
Abstract
Background
Single-port laparoscopic surgery as an alternative to conventional laparoscopic cholecystectomy for benign disease has not yet been accepted as a standard procedure. The aim of the multi-port versus single-port cholecystectomy trial was to compare morbidity rates after single-access (SPC) and standard laparoscopy (MPC).
Methods
This non-inferiority phase 3 trial was conducted at 20 hospital surgical departments in six countries. At each centre, patients were randomly assigned to undergo either SPC or MPC. The primary outcome was overall morbidity within 60 days after surgery. Analysis was by intention to treat. The study was registered with ClinicalTrials.gov (NCT01104727).
Results
The study was conducted between April 2011 and May 2015. A total of 600 patients were randomly assigned to receive either SPC (n = 297) or MPC (n = 303) and were eligible for data analysis. Postsurgical complications within 60 days were recorded in 13 patients (4.7 %) in the SPC group and in 16 (6.1 %) in the MPC group (P = 0.468); however, single-access procedures took longer [70 min (range 25–265) vs. 55 min (range 22–185); P < 0.001]. There were no significant differences in hospital length of stay or pain VAS scores between the two groups. An incisional hernia developed within 1 year in six patients in the SPC group and in three in the MPC group (P = 0.331). Patients were more satisfied with aesthetic results after SPC, whereas surgeons rated the aesthetic results higher after MPC. No difference in quality of life scores, as measured by the gastrointestinal quality of life index at 60 days after surgery, was observed between the two groups.
Conclusions
In selected patients undergoing cholecystectomy for benign gallbladder disease, SPC is non-inferior to MPC in terms of safety but it entails a longer operative time. Possible concerns about a higher risk of incisional hernia following SPC do not appear to be justified. Patient satisfaction with aesthetic results was greater after SPC than after MPC.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
In 1992 Pelosi first described the use of a single umbilical puncture for laparoscopic appendectomy [1], and in 1997 Navarra et al. published, as a short note, their results after single-incision laparoscopic cholecystectomy [2]. It is only more recently that the technique has begun to gain wider acceptance. Concerns over the safety issues with this new technique have been voiced by claims that its widespread adoption would lead to a significant increase in complications, especially bile duct injuries, as occurred during the early years of conventional laparoscopic cholecystectomy [3, 4]. More recently published studies have failed to demonstrate any major differences in clinical outcome after the single-incision laparoscopic technique versus standard multi-port laparoscopy [4–9]. Furthermore, there is increasing doubt about whether the new technique actually delivers the benefits of improved aesthetic results, reduced postoperative pain, earlier return to work, and greater patient satisfaction [10–12]. Also, it has been found that a larger peri-umbilical incision and consequent fascial defect may result in a higher rate of incisional hernia.
The aim of this randomised controlled trial (RCT) was to compare overall morbidity after single-incision laparoscopic technique versus standard multi-port laparoscopy for cholecystectomy in terms of skin incision-related morbidity, postoperative pain, and aesthetic results—the potential benefits advocated for single-port laparoscopic surgery.
Methods
We designed this multi-centre RCT under the endorsement of the Technology Committee of the European Association for Endoscopic Surgery (EAES). The project was approved by the local ethical committee (COMITATO ETICO INTERAZIENDALE, A.O.U. CITTA’ DELLA SALUTE E DELLA SCIENZA DI TORINO, University of Torino, Italy) of the principle study centre. The project was registered with ClinicalTrials.gov, U.S. International Clinical Trials Databank (U.S. National Institutes of Health), under ID-code NCT01104727, on behalf of the EAES. The study was designed to conform with CONSORT criteria.
Study population
The study population was patients with symptomatic cholelithiasis (gallstones <2 cm in diameter), gallbladder dyskinesia, or gallbladder polyps. Other inclusion criteria were: age 18–75 years, body mass index (BMI) <30, ASA class I–III, absence of non-correctable coagulopathy, and no previous abdominal surgery above the umbilicus. Exclusion criteria were preoperative clinical findings of acute cholecystitis, suspected common bile duct stones or cancer, or previous surgery of the upper abdomen or of the umbilicus.
Patient recruitment
Consecutive eligible patients were recruited at the outpatient clinic of each participating centre by a designated physician. Patients granting informed consent were enrolled in the trial, allocated to one of the treatment groups by computerised randomisation via web-based software, and treated according to the study protocol. Patients unable or refusing to provide informed consent were treated according to current clinical guidelines. Surgeons designated as first operator had to demonstrate documented performance of at least 50 cholecystectomies and previous experience with single-port instruments in at least 15 cases.
Randomisation
Patient data were entered into a web-based database by a designated physician at each centre. Blind computerised randomisation (1:1 allocation ratio), stratified per single centre, was done by unchangeable number-generating software. To ensure that an approximately equal number of patients would be allocated to each arm of the study, each of the 20 centres composing the Consortium had to enrol 30 patients. Patients were allocated to undergo either conventional 4-port cholecystectomy (MPC) or single-port cholecystectomy (SPC).
Operative technique
MPC procedure
A 12-mm Hg pneumoperitoneum was created through either a 10-mm umbilical Hasson’s port or a Veress needle, and a 10-mm umbilical port was inserted; a second 10-mm and two 5-mm ports were then placed. Instrumentation included a straight or angulated laparoscope, laparoscopic graspers, monopolar hook, bipolar forceps, scissors, and a 10-mm clips applier. A plastic bag system for gallbladder extraction was used as needed. Fascia suturing of the 10- and 12-mm access sites was done with resorbable sutures, and the skin was closed with either metallic clips or interrupted sutures.
SPC procedure
A single skin incision was made inside the umbilicus. The subcutaneous tissue was dissected, the muscular fascia exposed and incised along the middle line (linea alba), taking care not to damage the muscular tissue. The peritoneum was identified and incised. A single-port device was inserted and anchored. Depending on which port was used, either straight or curved instruments, crossed or uncrossed handles, gallbladder retractors or transcholecystic sutures or any other technical solution could be employed to complete the procedure safely. After cholecystectomy was completed and the gallbladder removed with/without a plastic bag, the fascia was sutured. Before closure, the fascial defect and the skin incision were measured in maximum length with sterile callipers and each was photographed for documentation. The choice of closure technique was left to the surgeon and had to be specified in detail on the surgical report form. The skin incision was secured with either metallic clips or interrupted sutures.
Primary end point
Overall morbidity rate was defined as any surgery-related morbidity that occurred within 60 days after surgery. Morbidity was defined as the occurrence of any complication directly or indirectly related to surgery. Complications were classified according to Dindo [13].
Secondary end points
Operative time was recorded in minutes between skin incision and end of skin closure. Conversion rate from SPC to MPC was defined as the number of cases in which the procedure was converted from SPC to MPC for safety or technical reasons. Conversion rate to open surgery was defined as the number of cases in which the procedure was converted from SPC or MPC to laparotomy for safety or technical reasons. Postoperative pain was assessed by means of a self-report horizontal visual analogical scale (VAS) for pain recorded daily for the first week and then weekly up to 60 days after surgery. Paracetamol IV 3 times a day was administered for the first 24 h and on demand thereafter. Tramadol was administered when pain control with paracetamol was judged insufficient. A single dose of ketorolac was given on request. Hospital length of stay was defined as the number of inhospital days after surgery. All participating study centres applied the following standardised discharge criteria: normal intake of nutrition; normal mobility; absence of fever (<38 °C); and stable haemoglobin level during postoperative day 1 (<1 g/dL). In cases of same-day discharge from hospital, patients were contacted by telephone the day after the operation. Follow-up examinations were scheduled at 30 and 60 days after surgery. Skin incision-related morbidity was defined as the occurrence of bleeding, infection, necrosis, skin retraction, incisional hernia, or suture dehiscence within 60 days after surgery.
Surgeon-evaluated aesthetic results were judged by three independent surgeons on the basis of a standardised methodology. The surgeons viewed two digital photographs (minimum resolution 800 × 600 pixels) of each patient in standing position taken before and then at 60 days after surgery. One was a close-up photo of the umbilical area and the other a large view of the abdomen. The results were scored on a 5-point Likert scale from 1 to 5 (1 indicates very poor, 2 poor, 3 satisfactory, 4 good, and 5 very good) in answer to the following questions:
-
1.
How would you rate the overall aesthetic results of the abdomen after surgery?
-
2.
How would you rate the scar size?
-
3.
How would you rate the scar shape?
-
4.
How would you rate the skin colour?
-
5.
How would you rate the skin retraction?
Patient-evaluated aesthetic results were judged by the patients on the basis of the scores marked on a 5-point Likert scale administered at the follow-up visit 60 days after surgery in answer to the following questions:
-
1.
How would you rate the overall aesthetic appearance of your body after surgery?
-
2.
How would you rate the impact of the surgical scar/s on the appearance of your abdomen?
-
3.
How would you rate the aesthetic appearance of the surgical scar/s?
-
4.
How would you rate the impact of the surgical scar/s on your everyday life?
Quality of life was assessed with the gastrointestinal quality of life index (GIQLI) at the follow-up visit 60 days after surgery.
Long-term morbidity was defined as any surgery-related morbidity that occurred within 1 year after surgery. Incisional hernia was defined as any fascial defect revealed on physical examination and confirmed by ultrasound within 1 year after surgery.
Sample size and power calculation
Assuming a baseline overall morbidity rate of 4 % in both the MPC and SPC groups (average morbidity rates drawn from the literature) and considering a clinically significant difference of 4 % (up to 8 % global) for SPC to be non-inferior, with a β-error of 0.2 and α-error of 0.05, a total of 600 patients were needed.
Data analysis
Intra- and postoperative data were entered in the web-based database at any time during the study by the recruiting surgeon. The photographic documentation was also up-loaded into the computerised database. Patients’ personal data were protected against unauthorised or accidental access. All analyses were carried out primarily on an intention-to-treat basis. Risk of bias was evaluated based on the CONSORT 2010 [14] statement.
Monitoring
Three experts in bilio-pancreatic and laparoscopic surgery were designated as members of multi-port versus single-port cholecystectomy (MUSIC) trial monitoring committee (Music TMC). They had access to the data during the entire course of the study and could recommend cessation of the trial if one arm was providing manifestly inferior results.
Statistical analysis
Categorical variables are described as frequencies and percentages and continuous variables as the median. The interquartile range (IQR) is given in brackets. The association between any categorical variable and treatment arm (MPC/SPC) was analysed using Fisher’s exact test; the Mann–Whitney test was used for continuous variables. All reported P values were obtained by the two-sided exact method at the conventional 5 % significance level. Data were analysed as of June 2016 by R 3.2.3 (R Foundation for Statistical Computing, Vienna-A, http://www.R-project.org).
Results
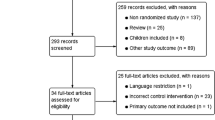
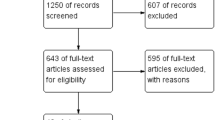
Following Ethical Committee approval, enrolment was begun on 1 April, 2011 and closed on 7 July, 2015. All 20 centres but 1 involved in the study at the time of trial registration recruited patients. Six of these 19 centres recruited an insufficient number of patients to complete the series according to local stratification (Table 1). By unanimous decision of the Consortium, the number of patients to be enrolled and randomised at the 13 other centres was raised to 40 in order to achieve the target of 600 patients (Fig. 1). The data from the patients recruited at the six centres were pooled as a miscellaneous group for sensitivity analysis by centre.

CONSORT 2010 flow diagram
The indication for cholecystectomy was cholelithiasis in 578 patients, gallbladder polyps in 20, and gallbladder dyskinesia in 2. Table 2 presents the patients’ characteristics, Table 3 the definitive diagnosis, and Table 4 the various device systems.
Data regarding skin and fascial incisions were reported in 278/297 patients. The median size of the skin incision was 25 mm (range 20–30). The median size of the fascial incision was 25 mm (range 20–30). Intraoperative complications were recorded in 25 patients in the MPC group (gallbladder perforation in 20, liver laceration in 3, and bleeding in 2) and in 21 patients in the SPC group (gallbladder perforation in 14, duodenal injury in 1, liver laceration in 1, and bleeding in 5) (P = 0.647). During SPC, an additional trocar was added in 18 procedures, and more than one trocar in 14 procedures, which were then recorded as conversion to laparoscopy. One procedure in the SPC group was converted to open surgery. Approximately equal amounts of analgesia were recorded for both groups (Table 5). The median VAS pain score was 2 in the MPC group (range 1–4) and 3 in the SPC group (range 1–4) (P = 0.905). The median hospital length of stay was 2 days in the MPC group (range 1–3) and 3 days in the SPC group (range 1–2) (P = 0.808). Postoperative complications during inhospital stay were recorded in 3 patients in the MPC group (biliary leak in 1, pulmonary effusion in 1, and subcutaneous emphysema in 1) and in 5 in the SPC group (bleeding in 2, hyperthermia in 1, increase in inflammatory markers in 1, and acute hypertension in 1) (P = 0.496).
A total of 541/600 patients (90.2 %) completed follow-up at 60 days. Postoperative complications at 60 days occurred in 11 MPC group patients (biliary leak in 1, skin suture dehiscence in 4, fascial suture dehiscence in 2, hyperthermia in 1, pulmonary infection in 1, diarrhoea in 1, and subphrenic abscess in 1) and in 11 SPC group patients (biliary leak in 2, skin suture dehiscence in 2, fascial suture dehiscence in 5, intra-abdominal collection in 1, and persistent neck pain in 1) (P = 1.000). Postoperative complications within 60 days were recorded in 13 patients (4.7 %) in the MPC group and in 16 (6.1 %) in the SPC group, which demonstrated the non-inferiority of the SPC technique as compared to MPC in terms of morbidity (P = 0.468). Complications recorded in 541/600 patients were classified according to Dindo [13] (Table 6). No further surgery was required in any cases.
A total of 446/600 patients (74.3 %) completed follow-up at 1 year. Postoperative complications were recorded in 9 MPC group patients (biliary stenosis in 1, skin retraction in 2, keloid formation in 3, and incisional hernia in 3) and in 10 SPC group patients (biliary stenosis in 1, skin retraction in 2, keloid formation in 1, and incisional hernia in 6) (P = 0.817). Complications within 1 year after surgery were recorded in 22 patients (9.7 %) in each group (P = 1.000).
Data on patient-evaluated aesthetic results were available for 513/600 patients. The patients in the SPC group gave the aesthetic results a significantly higher score on all accounts (Table 7). Data on surgeon-evaluated aesthetic result were available for 289/600 patients. The surgeons gave significantly higher scores particularly for scar and skin retraction in the MPC group (Table 8). There were no significant differences between the two groups (505/600 patients) in quality of life scores as measured with the GIQLI at 60 days after surgery (Table 9).
Discussion
Although single-port laparoscopic surgery is not new [1, 2], its use has gained momentum over the last few years in part through the support of major surgical instrument manufacturers. This raises concerns about a possible industry-driven interest in promoting wider use of the technique. There is no doubt, however, that single-port surgery has several drawbacks particularly in relation to the lack of “triangulation” to which laparoscopic surgeons have grown accustomed in terms of both instruments and scope. Although this seems to have been overcome by the growing acceptability of in-line viewing, device manufacturers have focused their product research on developing and marketing a variety of curved instruments featuring different characteristics with the aim of restoring standard triangulation as provided in a laparoscopic environment. Nevertheless, a recent study that measured ergonomic performance on a virtual-reality simulator designed for the purpose demonstrated that, after a short learning curve, only very experienced surgeons were able to perform the surgical tasks safely and effectively, while all the other surgeons found technique acquisition to be challenging [15].
For this reason, we chose as the main outcome the non-inferiority of SPC versus MPC in terms of overall postoperative morbidity at 60 days, and the results confirm this: no difference in severity of complications was observed. Hence, the hypothesis that SPC would be associated with a higher complications rate, but with greater overall satisfaction with clinical and aesthetic results, is not confirmed [6]. Few patients experienced complications, mostly minor, with 2 cases of biliary leak and 1 case of biliary stenosis recorded per group, all successfully treated by endoscopic retrograde cholangio-pancreatography (ERCP). Operative time was slightly but significantly longer in the SPC group, although this difference seems of marginal relevance for operating room organisation. An additional trocar was employed in very few cases, and in even fewer in which the procedure was converted to laparoscopy.
Moreover, it has been claimed that a larger peri-umbilical incision and consequent fascial defect would increase the risk of incisional hernia [9]. This article presents the largest series with 1-year follow-up of patients enrolled in a single-blind, multi-centre, prospective, randomised, controlled trial of SPC versus standard MPC. Although this was true in our series, the incidence of incision hernia was so low in both groups that many more cases would be needed to achieve significance if confirmed. This reinforces the hypothesis that the finding of Marks et al. [9] was depending on an increased rate of incisional adverse events, in particular a higher rate of superficial wound complications in the single-port group. This was not confirmed in our series, three times larger, and in which possible local biases were more likely to be avoided due to the proportional distribution of patients among the different centres. No other significant differences between the groups were observed in relation to the perioperative course, pain VAS scores, analgesic consumption, or QoL at 60 days as assessed by the GIQLI.
The basic rationale for the interest in single-port laparoscopy is that, because it may improve cosmesis and decrease postoperative pain, patient satisfaction would be greater than after standard laparoscopy. Our study shows that the majority of the patients in the single-port group were pleased with their aesthetic results, although it may be argued that other not investigated factors might have influenced their personal opinion. In contrast, the surgeon-evaluated aesthetic results were based on a comparative, standardised methodology in which the images were viewed and objectively scored by three independent surgeons. In their opinion, the scar shape and skin retraction after MPC appeared aesthetically more acceptable.
There are several limitations to this study that must be discussed. First, approximately 25 % of patients were lost to follow-up at 1 year, which is higher than would be normally expected for a 12-month prospective study. Second, all surgeons participating in this trial had performed at least 15 previous SPC cases, but the ability to generalise outcomes from this study might not be applicable to those in the initial learning curve associated with this new technique. Finally, the follow-up of 12 months might be too short to determine the true differences between SPC and MPC in terms of risk for hernia development.
Conclusions
In selected patients undergoing cholecystectomy for benign gallbladder disease, a single-access technique is non-inferior to standard laparoscopy in terms of safety, but it entails a longer operative time. The short follow-up cannot exclude possible concerns about a higher risk of incisional hernia following SPC, although this was not demonstrated in the present study. Patients rated the aesthetic results after the single-access technique higher than after standard laparoscopy.
References
Pelosi MA, Pelosi MA III (1992) Laparoscopic appendectomy using a single umbilical puncture (minilaparoscopy). J Reprod Med 37:588–594
Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I (1997) One-wound laparoscopic cholecystectomy. Br J Surg 84:695
Allemann P, Schafer M, Demartines N (2010) Critical appraisal of single port access cholecystectomy. Br J Surg 97:1476–1480
Joseph M, Phillips MR, Farrell TM, Rupp CC (2012) Single incision laparoscopic cholecystectomy is associated with a higher bile duct injury rate. A review and a word of caution. Ann Surg 256:1195–1200
Asakuma M, Hayashi M, Komeda K, Shimizu T, Hirokawa F, Miyamoto Y, Okuda J, Tanigawa N (2011) Impact of single-port cholecystectomy on postoperative pain. Br J Surg 98:991–995
Ma J, Cassera MA, Spaun GO, Hammill CW, Hansen PD, Aliabadi-Wahle S (2011) Randomized controlled trial comparing single-port laparoscopic cholecystectomy and four-port laparoscopic cholecystectomy. Ann Surg 254:22–27
Lee PC, Lo C, Lai PS, Chang JJ, Huang SJ, Lin MT, Lee PH (2010) Randomized clinical trial of single-incision laparoscopic cholecystectomy versus minilaparoscopic cholecystectomy. Br J Surg 97:1007–1012
Lirici MM, Califano AD, Angelini P, Corcione F (2011) Laparo-endoscopic single site cholecystectomy versus standard laparoscopic cholecystectomy: results of a pilot randomized trial. Am J Surg 202:45–52
Marks JM, Phillips MS, Tacchino R, Roberts K, Onders R, DeNoto G, Gecelter G, Rubach E, Rivas H, Islam A, Soper N, Paraskeva P, Rosemurgy A, Ross S, Shah S (2013) Single-incision laparoscopic cholecystectomy is associated with improved cosmesis scoring at the cost of significantly higher hernia rates: 1-year results of a prospective randomized, multicenter, single-blinded trial of traditional multiport laparoscopic cholecystectomy vs single-incision laparoscopic cholecystectomy. J Am Coll Surg 216:1037–1047
Edwards C, Bradshaw A, Ahearne P, Dematos P, Humble T, Johnson R, Mauterer D, Soosaar P (2010) Single-incision laparoscopic cholecystectomy is feasible: initial experience with 80 cases. Surg Endosc 24:2241–2247
Vettoretto N, Arezzo A (2010) Human natural orifice translumenal endoscopic surgery: on the way to two different philosophies? Surg Endosc 24:490–492
Lirici MM, Arezzo A (2006) Surgery without scars: the new frontier of minimally invasive surgery? Controversies, concerns and expectations in advanced operative endoscopy. Minim Invasive Ther Allied Technol 15:323–324
Moher D, Hopewell S (2010) CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ 340:c869
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Rimonda R, Brown S, Tang B, Cuschieri A (2012) Ergonomic performance with crossed and uncrossed instruments in single port laparoscopic surgery. Surg Endosc 26:3605–3611
Acknowledgments
The study was supported by a research grant from the European Association for Endoscopic Surgery in 2011.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Alberto Arezzo reports having received a grant from the European Association for Endoscopic Surgery to conduct this study. Dr. Luigi Boni reports having received travel grants from Karl Storz during this study. Drs. Roberto Passera, Alberto Bullano, Yoav Mintz, Asaf Kedar, Elisa Cassinotti, Riccardo Rosati, Uberto Fumagalli Romario, Mario Sorrentino, Marco Brizzolari, Nicola Di Lorenzo, Achille Lucio Gaspari, Dario Andreone, Elena De Stefani, Giuseppe Navarra, Salvatore Lazzara, Maurizio Degiuli, Kirill Shishin, Igor Khatkov, Ivan Kazakov, Rudolf Schrittwieser, Thomas Carus, Alessio Corradi, Guenther Sitzman, Antonio Lacy, Selman Uranues, Amir Szold, and Mario Morino have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Arezzo, A., Passera, R., Bullano, A. et al. Multi-port versus single-port cholecystectomy: results of a multi-centre, randomised controlled trial (MUSIC trial). Surg Endosc 31, 2872–2880 (2017). https://doi.org/10.1007/s00464-016-5298-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-016-5298-7