
Abstract
Background
Laparoscopic cholecystectomy (LC) combined with intraoperative endoscopic sphincterotomy (IOEST) was compared with laparoscopic exploration of the common bile duct (LCBDE) for cholecystocholedocholithiasis in an attempt tried to find the best mini-invasive treatment for the cholelithiasis and choledocholithiasis.
Methods
For this study, 234 patients with cholelithiasis and choledocholithiasis diagnosed by preoperative B-ultrasonography and intraoperative cholangiogram were divided at random into an LC-LCBDE group (141cases) and an LC-IOEST group (93 cases). The surgical times, surgical success rates, number of stone extractions, postoperative complications, retained common bile duct stones, postoperative lengths of stay, and hospital charges were compared prospectively.
Results
There were no differences between the two groups in terms of surgical time, surgical success rate, number of stone extractions, postoperative complications, retained common bile duct stones, postoperative length of stay, and hospital charge.
Conclusion
Both LC-IOEST and LC-LCBDE were shown to be safe, effective, minimally invasive treatments for cholecystocholedocholithiasis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
It is reported that laparoscopic cholecystectomy (LC) could be carried out for 95% of cholelithiasis cases in the hospitals with the laparoscopic devices available, whereas 70% to 90% of extrahepatic duct stones could be treated by a mini-invasive procedure using three kinds of endoscopes: (laparoscope, pancreatocholedochoscope and choledochoscope) [7]. Currently, it still is controversial how these three mini-invasive procedures should be combined to achieve the best result due to the lack of research involving large series [4, 9, 18]. We prospectively compared laparoscopic exploration of the common bile duct (LC-LCBDE) and laparoscopic cholecystectomy combined with intraoperative endoscopic sphincterotomy (LC-IOEST) and report the results.
Materials and methods
General conditions
From January 2002 to December 2003, 234 cases of cholelithiasis with extrahepatic duct stones diagnosed by history, physical examination, ultrasonography, magnetic resonance cholangiopancreatography (MRCP), or cholangiogram through cystic duct cannulation were treated. They were randomized into a LC-CBDE group (141 cases) and a LC-IOEST group (93 cases) according their identifying numbers. All the patients were informed about both the procedure and the technology, and all signed informed consent forms. The ultrasonographic findings were positive in 174 cases. Three cases had positive MRCP findings, and 57 cases had positive intraoperative cholangiogram (IOC) findings without a preoperative diagnosis of extrahepatic duct stones [3].
The postoperative diagnosis was acute cholecystitis, cholelithiasis, and extrahepatic duct stone leading to acute obstructive suppurative cholangitis in 18 cases, and cholelithiasis with extrahepatic duct stone in 216 cases. Among the latter, there were 16 cases involving acute gallbladder pancreatitis and 48 cases involving jaundice. The LC-LCBDE group comprised 28 males and 65 females ranging from 15 to 82 years of age (mean, 48 years). There was no significant difference between the two groups in terms of age or preoperative history of primary hypertension and coronary heart disease.
Operative techniques
LC-IOEST technique [3, 5]
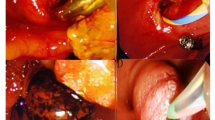
Laparoscopic cholecystectomy was performed using four trocars. We performed catheterization of the cystic duct and IOC using C-arm x-ray. If IOC yielded positive result, IOEST was performed by gastroenterologists with the equipment in the operating room. The patient was returned to the supine position. Pneumoperitoneum was canceled, and the nasogastric tube was removed. A pancreatocholangioscope (JF140 or JF100, Olympus) was inserted into the duodenal descending segment through the mouth. We performed retrograde endoscopic cholangiopancreatography (ERCP) before endoscopic sphincterotomy (EST). Small stones 5 to 8 mm in size could be cleared into the duodenum by saline irrigation using the cholangiographic catheter. Stones of 8 to 15 mm in size could be removed by basket or balloon catheter. Stones of larger than 15 mm were removed with a mechanical lithotriptor (replacement wire basket, MAJ-247; Olympus) during intraoperative endoscopic sphinicterotomy (IOEST). After biliary tract irrigation a second cholangiogram was performed to ensure that no stones had been retained. After the pancreatocholangioscope was removed, we created pneumoperitoneum and inserted a nasogastric tube to continue the LC.
LC-LCBDE technique
Laparoscopic cholecystectomy was performed using four trocars. The cystic duct as well as anterior and posterior walls of the common bile duct (CBD) were dissected. The distal cystic duct was clipped. Cannulation of the cholangiogram catheter proceeded was from the small incision in proximal cystic duct through the trocar on the right midclavicular line below the ribs. The catheter was fixed by clip. The trocar was removed, then inserted again for placement of the catheter attached to the outside of the trocar. If extrahepatic duct stone was detected by preoperative ultrasonography, we lifted the anterior wall of the CBD bile duct using the dissection clamp. A small incision is made, and the electric hook was used for hemastasis. After we had covered the Foley catheter or the irrigation catheter with a segment of a silicon tube, it was inserted into the CBD. The stone was flushed out or extracted after repeated saline irrigation of CBD. A cholangioscope was considered if stone removal failed. If we suspected CBD stone by clinical history or preoperative ultrasonography without demonstrated stones, cholangiogram through the cystic duct was performed [3, 9]. We opened the CBD in the case of positive cholangiography results. For sludge or a stone smaller than 10 mm in the CBD, irrigation through the catheter in cystic duct or introduction of a 3-mm cholangioscope into cystic duct was used in an attempt to clear the duct. If these procedures failed, opening of CBD was suggested.
A 5- or 3-mm cholangioscope was inserted into CBD through the 10-mm trocar in subxyphoid region. A multiple instrument guide (MIG) gave the 3-mm cholangioscope access to the CBD. The cholangioscope was connected with a monitor, and the stones were extracted by basket after we had checked the biliary tract upward and downward.
Primary closure of the CBD using 3-0 Vicryl or T-tube placement was performed after stone removal. We inserted the T-tube in 96 cases and used primary closure in 45 cases. After closure, a second cholangiogram through the cystic duct or T-tube was performed to rule out the retained stones and to ensure an unobstructed distal CBD. A J-P tube was maintained in the subhepatic space, then removed after 48 h.
Antibiotics were administered once preoperatively, then postoperatively for 1 or 3 days. No antibiotics were administered during the operation. On the second day, a semiliquid diet was given. Follow-up assessment using ultrasonography was carried out for 3 to 27 months, with MRCP or ERCP used when indicated.
Results
The surgical times, surgical success rates, stone numbers and sizes, retained stone incidences, complications, postoperative hospital lengths stay, and hospital charges were compared between the two groups.
Comparison of surgical results
There was no statistically significance difference in surgical time, surgical success rate, or stone number (sludge was excluded) between the two groups (Table 1). The surgical success rate for the LC-LCBDE group was 89.36% (126/141), with 15 cases converted to open surgery, 3 cases of which required IOEST because of stone removal failure, involving 1 basket intrapment, 7 CBD stone incarcerations, and 4 severe adhesions in Calot’s triangle.
The LC-IOEST success rate was 91.40% (85/93), with 8 cases converted to open surgery. The conversion include five cases of papilla knife insertion failure because of CBD stone impaction, two cases of severe adhesion in Calot’s triangle, and one case of papilla deformity. The diameter of the stone removed was 40 mm in the LC-LCBDE group and 15 mm in the LC-IOEST group.
Comparison of postoperative data
There were no significant differences in postoperative retained stones, complications, postoperative lengths of hospital stay, or hospital charges between the two groups (Table 2). Three cases of retained stone were found in the LC-LCBDE group and one case in the LC-IOEST group. All the retained stones were removed by postoperative EST. Seven cases involved complications, including four cases of asymptomatic serum amylase elevation (>1,000 I U/l), one case of pneumonia, one case of jaundice that did not improve (hepatitis B virus infection was suspected), and one case of bile leakage. Pleural effusion improved after conservative therapy.
Eight cases in the LC-IOEST group involved complications, including five cases of asymptomatic serum amylase elevation, one case of bile leakage cured by ultrasonography-guided drainage, one case of pneumonia, and one case of pancreatic pseudocyst with a preoperative diagnosis of acute biliary pancreatitis. One patient experienced recurrent jaundice with a diagnosis of acute obstructive suppurative cholangitis. The ERCP showed a 1 × 1-cm mass in the papilla and the pathologic report was adenocarcinoma. Thus, the patient was misdiagnosed because of suppurative and necrotic secretion coverage. He underwent the Whipple procedure.
The longest postoperative length of hospital stay was 32 days in the LC-LCBDE group and 27 days in the LC-IOEST group. In the one cases, there was no jaundice improvement, and HBV infection was suspected. The other case involved a postoperative complication of pneumonia and pancreatic pseudocyst. No deaths occurred.
Discussion
Because of applications involving EST, LC, and LCBDE, reports give increasing attention to mini-invasive treatment of peri-LC extrahepatic duct stones, and it has become the focus in recent mini-invasive biliary surgery.The following procedures are available:
-
No treatment for asymptomatic CBD stone while waiting for its natural clearance. For symptomatic cases after LC, EST is suggested [1].
-
Cannulation through the cystic duct to the CBD and duodenum for cholangiogram during LC or stone removal by EST [2, 14].
We reviewed the merits and faults of these procedures in literature and found the following:
-
It is not acceptable to suggest no treatment for asymptomatic CBD stone in Chinese patients.
-
It is time consuming to remove stones by cholangioscope during LC
-
A longer learning curve is required for LCBDE because of laparoscopic suture in T-tube placement.
-
Routine ERCP in pre-LC EST result in suffering and increased charge to patients. If elective ERCP is performed, 50% to 60% extrahepatic duct stone cases will show false-negative results. There still is a possibility of LC conversion to open procedure even if EST succeeds [3–5].
-
A second operation should be performed in post-LC EST failure cases.
-
EST during LC is better than pre- and post-LC EST, but needs more expertise and experience.
-
EST may cause Oddi’s sphincter dysfunction and still is controversial whether it leads to stone recurrence and biliary carcinoma caused by permanent duodenxal and pancreatic fluid reflux [2, 12, 13, 15].
With regard to the clinical effectiveness, as well as social and economy benefits, LC-IOEST and LC-LCBDE are the most ideal of the mini-invasive procedures. They are more and more prevalent [6, 8, 17]. We compared these two procedures and found no differences between them in terms of the surgical time, the number extracted of stones, the retained CBD stones, postoperative length of stay, and the hospital charge. For the LC-IOEST group, the rates were 89.38% surgical success and 91.4% complications, and the corresponding rates were 5.55% and 9.41% in the LC-LCBDE group. No deaths occurred.
Tranter and Thompson [15] reported the following rates: 79% to 98% (mean, 92%) for LC-EST success 75% to 96% (mean, 91%) for stone clearance, 0% to 6% (mean, 1%) for mortality, and 3% to 16% (mean, 13%) for complications.
For the LC-LCBDE group,the success rate was 80% to 99% (mean, 96%); the stone clearance rate was 81% to 100% (mean, 95%); the mortality rate was 0% to 5% (mean, 1%) and the complication rate was 2% to 17% (mean, 8%). Stone recurrence and biliary carcinoma were complications 10 years later, reaching rates of 16% and 2%, respectively. There still is a lack of large-sample controlled research.
To avoid the late complications, LCBDE is the procedure of choice when the operations are in competent hands. Sugiyama and Atomi [12] reported that EST caused transient bile and pancreatic fluid reflux, which disappeared 1 year later.The 10-year follow-up assesment did not show increasing of anaphase complications such as biliary carcinoma, cholangitis, or stone recurrence.
We concluded that stones larger than 20 mm are not suitable for stone removal by EST [10]. Excessive cutting of the sphincter may increase complications because cystic duct dilation and normal structure are required for LCBDE through it. In our study of 26 CBD cases, stones smaller than 10 mm were treated using this procedure. For a CBD diameter larger than 10 mm, first-stage closure of the CBD after stone removal not only avoided the T-tube, but also eliminated the possibility of bile leakage caused by T-tube removal in LCBDE. In our study, 75 patients underwent such a procedure, and no bile leakage or biliary tract stricture was reported.
In conclusion, the two reported procedures can be used for treating cholelithiasis with common bile duct stones. To decrease stone recurrence and biliary carcinoma incidence, which may be seen more often with EST, LC-LCBDE is the better choice, especially for young patients. Our current choice is LCBDE without a T-tube, or with a T-tube, through the cystic duct.
References
Collins C, Maguire D, Ireland A, Fitzgerald E, O’Sullivan GC (2004) A prospective study of common bile duct calculi in patients undergoing laparoscopic cholecystectomy: natural history of choledocholithiasis revisted. Ann Surg 239: 28–33
Fitzgobbons RJ, Gardner GC (2002) Laparoscopic surgery and the common bile duct.World J Surg 25: 1317–1324
Hong De-F, Gao M, Mou Yi-P, Cai Xiu-J, Wrs Br (2000) Study on laparoscopic cholecystectomy combined with intraoperative endoscopic sphinectomy and stone removal. Chin J Surg 38: 677–679
Hong De-F, Gao M, Wrs Br, Cai X-J, Mou Yi-P (2000) Intraoperative endoscopic sphincterotomy during laparoscopic cholecystectomy.World J Gastroenterol 6: 448–450
Hong De-F, LI Jun-D, Gao M, Yuan X-M, Wang Jian-G, Cai Xiu-J, Wang X-Fa (2003) One hundred and six cases analyses of laparoscopic technique combined with intraoperative cholangiogram and endoscopic sphincterotomy in sequential treatment of cholelithiasis. Chin J Gen Surg 15: 648–650
Larter DM, Froines EJ (2000) Laparoscopic common duct exploration in the management of choledocholithiasis. Am J Surg 179: 372–374
Mao J-Y, Chen X-R (2002) Diagnosis and mini-invasive treatment in extrahepatic duct stone.Hepatobiliary Surg 1: 73–74
Memon MA, Hassaballa H, Memmon MI (2000) Laparoscopic common bile duct exploration: the past, the present, and the future. Am J Surg 179: 309–315
Patel AP, Lokey JS, Harris JB, Sticca RP, McGill ES, Arrillaga A, Miller RS, Kopelman TR (2003) Current management of common bile duct stones in a teaching community hospital. Am Surg 69: 555–560
Pineres G, Yamakawa T, Kasugai H, Fukuda N, Ishiyama J, Sakai S, Maruno K, Miyajima N, Sunpaweravong S (1998) Common bile duct stones: management strategies in the laparoscopic era. Hepatobiliary Pancreat Surg 5: 97–103
Riciardi R, Islam S, Canete JJ, Arcand PL, Stoker ME (2003) Effective and long-term results of laparoscopic common bile duct exploration. Surg Endosc 17: 19–22
Sugiyama M, Atomi A (1999) Does endoscopic sphincterotomy cause prolonged pancreatobiliary reflux. Am J Gastroenterol 94: 795–797
Sugiyama M, Atomi Y (2002) Risk factors predictive of late complications after endoscopic sphincterotomy for bile duct stones: long-term (more than 10 years) follow-up study. Am J Gastroenterol 97: 2763–2767
Thompson MH, Tranter SE (2002) All-comers policy for laparoscopic exploration of the common bile duct. Br J Surg 89: 1608–1612
Tranter SE, Thompson MH (2002) Comparison of endoscopic sphincterotomy and laparoscopic exploration of the common bile duct. Br J Surg 89: 1495–1504
Tricarico A, Cione G, Sczio M, Di Palo P, Bottino V, Tricarico T, Tartaglia A, Iazzetta I, Sessa E, Mosca S, De Nucci C, Falco P (2002) Endolaparoscopic rendezvous treatment: a satisfying therapeutic choice for cholecysterctocholedocholithiasis. Surg Endosc 16: 585–588
Wei Q, Wang JG, Li LB, Li JD (2003) Management of choledocholithiasis: comparison between laparoscopic common bile duct exploration and intraoperative endoscopic sphincterotomy. World J Gastroenterol 9: 2856–2858
Wright BE, Freeman ML, Cumming JK, Quickel RR, Mandal AK (2002) Current management of common bile duct stones:is there a role for laparoscopic cholecystectomy and intraoperative endoscopic retrograde cholangiopancreatography as a single-stage procedure. Surgery 132: 729–737
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hong, DF., Xin, Y. & Chen, DW. Comparison of laparoscopic cholecystectomy combined with intraoperative endoscopic sphincterotomy and laparoscopic exploration of the common bile duct for cholecystocholedocholithiasis. Surg Endosc 20, 424–427 (2006). https://doi.org/10.1007/s00464-004-8248-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-004-8248-8