
Abstract
Background
Mesh fixation is a critical step in TAPP laparoscopic hernia repair because tackers used for this purpose are associated with possible neuralgia.
Methods
For the present study, 70 patients referred with unilateral inguinal or femoral hernia were divided in two groups for hernia repair. In first group mesh was fixed with titanium tacker. In the second group mesh was fixed with a single suture of Vicryl.
Results
Patients in the Vicryl group experienced less postoperative pain and analgesic consumption. Six month follow-up demonstrated no hernia recurrence either.
Conclusions
According to results, use of Vicryl suture instead of a titanium tacker is beneficial owing to reduced pain, less analgesic consumption, and lower cost.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Among different methods introduced for reducing hernia repair complications, laparoscopic techniques have gained broad acceptance. Since the early 1990s, significant advances have occurred in laparoscopic methods. When compared with the open technique, laparoscopy is associated with a shorter period of hospitalization and earlier returns to work [1]. Regarding these benefits, as well as the significant reduction in postoperative pain, laparoscopic hernia repair has gained widespread acceptance by surgeons and their patients [2–8].
Among available laparoscopic methods, two are used most frequently: “transabdominal preperitoneal (TAPP)” and “totally extraperitoneal (TEP)” laparoscopic hernia repair. In the TAPP method, the subject of the present trial, intra-abdominal synthetic mesh is fixed via different methods. Inadequate or inappropriate mesh fixation is the major cause of hernia recurrence in patients who have undergone TAPP [9–12].
Most frequently, mesh fixation is accomplished with the use of a stapler that delivers titanium tackers. Tackers not only reduce the hazard of mesh migration, they also maintain the optimum strength of the repair [13, 14]. However, neuralgia resulting from nerve entrapment in tackers has been reported [15–17].
In the inguinal region the nerves most prone to injury in TAPP are the lateral cutaneous nerve of the thigh, ilioinguinal nerves, and iliohypogastric nerves. In view of the importance attributed to days of pain relief after surgery, postoperative pain reduction has gained importance in evaluations of laparoscopic surgery [18].
Of complications related to hernia repair technique, seroma is one of the most frequent. Its importance relates to the patient’s assumption that the bulging appearance at the surgery site represents hernia recurrence [19].
The aim of the present study was to identify morbidities associated with TAPP repair, namely postoperative pain and hernia recurrence after two methods of mesh fixation: staple tackers and a hand-sewn method that we assume is worth introducing.
Methods
Between March 2012 and February 2013, after providing written consent, 70 patients with unilateral inguinal or femoral hernia were enrolled into the study, which was conducted at the Esfahan Alzahra Training Hospital. Inclusion criteria were age >18 years, American Society of Anesthesiologists (ASA) score of I or II, and no comorbidity that contraindicated general anesthesia and laparoscopic surgery. Exclusion criteria included ASA III or IV, large scrotal hernia, opium or alcohol addiction, prostatism, morbid obesity, bilateral inguinal hernia, and prior laparoscopic hernia repair. The flow diagram of patient enrolment into the study is included in Fig. 1.

The flow diagram of progress through the phases of a parallel randomized trial of two groups
With a table of random numbers, patients were divided randomly into two groups; (group 1 = Tacker group) (group 2 = Vicryl group).
Two surgeons, both trained in advanced laparoscopic surgery in a single unit and expert in laparoscopic TAPP hernia repair, were assigned to perform the operations. Another investigator was enrolled to record preoperative patient characteristics. To make the study double blinded, one more investigator was assigned to collect the postoperative and follow up data. None of the investigators were aware of correlating group, preoperative data, and postoperative data.
Surgery method
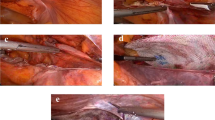
For TAPP laparoscopic hernia repair, before anesthesia induction, 1 g of cefazolin was injected. After induction of general anesthesia and endotracheal intubation, CO2 insufflation was performed via Veress needle. The patient was placed in the Trendlenberg position, and a 10 mm trocar was introduced via the umbilicus. The laparoscope was inserted, and intra-abdominal exploration was performed. If a unilateral inguinal or femoral hernia was documented, additional ports were inserted. For the unilateral procedure, a 5 mm ipsilateral port was inserted 1 in. above the umbilicus in the midclavicular line. Formal dissection of the hernia region was performed, and after creating a peritoneal window and dissecting the hernia sac, a 10 × 15 cm synthetic polypropylene mesh was inserted. In the first group mesh fixation was done with a single suture of 2–0 Vicryl that was anchored to the suprapubic region. In the second group mesh was fixed with three titanium tacks in the same location used for placement of the Vicryl suture in the first group. After completion of mesh fixation, the peritoneal window was closed with 2–0 Prolene. Trocars were extracted and abdominal gas emptied. The umbilical fascia and port site incisions were repaired, and the patient was transferred to the recovery room. Postoperative orders included a uniform set of analgesics for all patients:
-
Narcotics (pethidine 25 mg q8h)
-
Nonsteroidal anti-inflammatory drugs (NSAIDs) (diclofenac suppository 50 mg q8h)
Postoperation day
On the first postoperative day, the patient’s pain score, based on the visual analogue scale (VAS), and the amount of analgesic consumed were recorded.
If no complications occurred during the operation and the patient was able to tolerate an oral diet and was in good condition, he/she was discharged on the first postoperative day with an analgesic prescription (the dosage of the analgesic was again uniform for all patients):
-
Acetaminophen: 500 mg q8h
-
Diclophenac suppository: 50 mg q8h
Patients were instructed to complete a form at home, recording the VAS and the amount of analgesic required; the completed form was to be brought to the follow-up visit 1 week after operation.
At that first weekly postoperative visit, aside from examining the inguinal region for any sign of hematoma or seroma formation and the presence of neuralgia, a follow-up plan was also scheduled for visits at 1, 3, and 6 months after surgery. At each follow-up visit the search for hematoma, seroma, orchitis, mesh infection signs, neuralgia, and hernia recurrence was performed.
Statistical goals
This study was intended to show equal or better outcomes after mesh fixation with Vicryl suture rather than titanium tacks, with reference to specific points of interest that included postoperative pain, neuralgia, and long-term hernia recurrence.
Ethics
After we received written informed consent approval from the Esfahan University of Medical Science Ethics Committee on Medical Research, Esfahan, Iran (based on the World Medical Association Declaration of Helsinki regarding ethical conduct of research), each patient’s enrolment into the study was registered (Iranian Registry of Clinical Trials [IRCT] and the study was recorded as trial number: IRCT201202118972N1).
Results
This trial included 70 patients with inguinal hernia with a mean age of 43 years (range: 18–88 years). Comparing the demographics of the groups statistically, the two groups were equal (see Table 1).
After the surgery, no intraoperative complication was observed, and all patients stayed only one night in the hospital (see Table 2). At discharge, each patient was asked to avoid work for 7 days, and after the follow-up visit on the seventh day, all of them were fit to return to their occupations.
On the morning after surgery patients were instructed to score their pain. The Vicryl group patients had a lower mean VAS score than the tacker group patients. Mean analgesic consumption was also lower in the Vicryl group. Comparison of the VAS score and analgesic consumption on the first postoperative day and night did not reveal significant differences between the groups. None of the patients in either group had urinary retention, hematoma, or seroma in the inguinal region, and none of them complained of neuralgia (see Table 3).
At the first week follow-up visit the questionnaires recording the first week’s VAS scores were returned by patients. Statistical analysis revealed that patients in Vicryl group had lower mean VAS scores and on postoperative days 1 and 6 this difference was statistically significant.
The number of days on which patients consumed analgesics at home was also significantly fewer in the Vicryl group. After 1 week, there was no evidence of seroma, hematoma, neuralgia, orchitis, or signs of mesh infection in patients in either group. On follow-up visits after 1, 3, and 6 months, we did not observe complications or recurrence in any patient (see Table 4).
Discussion
With advancements in laparoscopic surgery, inguinal hernia repair with laparoscopic method has gained major acceptance by both surgeons and their patients. The method is associated with less postoperative pain, and return to work is earlier [5–8].
Among laparoscopic methods, transabdominal preperitoneal (TAPP) hernia repair was practiced in the present trial. With this method, synthetic mesh is fixed to the anterior abdominal wall, behind a peritoneal flap that inhibits adherence of the mesh to the viscera. The most common means of mesh fixation is the use of titanium tackers applied on the suprainguinal abdominal wall intersurface. Mesh fixation is a critical part of the operation and can be associated with important complications such as vascular or neuronal injury [7, 20, 21]. According to most previous studies, neuralgia is observed in 0.5–14 % of hernia repairs that use titanium tackers [22–24]. The inguinal nerves most vulnerable to injury are the genitofemoral nerve, the lateral cutaneous nerve of the thigh, and the ilioinguinal and iliohypogastric nerves [1], of which the lateral cutaneous nerve of the thigh is the most commonly injured in 0.1–10 % of cases [5, 6, 8, 25, 26, 27, 28]. Neural injury occurs as a result of nerve entrapment in the staple tacks. Stark et al. [16] reported a 4.2 % incidence of neuralgia. Some trials have reported suprapubic or pelvic pain following TAPP repair [1]. Tetik et al. [10] reported two cases of neural complication that needed reoperation among 1,514 patients undergoing TAPP repair. Sayad et al. [29] mentioned 2 % prevalence of neuralgia and a 0.4 % incidence of chronic pain among 9,955 TAPP repairs.
Considering the findings mentioned above, it can be assumed that neuralgia is a burden after TAPP hernia repair. Some methods are being used for reduction of tacker neural complications; namely, vertical orientation of the stapling device when placing the tacks and reduction in the number of tacks used [5, 20, 30]. Smith et al. [12] and Ferzli et al. [31] demonstrated that there is no need for fixing the mesh to the abdominal wall. At the same time studies have indicated that hernia recurrence is believed to be related to inappropriate mesh fixation [31–33]. For this reason, some authors have practiced methods that use a material other than titanium staple tacks, such as Tissucol [1] and fibrin sealant [19] for mesh fixation. These newer methods are associated with lower cost, a lower incidence of neuralgia, and fewer cases of seroma [5, 34, 35].
In the present study we used a single absorbable Vicryl suture to fix the mesh. It has some benefits; namely, lower cost (about 1 USD for a single suture in comparison with tacks that cost about 100 USD), lower VAS scores after surgery, and reduced analgesic consumption. With the Vicry suture there were no cases of neuralgia in our series. Actually, risk of nerve entrapment was eliminated with this method. The only concern was the possibility of hernia recurrence. Fortunately, at 6 months follow-up there were no cases of recurrence.
Considering postoperative complications such as seroma and hematoma, we believe that meticulous surgical technique used in this study is of paramount importance in reducing complications. Another possibility could be the number of patients enrolled in this study. Although after 6 months of follow-up we did not observe any hernia recurrence in Vicryl group, it is assumed that longer follow-up would be of benefit. We therefore intend to continue the trial, both to enlarge the data mass and to provide longer follow-up of our patients.
Conclusions
According to data obtained in this study, mesh fixation with a single absorbable Vicryl suture in comparison to titanium tackers is associated with less pain and analgesic consumption after surgery. The risk of neuralgia because of nerve entrapment was thereby omitted, and at 6 months follow-up the incidence of hernia recurrence is not more than tacker fixation. This method can be an alternative to conventional mesh fixation methods.
References
Lovisetto F, Zonta S, Rota E, Mazzilli M, Bardone M, Bottero L, Faillace G, Longoni M (2007) Use of human fibrin glue (Tissucol) versus staples for mesh fixation in laparoscopic transabdominal preperitoneal hernioplasty: a prospective, randomized study. Ann Surg 245:222–231
Liem MS, van der Graaf Y, van Steensel CJ, Boelhouwer RU, Clevers GJ, Meijer WS, Stassen LP, Vente JP, Weidema WF, Schrijvers AJ, van Vroonhoven TJ (1997) Comparison of conventional anterior surgery and laparoscopic surgery for inguinal hernia repair. N Engl J Med 336:1541–1547
MRC Laparoscopic Groin Hernia Trial Group (1999) Laparoscopic versus open repair of groin hernia: a randomized comparison. Lancet 354:185–190
Bringman S, Ramel S, Heikkinen TJ, Englund T, Westman B, Anderberg B (2003) Tension-free inguinal hernia repair: TEP versus mesh-plug versus Lichtenstein. A prospective randomized controlled trial. Ann Surg 237:142–147
Bueno J, Serralta A, Planells M, Rodero D (2004) Inguinodynia after two inguinal herniorrhaphy methods. Surg Laparosc Endosc Percutan Tech 14:210–214
Mahon D, Decadt B, Rhodes M (2003) Prospective randomized trial of laparoscopic (transabdominal preperitoneal) vs open (mesh) repair for bilateral and recurrent inguinal hernia. Surg Endosc 17:1386–1390
Onofrio L, Cafaro D, Manzo F, Cristiano SF, Sgromo B, Ussia G (2004) Tension-free laparoscopic versus open inguinal hernia repair. Minerva Chir 59:369–377
Smith JR, Demers ML, Pollack R, Gregory S (2001) Prospective comparison between laparoscopic preperitoneal herniorrhaphy and open mesh herniorrhaphy. Am Surg 67:11–17
Lowham AS, Filipi CJ, Fitzgibbons RJ Jr, Stoppa R, Wantz GE, Felix EL, Crafton WB (1997) Mechanism of hernia recurrence after preperitoneal mesh repair: traditional and laparoscopic. Ann Surg 225:422–431
Tetik C, Arregui ME, Dulucq JL, Fitzgibbons RJ, Franklin ME, McKernan JB, Rosin RD, Schultz LS, Toy FK (1994) Complications and recurrences associated with laparoscopic repair of groin hernias: a multi-institutional retrospective analysis. Ann Surg 8:1316–1323
Felix E, Scott S, Crafton B, Geis P, Duncan T, Sewell R, McKernan B (1998) Causes of recurrence after laparoscopic hernioplasty: a multicenter study. Surg Endosc 12:226–231
Phillips EH, Rosenthal R, Fallas M, Carroll B, Arregui M, Corbitt J, Fitzgibbons R, Seid A, Schultz L, Toy F (1995) Reasons for recurrence following laparoscopic hernioplasty. Surg Endosc 9:140–145
Dion YM, Laplante R, Charara J, Marois M (1994) The influence of the number of endoclips and of mesh incorporation on the strength of an experimental hernia patch repair. Surg Endosc 8:1324–1328
Hollinsky C, Gobl S (1999) Bursting strength evaluation after different types of mesh fixation in laparoscopic herniorrhaphy. Surg Endosc 13:958–961
Eubanks S, Newman L III, Goehring L, Lucas GW, Adams CP, Mason E, Duncan T (1993) Meralgia paresthetica: a complication of laparoscopic herniorrhaphy. Surg Laparosc Endosc 3:381–385
Stark E, Oestreich K, Wendl K, Rumstadt B, Hagmüller E (1999) Nerve irritation after laparoscopic hernia repair. Surg Endosc 13:878–881
Tucker JG, Wilson RA, Rarnshaw BJ, Mason EM, Duncan TD, Lucas GW (1995) Laparoscopic herniorrhaphy: technical concerns in prevention of complications and early recurrence. Am Surg 61:36–39
Lau H, Patil NG (2004) Acute pain following endoscopic totally extraperitoneal (TEP) inguinal hernioplasty: multivariate analysis of predictive factors. Surg Endosc 18:92–96
Lau H (2005) Fibrin sealant versus mechanical stapling for mesh fixation during endoscopic extraperitoneal inguinal hernioplasty: a randomized prospective trial. Ann Surg 242:670–675
Katkhouda N (2004) A new technique for laparoscopic hernia repair using fibrin sealant. Surg Technol Int 12:120–126
Langrehr JM, Schmidt SC, Neuhaus P (2005) Initial experience with the use of fibrin sealant for the fixation of the prosthetic mesh in laparoscopic transabdominal preperitoneal hernia repair. Rozhl Chir 84:399–402
Rosier EM, Iadarola MJ, Coghill RC (2002) Reproducibility of pain measurement and pain perception. Pain 98:205–216
Felix EL, Michas CA, McKnight RL (1994) Laparoscopic repair of recurrent groin hernias. Surg Laparosc Endosc 4:200–204
Kapiris SA, Brough WA, Royston CM, O’Boyle C, Sedman PC (2001) Laparoscopic transabdominal preperitoneal (TAPP) hernia repair. Surg Endosc 15:972–975
Quilici PJ, Greaney EM Jr, Quilici J, Anderson S (2000) Laparoscopic inguinal hernia repair: optimal technical variations and results in 1700 cases. Am Surg 66:848–852
Totte E, Van Hee R, Kox G, Hendrickx L, van Zwieten KJ (2005) Surgical anatomy of the inguinal region: implications during inguinal laparoscopic herniorrhaphy. Eur Surg Res 37:185–190
Broin EO, Horner C, Mealy K, Kerin MJ, Gillen P, O’Brien M, Tanner WA (1995) Meralgia paresthetica following laparoscopic inguinal hernia repair: an anatomical analysis. Surg Endosc 9:76–78
Felix EL, Harbertson N, Vartanian S (1999) Laparoscopic hernioplasty: significant complications. Surg Endosc 13:328–331
Sayad P, Hallak A, Ferzli G (1998) Laparoscopic herniorraphy: review of complications and recurrence. J Laparoendosc Adv Surg Tech 3:381–385
Katkhouda N, Mavor E, Friedlander MH, Mason RJ, Kiyabu M, Grant SW, Achanta K, Kirkman EL, Narayanan K, Essani R (2001) Use of fibrin sealant for prosthetic mesh fixation in laparoscopic extraperitoneal inguinal hernia repair. Ann Surg 233:18–25
Ferzli GS, Frezza EE, Pecoraro AM Jr, Ahern KD (1999) Prospective randomized study of stapled versus unstapled mesh in a laparoscopic preperitoneal inguinal hernia repair. J Am Coll Surg 188:461–465
Khajanchee YS, Urbach DR, Swanstrom LL, Hansen PD (2001) Outcomes of laparoscopic herniorrhaphy without fixation of mesh to the abdominal wall. Surg Endosc 15:1102–1107
Lau H, Patil NG (2003) Selective non-stapling of mesh during unilateral endoscopic total extraperitoneal inguinal hernioplasty: a case-control study. Arch Surg 138:1352–1355
Fernandez Lobato R, Garcia Septiem J, Ortega Deballon P, Martín Lucas FJ, Ruíz de Adana JC, Limones Esteban M (2001) Tissucol application in dermolipectomy and incisional hernia repair. Int Surg 86:240–245
McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E, Vale L, Grant A (2005) Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation. Health Technol Assess 9:1–203
Disclosure
Authors Behrooz Kleidari, Mohsen Mahmoudieh, Mohammad Yaribakht, and Zhila Homaei have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kleidari, B., Mahmoudieh, M., Yaribakht, M. et al. Mesh fixation in TAPP laparoscopic hernia repair: introduction of a new method in a prospective randomized trial. Surg Endosc 28, 531–536 (2014). https://doi.org/10.1007/s00464-013-3198-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-3198-7