nephrotic syndrome: new guidelines from KDIGO. Pediatr Nephrol 28:415–426
Baroncelli GI, Federico G, Vignolo M, Valerio G, del Puente A, Maghnie M, Baserga M, Farello G, Saggese G (2006) Phalangeal Quantitative Ultrasound Group. Cross-sectional reference data for phalangeal quantitative ultrasound from early childhood to young-adulthood according to gender, age, skeletal growth, and pubertal development. Bone 39:159–173
Shults J, Morrow AL (2002) Use of quasi-least squares to adjust for two levels of correlation. Biometrics 58:521–530
Shults J, Ratcliffe SJ, Leonard M (2007) Improved generalized estimating equation analysis via xtqls for quasi-least squares in Stata. Stata J 7:147–166
Gordon CM, Lewiecki EM, Baim S, Leonard MB, Bishop NJ, Bianchi ML, Kalkwarf HJ, Langman CB, Plotkin H, Rauch F, Zemel BS, Binkley N, Bilezikian JP, Kendler DL, Hans DB, Silverman S (2008) International Society for Clinical Densitometry Adult and Pediatric Official Positions. Bone 43:1115–1121
Wüster C, Albanese C, De Aloysio D, Duboeuf F, Gambacciani M, Gonnelli S, Glüer CC, Hans D, Joly J, Reginster JY, De Terlizzi F, Cadossi R (2000) Phalangeal osteosonogrammetry study (PhOS): age related changes, diagnostic sensitivity and discrimination power. J Bone Miner Res 15:1603–1614
Knapp KM (2009) Quantitative ultrasound and bone health. Salud Publica Mex 51:S18–S24
Gulati S, Sharma RK, Gulati K, Singh U, Srivastava A (2005) Longitudinal follow-up of bone mineral density in children with nephrotic syndrome and the role of calcium and vitamin D supplements. Nephrol Dial Transplant 20:1598–1603
Gafni RI, Weise M, Robrecht DT, Meyers JL, Barnes KM, De-Levi S, Baron J (2001) Catch-up growth is associated with delayed senescence of the growth plate in rabbits. Pediatr Res 50:618–623
Henderson RC, Madsen CD, Davis C, Gold SH (1998) Longitudinal evaluation of bone mineral density in children receiving chemotherapy. J Pediatr Hematol Oncol 20:322–326
Skrzypczyk P, Panczyk-Tomaszewska M, Roszkowska-Blaim M, Wawer Z, Bienias B, Zajgzkowska M, Kilis-Pstrusinska K, Jakubowska A, Szczepaniak M, Pawlak-Bratkowska M, Tkaczyk M (2014) Long-term outcomes in idiopathic nephrotic syndrome: from childhood to adulthood. Clin Nephrol 81:166–173
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Aceto, G., D’Addato, O., Messina, G. et al. Bone health in children and adolescents with steroid-sensitive nephrotic syndrome assessed by DXA and QUS. Pediatr Nephrol 29, 2147–2155 (2014). https://doi.org/10.1007/s00467-014-2834-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-014-2834-3