
Abstract
Background
Laparoscopic cholecystectomy (LC) is safe in acute cholecystitis, but the exact timing remains ill-defined. This study evaluated the effect of timing of LC in patients with acute cholecystitis.
Methods
Prospective data from the hospital registry were reviewed. All patients admitted with acute cholecystitis from June 1994 to January 2004 were included in the cohort.
Results
Laparoscopic cholecystectomy was attempted in 1,967 patients during the study period; 80% were women, mean patient age was 44 years (range, 20–73 years). Of the 1,967 LC procedures, 1,675 were successful, and 292 were converted to an open procedure (14%). Mean operating time for LC was 1 h 44 min (SD ± 50 min), versus 3 h 5 min (SD ± 79 min) when converted to an open procedure. Average postoperative length of stay was 1.89 days (± 2.47 days) for the laparoscopic group and 4.3 days (± 2.2 days) for the conversion group. No clinically relevant differences regarding conversion rates, operative times, or postoperative length of stay were found between patients who were operated on within 48 h compared to those patients who were operated on post-admission days 3–7.
Conclusions
The timing of laparoscopic cholecystectomy in patients with acute cholecystitis has no clinically relevant effect on conversion rates, operative times, or length of stay.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The surgical management of patients with acute cholecystitis remains controversial. While some surgeons may have concerns that early surgery is associated with increased operative difficulty and consequently higher morbidity and conversion rates, these concerns are not substantiated by recent experience. Laparoscopic cholecystectomy (LC) was found to be safe in cases of acute cholecystitis [4, 9]. Prospective and retrospective studies found no significant differences between early or interval LC [14, 15]. The timing of operation was felt to be important to the results, but the exact timing remains ill-defined. Previous prospective and retrospective studies have failed to demonstrate statistical differences between early and late cholecystectomy [2, 4]. On the other hand, there is accumulating evidence that delayed operation is accompanied with higher rates of conversion and complications. Eldar and colleagues performed a prospective study and found a 23% conversion rate when the procedure was delayed by 96 h, and a 47% conversion rate beyond 96 h. The complication rates were higher in the conversion group (27%) compared to the laparoscopy group (8.5%) [9]. A 5-day delay was found to have a conversion rate of 26% compared to 3.6% in the earlier group [10]. Other reports have suggested the best time for surgical intervention is anywhere from 72 h from the onset of symptoms [11] to 48 h [16], 3 days [17], or even 4 days [20].
Laparoscopic cholecystectomy is the treatment of choice for chronic and acute cholecystitis in our institution. Although routinely performed, the timing of the operation is subject to many factors. Because the optimal timing of the operation is not well defined, the timing of the procedure differs. Identification of the optimal timing of operation in the case of acute cholecystitis would permit the adoption of a uniform approach, which potentially offers a better outcome for the patients and could lead to a shorter hospital stay [21].
Patients and methods
All patients admitted with acute cholecystitis to the University of Miami/Jackson Memorial Hospital, Miami, Florida from June 1994 to January 2004 were included in the study cohort. The University of Miami Institutional Review Board approved this study prior to the initiation of data collection. The prospectively collected data from the hospital registry were reviewed. Patients who had a diagnosis of acute cholecystitis and who had an attempted LC procedure during the time of admission were included. Patients who had incomplete data, those who were not operated on, and those who had an open cholecystectomy to begin with were excluded. Demographics, physiological and laboratory parameters, as well as time from admission to operation, length of operation, conversion from laparoscopic cholecystectomy to open cholecystectomy, complications, and postoperative hospital stay were included in the analysis.
All patients in the registry were followed for the full length of their hospital stay, and both length of stay and discharge disposition information were available. Data are expressed as mean ± standard deviation (SD) or proportions. A z-test was used for detecting differences in proportions, and the Student t-test was used for continuous variables. Multiple logistic regression analysis (SPSS version 10.1, SPSS, Inc.) was used to determine the independent effects of age, gender, initial whole blood count (WBC), and hospital stay before operation on the need for conversion to an open procedure. A value of p < 0.05 was considered statistically significant.
Results
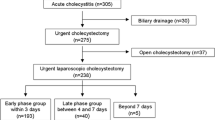
The initial database consisted of 2,168 patients admitted urgently with the diagnosis of acute cholecystitis. Of these, 190 had acute biliary pancreatitis as a primary or secondary diagnosis and were therefore excluded. Eleven other patients were excluded because of incomplete data. Of the remaining 1,967 patients, 393 were men (20%) and 1,574 were women (80%). The mean age was 44 years, with a standard deviation of 16 and an age range of 20–73 years. The patients were divided into seven different groups according to their post-admission operative day. The number of patients operated on by day post admission, the conversion rate for each group, the postoperative length of hospital stay, and the time for completion of the operation are listed in Table 1.
In this series, 1,675 patients had a successful LC, and 292 were converted to an open procedure (14.8%). The average operating time for completion of the procedure was 1 h and 56 min. The average postoperative length of stay was 2.23 ± 2.59 days for all patients. No clinically significant differences were found regarding conversion rates, operating time, or postoperative length of stay between patients who were operated on post-admission day 1 or 2 compared to those patients who were operated on post admission days 3–7. Considering patients whose procedure was converted to open cholecystectomy as a different group, we separated them from the entire cohort as described in the demographic data shown in Table 2. Patients who were converted were older (47 ± 15 versus 42 ± 14, t-test p < 0.005) and more likely to be male (t-test p < 0.001) than those whose procedure was completed laparoscopically. The average time for laparoscopic cholecystectomy was 1 h and 44 min (SD ± 50 min), compared to 3 h and 5 min (SD ± 1 h and 19 min) when converted to an open procedure (p < 0.001). The average length of stay was 1.89 days (SD ± 2.47 days) for the laparoscopic group and 4.3 days (SD ± 2.2 days) for the conversion group (p < 0.001), as described in Table 3. The only significant statistical difference in length of stay was found among patients who were operated on day 1 compared to those operated on day 6 (Table 4), and this difference of a half-day’s hospitalization is of questionable clinical relevance. No difference was found regarding conversion rates between patients who were operated on post admission day 1 and 2 compared to those who were operated on post-admission days 3–7. There were statistically significant differences in operative times between those operated on day 1 compared to days 6 and 7, but again this difference of 11 and 12 min, respectively, is likely not clinically relevant. Patients who were operated and converted on post-admission day 1 had a longer length of stay and a longer procedure time than those who were operated on day 6 (Table 5). Using multiple logistic regression, only patient age (p < 0.001) and gender (p < 0.001) were associated with the need for conversion to an open procedure. The initial WBC (p = 0.38) and length of stay prior to operation (p = 0.51) was not associated with the need for conversion to an open procedure.
There were five major biliary (duct) injuries (0.3%), defined as any accidental puncture or laceration to a major bile duct such as the common, right, or left hepatic duct, one on day 1, two on day 3, and two on day 4. Four of these injuries occurred during the laparoscopic procedure and only one occurred after conversion. There were three iatrogenic enterotomies (0.2%), all of which occurred during the laparoscopic procedure.
Discussion
Laparoscopic cholecystectomy is considered the treatment of choice for patients with symptomatic cholelithiasis. First executed on an elective basis, the procedure proved to be superior in many ways to open cholecystectomy. As more experience was gained with the laparoscopic technique it was only natural that its boundaries of utilization would be expanded. Indeed, it was believed by many surgeons that laparoscopic cholecystectomy carried a high risk when used for the treatment of acute cholecystitis and that the open procedure should remain the only treatment. Some authors advocated the “interval cholecystectomy” as the preferred method, in which antibiotic treatment or percutaneous drainage of the infected gallbladder served as a bridge to elective laparoscopic surgery, which was done after the patient’s disease had “cooled down” [6]. Recent studies, prospective and retrospective, have demonstrated that laparoscopic cholecystectomy for acute cholecystitis is as safe as the open technique, and it carries the same rates of complication while exerting all the benefits of laparoscopic surgery, such as shorter length of hospital stay, reduced postoperative pain, a better cosmetic result, and a faster return to normal activity [9].
While laparoscopic cholecystectomy has gained a leading role in the treatment of acute cholecystitis, despite higher reported rates of conversion to open surgery (14%–26%), there is still some debate as to the optimal timing of the operation. Several clinical studies showed higher rates of conversion when the procedure was done beyond the first two days of disease, as well as higher complication rates. In contrast, several other studies have failed to show that tendency. Our results show that, even in a teaching hospital, conversion rates are relatively higher in elective cases (8.8%–16.5%), but still lower than one would expect based on previous reports. Most important, conversion rates were not influenced by the timing of surgery.
We chose to use the day of admission as a reference for time measurement instead of the first day of symptoms. Eldar and colleagues used the first day of symptoms as a reference and found higher conversion rates (39%), but no increase in complication rates with delays of more than 48 h, and this finding was supported by others [5, 7, 18]. Onset of symptoms is a subjective parameter, and therefore in many hospitals it is the day of admission and the initiation of conservative treatment that is the main guide to operative scheduling [2].
Other factors that may influence the need for conversion to open surgery were identified, and most were related to the severity of the disease and not to the day of operation. Koperna and colleagues found higher conversion rates related to higher WBC counts and the presence of empyema of the gallbladder [12]. Age older than 60 years, history of biliary disease, pericholecystic collections seen on ultrasound, gallbladder wall thickening greater than 5 mm, and male gender were also identified as risk factors for conversion [7, 19]. In our study, multiple regression analysis failed to show any association between initial WBC or preoperative length of stay and the need for conversion to an open procedure. However, as in previous studies, age and male sex were also risk factors for conversion in our study.
The lower conversion rate and the lack of statistical difference among different days of surgery might be explained by the large number of operations done in our hospital in the acute phase of the disease, as well as by the fact that many patients are operated on several days after their admission. That variety in numbers and different disease stages might contribute to better experience and better results, especially the accumulation of experience by the attending surgeons. That expertise theory does not stand along with the fact that most of these operations were done, as in most teaching hospitals, by heterogeneous teams made up mainly of residents and fellows. Bender and colleagues suggested that increased laparoscopic experience does not lead to improved results with acute cholecystitis, because in their study, better experience did not change the conversion rates [1]. The assumption that the technical difficulty of the procedure is reflected by its length was supported by the fact that open cholecystectomies (laparoscopic converted to open surgery) took more time to complete than laparoscopic cholecystectomies. That difference remained statistically significant at all times of operations studied.
At our institution there is no “conservative treatment policy” because all patients sick enough to warrant admission are operated on for their disease prior to discharge. There might be some bias toward patients with fulminant or nonresponsive cholecystitis (failure to improve with medical management), as they may tend to be operated on sooner than others. Our policy, however, is that the ideal timing of surgery for all patients admitted to the hospital for acute cholecystitis is close to or after 48 h, whether they are responding to medical treatment or not. As with many large public teaching hospitals, delays do occur due to administrative problems such as unavailability of an operating room.
Although a difference in operative time was found between days 1 and 2 compared to day 6, the fact that it was only an extra 10 min in the length of the procedure (Table 2) makes this statistical finding clinically unimportant. Patients who were converted on day one post-admission had a longer operative time and a longer length of hospital stay. This might be explained by the assumption that this group of patients represents the sicker ones, but because no grading system is available to classify patients with acute cholecystitis into severity groups, we cannot prove that assumption.
The length of hospital stay was found to be longer in the converted group than in the laparoscopic group, but no statistical difference was found among the different laparoscopic groups, except for those who were operated on post-admission day 6. That difference of an extra 0.5 hospital day, although statistically significant, represents little clinical relevance.
In our series major bile duct injuries occurring during the laparoscopic procedure resemble those of other elective cholecystectomy reports (0.3%) [13]. There is insufficient power to analyze whether there is a difference in iatrogenic bile duct injuries.
The finding that the timing of LC and the natural history of acute cholecystitis does not affect the conversion rate, hospital stay, or complication rate does contradict other studies, as noted previously. This may be related in part to our policy that all patients are operated on prior to discharge. Our successful operative management of these patients at all times of their hospital stay may reflect our comfort level using this policy and the standardized approach to their treatment. Clearly, institution-specific factors may be at play that cannot be easily defined in this retrospective study. Our patient management has not changed based on these results, but we are better able to be confident that our policy is safe and effective and better able to inform our patients about the risks of the procedure, regardless of its timing.
In conclusion, there is no optimal timing for laparoscopic cholecystectomy in acute cholecystitis. The chances that the procedure will be converted are related to age and gender (male sex). Laparoscopic cholecystectomy as a treatment for acute cholecystitis is safe and carries the same risk for major bile duct injuries and other iatrogenic complications as in elective cases.
References
Bender JS, Duncan MD, Freeswick PD, Harmon JW, Magnuson TH (2002) Increased laparoscopic experience does not lead to improved results with acute cholecystitis. Am J Surg 184:591–594; discussion 594–595
Bhattacharya D, Senapati PS, Hurle R, Ammori BJ (2002) Urgent versus interval laparoscopic cholecystectomy for acute cholecystitis: a comparative study. J Hepatobiliary Pancreat Surg 9:538–542
Bittner R, Leibl B, Kraft K, Butters M, Nick G, Ulrich M (1997) Laparoscopic cholecystectomy in therapy of acute cholecystitis: immediate versus interval operation. Chirurg 68:237–243
Chandler CF, Lane JS, Ferguson P, Thompson SW (2000) Prospective evaluation of early versus delayed laparoscopic cholecystectomy for treatment of acute cholecystitis. Am Surg 66:896–900
Cheema S, Brannigan AE, Johnson S, Delaney PV, Grace PA (2003) Timing of laparoscopic cholecystectomy in acute cholecystitis. Ir J Med Sci 172:128–131
Chikamori F, Kuniyoshi N, Shibuya S, Takase Y (2002) Early scheduled laparoscopic cholecystectomy following percutaneous transhepatic gallbladder drainage for patients with acute cholecystitis. Surg Endosc 16:1704–1707
Eldar S, Eitan A, Bickel A, Sabo E, Cohen J, Abrahamson J, Matter I (1999) The impact of patient delay and physician delay on the outcome of laparoscopic cholecystectomy for acute cholecystitis. Am J Surg 178:303–307
Eldar S, Sabo E, Nash E, Abrahamson J, Matter I (1997) Laparoscopic cholecystectomy for acute cholecystitis: prospective trial. World J Surg 21:540–545
Eldar S, Sabo E, Nash E, Abrahamson J, Matter I (1997) Laparoscopic versus open cholecystectomy in acute cholecystitis. Surg Laparosc Endosc 7:407–414
Garber SM, Korman J, Cosgrove JM, Cohen JR (1997) Early laparoscopic cholecystectomy for acute cholecystitis. Surg Endosc 11:347–350
Koo KP, Thirlby RC (1996) Laparoscopic cholecystectomy in acute cholecystitis. What is the optimal timing for operation? Arch Surg 131:540–544; discussion 544–545
Koperna T, Kisser M, Schulz F (1999) Laparoscopic versus open treatment of patients with acute cholecystitis. Hepatogastroenterology 46:753–757
Krahenbühl L, Sclabas G, Moritz N, Wente M, Schäfer R, Schlumpf R, Büchler MW (2001) Incidence, risk factors, and prevention of biliary tract injuries during laparoscopic cholecystectomy in Switzerland. World J Surg 25:1325–1330
Lo CM, Liu CL, Lai EC, Fan ST, Wong J (1996) Early versus delayed laparoscopic cholecystectomy for treatment of acute cholecystitis. Ann Surg 223:37–42
Lo CM, Liu CL, Lai EC, Fan ST, Wong J (1998) Prospective randomized study of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Ann Surg 227:461–467
Madan AK, Aliabadi-Wahle S, Tesi D, Flint LM, Steinberg SM (2002) How early is early laparoscopic treatment of acute cholecystitis? Am J Surg 183:232–236
Pessaux P, Tuech JJ, Regenet N, Fauvet R, Boyer J, Arnaud JP (2000) Laparoscopic cholecystectomy in the treatment of acute cholecystitis. Prospective non-randomized study. Gastroenterol Clin Biol 24:400–403
Pessaux P, Tuech JJ, Rouge C, Duplessis R, Cervi C, Arnaud JP (2000) Laparoscopic cholecystectomy in acute cholecystitis. A prospective comparative study in patients with acute vs. chronic cholecystitis. Surg Endosc 14:358–361
Prakash K, Jacob G, Lekha V, Venugopal A, Venugopal B, Ramesh H (2002) Laparoscopic cholecystectomy in acute cholecystitis. Surg Endosc 16:180–183
Suter M, Meyer A (2001) A 10-year experience with the use of laparoscopic cholecystectomy for acute cholecystitis: is it safe? Surg Endosc 15:1187–1192
Wu X, Merchuk JC (2002) Simulation of algae growth in a bench-scale bubble column reactor. Biotechnol Bioeng 80:156–168
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Soffer, D., Blackbourne, L.H., Schulman, C.I. et al. Is there an optimal time for laparoscopic cholecystectomy in acute cholecystitis?. Surg Endosc 21, 805–809 (2007). https://doi.org/10.1007/s00464-006-9019-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-006-9019-5